https://doi.org/10.14734/PN.2021.32.2.95 pISSN 2508-4887•eISSN 2508-4895
Rina Kim, MD1,
Mi-Young Lee, MD, PhD1, Lee Room Song, MD1, Seung A Choi, MD1, Jin Hoon Chung, MD, PhD1, Hye-Sung Won, MD, PhD1, Pil-Ryang Lee, MD, PhD1, Ellen Ai-Rhan Kim, MD, PhD2, Jae Suk Baek, MD, PhD3
1Department of Obstetrics and Gynecology, 2Division of Neonatology, Department of Pediatrics, 3Department of Pediatric Cardiology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
Fetal ventricular tachycardia (VT) is an extremely rare condition. Because sustained VT is highly associated with perinatal morbidity and mortality, prenatal management with antiarrhythmic drugs is crucial. A 33-year-old woman was referred to our hospital for fetal bradycardia at 25.2 weeks of gestation. Initial echocardiography showed bradycardia with irregular atrial beats, which was suspected as blocked atrial bigeminy. Four weeks later, the fetal tachycardia was accompanied by no atrioventricular conduction. Therefore, VT was diagnosed. The fetus developed hydrops. Despite the use of antiarrhythmic drug, the neonate died a few hours after birth because of persistent VT.
Only few cases of fetal VT have been reported worldwide, and no case has been reported in Korea.
Here, we report a case of fetal VT and discuss the prenatal management using antiarrhythmic drugs, reviewing previous reports.
Key Words: Arrhythmias, Congenital heart block, Prenatal diagnosis, Ventricular tachycardia
Introduction
Fetal ventricular tachycardia (VT) is an extremely rare disease and accounts for fewer than 2% of fetal tachycardia.1 VT can be diagnosed prenatally when the ventricular rate is faster than the atrial rate, with atrioventricular (AV) dissociation. Prenatal VT commonly occurs secondary to AV block, cardiac tumors, acute myocarditis, and hereditary ion channelopathies.2 Sustained tachycardia may cause fetal hydrops, preterm delivery, and associated with high perinatal morbidity and mortality.2 Therefore, prenatal diagnosis and management of VT are crucial. However, because only few cases of VT have been treated prenatally worldwide,1,3-9 and no case has been reported in Korea, treatment strategies have not yet been well established. Here, we report a case of fetal VT which was initiated from bradycardia and discuss the prenatal management using antiarrhythmic agents as in previously reported studies.
Case
A 33-year-old woman, gravida 2 para 1, was referred to our hospital at 25.2 weeks of gestation with suspected fetal bradycardia. The ultrasonographic findings showed a normal-sized fetus and normal range of amniotic fluid. The echocardiographic findings showed an atrial rate of 136-143 beats per minute (bpm) with a ventricular rate of 69-72 bpm (Fig. 1). When the intervals between the atrial systole for the first beat (A) and the next beat (A’) were measured, A to A’ intervals were 141-143 bpm and A’ to A intervals were 136-138 bpm. The A’ beat was regarded as the ectopic beat and was not conducted Received: 12 January 2021
Revised: 15 February 2021 Accepted: 17 February 2021 Correspondence to Mi-Young Lee, MD, PhD Department of Obstetrics and Gynecology, Asan Medical Center, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 05505, Korea
Tel: +82-2-3010-1829 Fax: +82-2-3010-6944
E-mail: [email protected] Copyright© 2021 by The Korean Society of Perinatology
This is an Open Access article distributed under the terms of the Creative Com- mons Attribution Non-Commercial License (http://creativecommons.org/
license/by-nc/4.0/), which permits unrestricted non-commercial use, distribution, and reproduction in any
Prenatal Diagnosis of Ventricular Tachycar
dia Initiated from Bradycardia
the arterial and venous Doppler were normal; cardiothoracic (CT) area was 0.31 (normal range, 0.2-0.3510); left ventricular fractional shortening (LV FS) was 0.60 (normal >0.2810); no evidence of valve regurgitations; the monophasic fillings were observed in the both ventricles. Therefore, the cardiovascular profile (CVP) score was 8. Due to the possibility of an AV
block, maternal autoantibodies including anti-Ro/SSA, anti-La/
SSB, and anti nuclear antibodies were checked, which were all negative. Maternal electrocardiography (ECG) also showed a normal sinus rhythm.
