Implementation of Chest X-ray Observation Report Entry System
Suk-Tae Seo, PhD1, Hee-Joon Park, PhD2, Min Soo Kim, PhD1, Chang-Sik Son, PhD3, Hyoung-Seob Park, MD, MS4, Hyo Chan Jeon, PhD5, Chi Young Jung, MD, PhD4, Yoon-Nyun Kim, MD, PhD4
1Biomedical Information Technology Center, Keimyung University; Departments of 2Biomedical Engineering, 3Medical Informatics, and 4Internal Medicine, Keimyung University School of Medicine; 5Institute of Medical Information, MDware Co. Ltd., Daegu, Korea
Objectives: X-rays are widely used in medical examinations. In particular, chest X-rays are the most frequent imaging test.
However, observations are usually recorded in a free-text format. Therefore, it is difficult to standardize the information pro- vided to construct a database for the sharing of clinical data. Here, we describe a simple X-ray observation entry system that can interlock with an electronic medical record system. Methods: We investigated common diagnosis indices. Based on the indices, we have designed an entry system which consists of 5 parts: 1) patient lists, 2) image selection, 3) diagnosis result en- try, 4) image view, and 5) main menu. The X-ray observation results can be extracted in an Excel format. Results: The useful- ness of the proposed system was assessed in a study using over 500 patients' chest X-ray images. The data was readily extract- ed in a format that allowed convenient assessment. Conclusions: We proposed the chest X-ray observation entry system. The proposed X-ray observation system, which can be linked with an electronic medical record system, allows easy extraction of standardized clinical information to construct a database. However, the proposed entry system is limited to chest X-rays and it is impossible to interpret the semantic information. Therefore, further research into domains using other interpretation methods is required.
Keywords: Chest X-ray, Electronic Medical Record, Standardized Clinical Information, Entry System, Picture Archiving and Communication System
Healthc Inform Res. 2010 December;16(4):305-311.
doi: 10.4258/hir.2010.16.4.305 pISSN 2093-3681 • eISSN 2093-369X
Received for review: November 4, 2010 Accepted for publication: December 23, 2010 Corresponding Author
Yoon-Nyun Kim, MD, PhD
Department of Internal Medicine, Keimyung University School of Medicine, 194 Dongsan-dong, Jung-gu, Daegu 700-712, Korea. Tel:
+82-53-250-7432, Fax: +82-53-580-3745, E-mail: [email protected]
This is an Open Access article distributed under the terms of the Creative Com- mons Attribution Non-Commercial License (http://creativecommons.org/licenses/by- nc/3.0/) which permits unrestricted non-commercial use, distribution, and reproduc- tion in any medium, provided the original work is properly cited.
ⓒ 2010 The Korean Society of Medical Informatics
I. Introduction
X-rays have been widely used in medical examinations since their discovery by Wilhelm Conrad Roentgen in 1895 [1].
Various other medical imaging methods, such as computed tomography (CT), magnetic resonance imaging (MRI), and positron emission tomography (PET) have been developed and have replaced the use of X-ray imaging for some func- tions. However, X-ray remains the most common medical imaging tool. Especially, the chest X-ray, which reveals the lungs, heart, and bones, is one of the most common chest imaging protocols. The advent and advances in computer technology have spurred interest in the exchange of medical record between medical centers and more effective manage- ment of medical records using computers and communi- cation systems. Based on the interests, electronic medical record (EMR) systems and picture archiving and communi-
cation systems (PACSs) have been proposed [2,3].
Despite the allure of computation data collection, exchange, and management, X-ray information is still collected as nar- rative reports in free-text form [4,5]. Electronic standardiza- tion and exchange of X-ray clinical information effectively requires the interlocking of the standardized chest X-ray ob- servation system with PACS and/or EMR. Natural language processing [4-6] and standardized methods such as clinical model-based [7-10], have been proposed. However it is often difficult to use and/or need improvement in various cases [7].
Therefore, to simplify the exchange of clinical X-ray diag- nosis information according to patients and to standardize the diagnosis report form, we herein propose a simple X-ray observation entry system that can be interlocked with EMR and PACS. The proposed system consists of patient lists, an observation result entry component composed of radio but- tons and a chest X-ray image view module. Using this chest X-ray observation entry system, it is possible to extract the observation results in an Excel format, which enables both construction of a data mart and further research using com- puter-aided decision tools.
The rest of this paper is organized as follows: In section 2, we show the composition of the proposed entry system. In section 3, we show the implemented entry system, and, fi- nally, In section 4 concludes this paper.
II. Case Description
1. Conventional Methods
The conventional EMR system is based on free-text. There- fore, it is impossible to reuse and/or exchange the medical information. To overcome this drawback, structured entry support systems have been proposed and studied. The key purpose of these methods is to construct structured data set for effective medical information exchange and practi- cal clinical data creation. In this paper, we provide an over- view of two typical methods: the natural language-based method (also known as symbolic text processor, or SymText [5,11,12], and the clinical model-based method (also known as openEHR) [10,13].
1) Natural language-based method
Natural language processing (NLP) allows a machine to be able to read and learn text [11,12]. Methods based on NLP to extract information from EHRs have been proposed [4- 6]. SymText, which is proposed Koehler [5], is one of them.
The purpose of SymText is to construct structured data that enables diagnostic systems to be used for medical decision making and alerting systems.
However SymText improvements are still needed in lexicon, grammar, and transformation. Presently, SymText is not ac- curate enough, especially on unclear reports, to be used to automatically generate the characteristics.
2) Clinical model-based
The brief description of archetypes and templates of openEHR is as follow [10,13].
An archetype is a re-usable, formal model of a domain concept. Archetypes are used to create detailed clinical models of for example observations like blood pressure or a specific laboratory results, information related to the evaluation of a clinical problem, related to activities like prescribing of medications etc.
The openEHR templates are used to adjust and combine archetypes for specific use cases and local needs. Templates are connected to entry forms (documentation templates), and may be bound to terminologies [14].
The purpose of overall researches and tools is to develop structured data set in some specific medical fields. According to the need, we propose an X-ray observation entry program which is possible to interlock with EMR and PACS. More- over, using the proposed system, observational mistakes can be reduced because the system consists of radio button type and/or structured type entry system. Sometimes, even clini- cal experts can err in reading text without considering the characteristics of some diseases. However, the proposed sys- tem provides the two entry routes for various diseases, which reduces mistakes. Furthermore, the system is applicable to construction of a data mart for clinical research, health in- formation exchange, and constructing content-based system, and etc.
2. Description of Chest X-ray Entry System
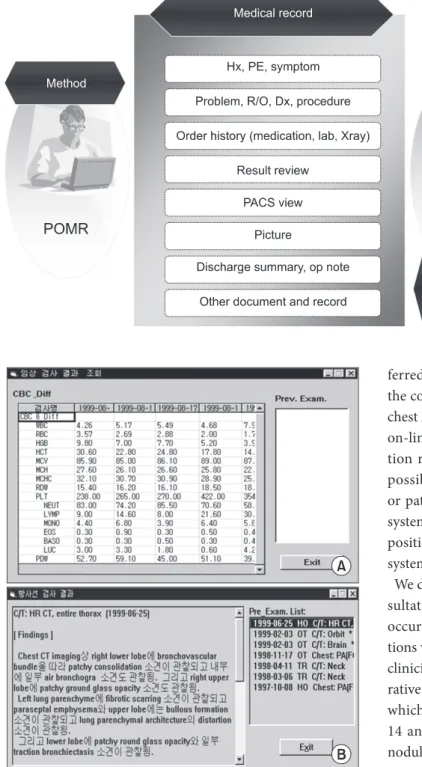
Medical record is a document of a patient's medical history that contains diagnosis information, results of treatments, laboratory results, and radiology report, among other infor- mation. The typical elements of medical records of D hospi- tal in Daegu city are listed in Figure 1.