The patient was followed up every two weeks, and ultra- sonographic findings at 29.2 weeks of gestation showed that the
Fig. 1. M-mode echocardiographic image at 25.2 weeks of gestation showing the indicator line crossing the right ventricle and left atrium (upper column). The A to A’
intervals are shorter than A’ to A intervals, and ventricular contractions are not followed by every A’ beat, with an average rate of 69-72 beats per minute (bpm) (lower column).
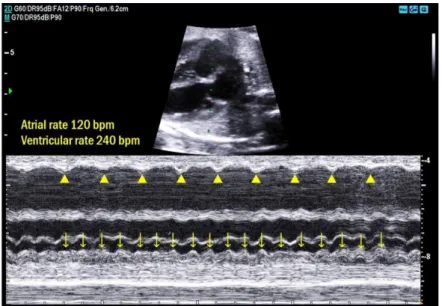
Fig. 2. M-mode echocardiographic image at 29.2 weeks of gestation showing the indicator line crossing the right atrium and left ventricle (upper column). The atrial rate was 120 beats per minute (bpm) (arrowheads) and the ventricular rate was 240 bpm (arrows), with atrioventricular dissociation (lower column).
reported so far.1,3-9,11-18 Most cases were intermittently asso- ciated with sinus bradycardia or AV block, whereas our case revealed that bradycardia was followed by VT. There was a gap in time between the occurrence of bradycardia and VT.
Because of this finding, it was difficult to predict the occurrence of VT, which may cause the delay in prenatal treatment and eventually lead to a poor outcome. The perinatal outcomes of 25 reported VT cases showed that 14 were managed from the prenatal period with a survival rate of 85.7% (12/14), while 11 were treated only in the postnatal period with a survival rate of 36.4% (4/11). Although our case showed a dismal prognosis despite the prenatal management, VT fetuses have been found to show better perinatal outcomes when treatment is initiated in the prenatal period.
At the time of the initial diagnosis, the ventricular rates were slower than atrial rates and the atrial-to-atrial activation (AA) intervals showed irregular short/long intervals. Therefore, we suspected that the premature atrial beats occurred continuously without conduction to the ventricles. After reviewing the images and videos of our case, we found that the findings were different from the typical BAB pattern: A’ beats (ectopic beats) are usually smaller than A beats in BAB, whereas the A’ beats were almost of the same size as the A beats in our case; furthermore, AA’ intervals are much shorter than A’A intervals in BAB, whereas our case had less prominent difference between AA’
and A’A intervals. The abovementioned findings are not always significant and, therefore, it is sometimes difficult to differentiate BAB from a 2:1 AV block. The differential diagnostic tips between BAB and 2:1 AV block are as follows: BAB has short/
long AA intervals, whereas 2:1 AV block has constant AA intervals,19 and the presence of maternal immune antibodies may help to rule out AV block. Although fetal magnetocardiography and ECG have been known to be helpful diagnostic tools for AV block, the clinical application of such modalities is still limited.2
Previous studies have documented that fetal onset of VT with AV block usually has a poor prognosis,3,6 and sustained VT with AV block can be strongly associated with long QT syndrome (LQTS).8 This is a hereditary disease and a leading cause of unexplained sudden death. It can also occur as de novo mutation. De novo LQTS has been reported to have a worse prognosis than inherited LQTS.20 For prenatal diagnosis of LQTS, magnetocardiography or ECG is required to measure fetus developed a fetal hydrops with ascites, pericardial effusion,
and pleural effusion. The echocardiographic findings showed an average atrial rate of 120 bpm and average ventricular rate of 240 bpm, with no relationship between atrial and ventricular contractions (Fig. 2). Therefore, VT was diagnosed. Besides, ductus venosus atrial flow was reversed; CT area was 0.41;
LV FS was 0.07; no evidence of valve regurgitations; and the monophasic fillings were still observed. Therefore, the CVP score was 5, suggestive of worsening cardiac function.