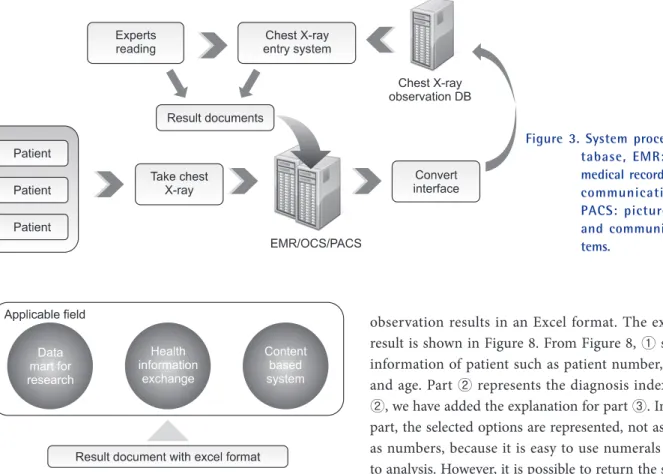
However, current EMRs have different types of archi- tectures and terminologies that vary from one hospital to another. Therefore, exchange of data is onerous, given the lack of standardization. Moreover, observation reports for medical radiology images such as X-ray, CT, and MRI are typically written in a narrative way, which is different from laboratory results, as shown in Figure 2.
Laboratory results are presented in a way that is readily in-
terpretable by clinicians, and can be directly stored as a com- puter file (Figure 2). However, in case of an observation re- port for radiology, such direct conversion to a computer file is onerous, if not impossible, and data exchange is hobbled by the free text form of the information.
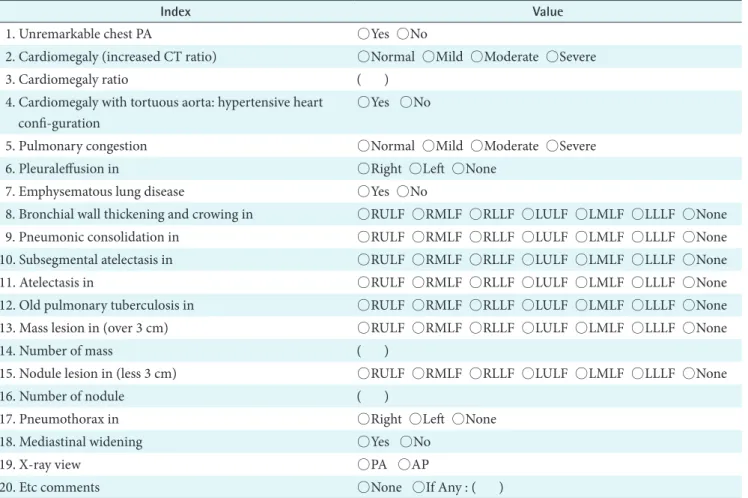
Presently, we propose a simple chest X-ray entry system.
The system process is diagrammed in Figure 3.
Firstly, chest X-ray images according to patients are trans-
ferred into the chest X-ray observation data mart through the conversion interface. Secondly, clinical experts check the chest X-ray on-line using the proposed entry system through on-line, and the checked image is stored with the observa- tion results. Searching for the data of a specific patient is possible using an identifier such as patient number and/
or patient name. Moreover the proposed chest X-ray entry system has various applicable fields such as data mart com- position, health record exchange, and other contents-based systems (Figure 4).