For conversion of the heart rate to normal, the patient was admitted on the same day. On the first day of hospitalization, maternal administration of digoxin was started at a dose of 0.5 mg every 12 hours for one day. Normal sinus rhythm was occasionally observed with an average ventricular rate of 155 bpm. The dosage of 0.25 mg was then maintained every 8 hours. However, VT more frequently occurred after 15 hours of digitalization. Besides, ventricular fibrillation also occurred.
A 4 g-loading dose of magnesium sulfate in 100 mL of dextrose 5% was administered intravenously over 20 minutes at a rate of 200 mL per hour. Soon after administration of magnesium sulfate, fetal distress was observed; therefore, an emergency cesarean section was performed under general anesthesia at 29.3 weeks of gestation. A female neonate with a bodyweight of 1.5 kg was born with an Apgar score of 1 at the 1 minute and 2 at the 5 minutes. Despite proper initial management, cardiopulmonary resuscitation was started with epinephrine injection because of pulseless electrical activity. Although a heart rate was detected upon resuscitation, ECG showed a mixture of persistent VT and ventricular fibrillation. Cardiac massage was repeated with defibrillation and administration of amiodarone as an antiarrhy thmic agent to terminate the tachycardia. However, she eventually died within four hours of birth.
Discussion
We reported a very unusual case of arrhythmia, i.e., VT, during the prenatal period: bradycardia was found without associated cardiac anomalies during the early period of gestation, and VT subsequently developed. Twenty-five cases of prenatally diagnosed VT without major cardiac abnormalities have been
Conflict of interest
No potential conflict of interest relevant to this article was reported.
References
1) Simpson JM, Maxwell D, Rosenthal E, Gill H. Fetal ventricular tachycardia secondary to long QT syndrome treated with maternal intravenous magnesium: case report and review of the literature. Ultrasound Obstet Gynecol 2009;34:475-80.
2) Donofrio MT, Moon-Grady AJ, Hornberger LK, Copel JA, Sklansky MS, Abuhamad A, et al. Diagnosis and treatment of fetal cardiac disease: a scientific statement from the American Heart Association. Circulation 2014;129:2183-242.
3) Hofbeck M, Ulmer H, Beinder E, Sieber E, Singer H. Prenatal findings in patients with prolonged QT interval in the neonatal period. Heart 1997;77:198-204.
4) Chang IK, Shyu MK, Lee CN, Kau ML, Ko YH, Chow SN, et al. Prenatal diagnosis and treatment of fetal long QT syndrome: a case report.
Prenat Diagn 2002;22:1209-12.
5) Cuneo BF, Ovadia M, Strasburger JF, Zhao H, Petropulos T, Schneider J, et al. Prenatal diagnosis and in utero treatment of torsades de pointes associated with congenital long QT syndrome. Am J Cardiol 2003;
91:1395-8.
6) Lin MT, Hsieh FJ, Shyu MK, Lee CN, Wang JK, Wu MH. Postnatal outcome of fetal bradycardia without significant cardiac abnormalities. Am Heart J 2004;147:540-4.
7) Horigome H, Nagashima M, Sumitomo N, Yoshinaga M, Ushinohama H, Iwamoto M, et al. Clinical characteristics and genetic background of congenital long-QT syndrome diagnosed in fetal, neonatal, and infantile life: a nationwide questionnaire survey in Japan. Circ Arrhythm Electrophysiol 2010;3:10-7.
8) Anuwutnavin S, Wanitpongpan P, Chungsomprasong P, Soongswang J, Srisantiroj N, Wataganara T. Fetal long QT syndrome manifested as atrioventricular block and ventricular tachycardia: a case report and a review of the literature. Pediatr Cardiol 2013;34:1955-62.
9) Miyoshi T, Sakaguchi H, Shiraishi I, Yoshimatsu J, Ikeda T. Potential utility of pulsed-wave Doppler for prenatal diagnosis of fetal ventricular tachycardia secondary to long QT syndrome. Ultrasound Obstet Gynecol 2018;51:697-9.
10) Huhta JC. Fetal congestive heart failure. Semin Fetal Neonatal Med 2005;10:542-52.
11) Lopes LM, Cha SC, Scanavacca MI, Tuma-Calil VM, Zugaib M. Fetal idiopathic ventricular tachycardia with nonimmune hydrops: benign course. Pediatr Cardiol 1996;17:192-3.
12) Manning N, Anthony JP, Ostman-Smith I, Snyder CS, Burch M. Prenatal diagnosis and successful preterm delivery of a fetus with long QT the QT interval. However, because the modalities are rarely
used in our center, we could not evaluate QT prolongation in the prenatal period. Furthermore, because the neonate showed persistent VT and ventricular fibrillation on ECG and died soon after birth, it was not possible to assess for associated LQTS.
There was no family history of sudden death, and ECG findings of her family members (the parents and the older brother) showed no evidence of QT prolongation. Nevertheless, based on the pattern of fetal arrhythmia and the poor prognosis, our case may have had LQTS.
When VT is sustained, proper management with antiarrhy- thmic drugs during pregnancy is essential. However, due to the rarity of fetal VT, there is still limited consensuses about optimal therapy. Several antiarrhythmic drugs, such as Na+ channel blockers (amiodarone, flecainide, lidocaine, and mexiletine), beta blockers (propranolol and sotalol), digoxin, and magnesium sulfate have all been used for the treatment of VT.1 The choice of drug depends on the presence of LQTS. When VT is associated with LQTS, the first-line drugs include magnesium sulfate, lidocaine, and propranolol.1,2,8 Magnesium reduces the occurrence of and eliminates early after-depolarization.5 Lidocaine can reduce the risk of premature excitation in Na+ channelopathies.4 Besides, propranolol can reduce the fre- quency of VT.1,3,4 In the presence of LQTS, drugs that have QT-prolonging potentials, such as sotalol, amiodarone, and flecainide, should be avoided because those can aggravate tachycardia.2,5 When LQTS is excluded, sotalol, amiodarone, and flecainide can be used, resulting in the successful resolution of VT.2 Digoxin was used as the first-line drug in our case and did not result in termination of VT even when the therapeutic level was achieved; we then started intravenous magnesium sulfate as the second-line drug. Unfortunately, before any further effect was observed, the fetal condition deteriorated rapidly, necessitating emergent delivery. After birth, although amiodarone was administrated intravenously, it did not have an effect.
In conclusion, we emphasize the importance of correct prenatal diagnosis of fetal arrhythmia and proper perinatal management. When VT is suspected, close fetal surveillance is necessary and antiarrhythmic drugs should be carefully chosen considering the possibility of associated LQTS.
syndrome. BJOG 2000;107:1049-51.
13) Beinder E, Grancay T, Menéndez T, Singer H, Hofbeck M. Fetal sinus bradycardia and the long QT syndrome. Am J Obstet Gynecol 2001;185:
743-7.
14) Duke C, Stuart G, Simpson JM. Ventricular tachycardia secondary to prolongation of the QT interval in a fetus with autoimmune mediated congenital complete heart block. Cardiol Young 2005;15:319-21.
15) Das B, Cuneo BF, Ovadia M, Strasburger JF, Johnsrude C, Wakai RT.
Magnetocardiography-guided management of an unusual case of isoimmune complete atrioventricular block complicated by ventricular tachycardia. Fetal Diagn Ther 2008;24:282-5.
16) Horigome H, Iwashita H, Yoshinaga M, Shimizu W. Magnetocardio- graphic demonstration of torsade de pointes in a fetus with congenital long QT syndrome. J Cardiovasc Electrophysiol 2008;19:334-5.
17) Saileela R, Sachdeva S, Saggu DK, Koneti NR. Ventricular tachycardia in a fetus: benign course of a malignant arrhythmia. J Obstet Gynaecol India 2019;69:383-6.
18) Vaksmann G, Lucidarme S, Henriet E. Fetal ventricular tachycardia:
betablockers should be the first line treatment. J Gynecol Obstet Hum Reprod 2020 Oct 15 [Epub]. https://doi.org/10.1016/j.jogoh.2020.
101946.
19) Eliasson H, Wahren-Herlenius M, Sonesson SE. Mechanisms in fetal bradyarrhythmia: 65 cases in a single center analyzed by Doppler flow echocardiographic techniques. Ultrasound Obstet Gynecol 2011;37:
172-8.
20) Strand S, Strasburger JF, Cuneo BF, Wakai RT. Complex and novel arrhythmias precede stillbirth in fetuses with de novo long QT syndrome.
Circ Arrhythm Electrophysiol 2020;13:e008082.