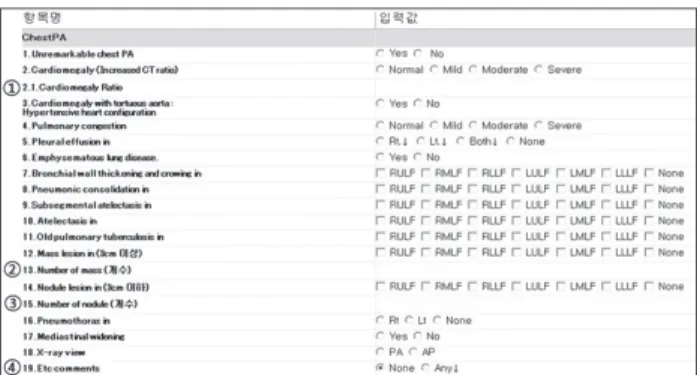
We designed chest X-ray observation indexes based on con- sultations with clinical experts. Significant and frequently occurring indexes were selected, and the values of input op- tions were designed with items that would be recognizable to clinicians (Table 1). Parts 3, 14, 16, and 20 are the short nar- rative parts. In part 3, the real value of cardiothoracic ratio, which is used to diagnosis cardiomegaly, is inputted. Parts 14 and 16 are where the observed number of masses and nodules, respectively, are entered. Part 20 is for the input of any comments. To specify the regions where unusual states exist, the chest region was divided into seven parts, as shown in from indexes 8-13 and 15. In the indexes, RULF, RMLF, RLLF, LULF, LMLF, and LLLF stand for right upper lung field, right middle lung field, right low lung field, left upper lung field, left middle lung field, and left low lung field, re- spectively.
III. Results
In this section, we show configuration of the implemented system. The implemented chest X-ray entry system consists Figure 1. Medical record elements.
POMR: problem-oriented medical record, Hx: history, PE: physical examination, R/O: rule out, OP: op- eration, SOAP: subjective- objective-asessment-plan.
Figure 2. Example of results report. (A) Laboratory result. (B) Ob- servation report.
of five parts as shown in Figure 5.
The configurated implemented chest X-ray entry system consists of five parts (Figure 5). ① represents the informa- tion of patients such as patient number, name, and sex.
② shows the list of the chest X-ray images according to patients. ③ shows the diagnosis indexes and input options.
④ represents the image selected in part ②. ⑤ is the main menu. Using the sub-menus of part ⑤, it is possible to edit the index and input options, to extract observation result as excel format, and to search specific patient's chest X-ray with result. Figure 6 shows an example of a search result for one patient.
Based on the Table 1, we have implemented detail indexes and input options as shown in Figure 7. Parts ①, ②, ③, and
④ are narrative parts. In case of part ①, the diagnostic cri- teria could differ according to clinical experts. Therefore, we made the free-text part to clarify the ratio of cardiothoracic ratio (CTR), which is used in the diagnosis. Moreover, if any other comments exist for the given chest X-ray image, the clinical expert(s) can write the extra comments in index 19 by selecting the "Any" option.
To verify the observation results, it is possible to save the
observation results in an Excel format. The example of a result is shown in Figure 8. From Figure 8, ① shows basic information of patient such as patient number, name, sex, and age. Part ② represents the diagnosis indexes. In part
②, we have added the explanation for part ③. In the results part, the selected options are represented, not as words, but as numbers, because it is easy to use numerals in analyses to analysis. However, it is possible to return the selected op- tions to words if necessary.
Although the proposed chest X-ray observation entry sys- tem is convenient and can be used in various applications, the proposed system is limited to chest X-rays. Moreover, it is as yet unable to interpret semantic information. Therefore, to improve the quality and applicability of system, more research on techniques such as X-ray, CT, and MRI of the abdomen is required.
IV. Discussion
Although various other medical imaging techniques have been proposed, such as CT, MRI, and positron emission to- mography, the X-ray (especially the chest X-ray) is the most common and widely used examination method in medicine.
Especially, chest X-ray, which is used to evaluate normality of organs inside chest such as lungs, heart, bones, and etc., is one of them. The development of PACS and EMR systems has spurred interest in the exchange of medical records between medical centers. However, the free text format of most medical reports hinders this goal. Therefore, to extract medical information automatically from the reports, various methods based on natural language processing have been proposed. In other cases, to create encoded and structured data, studies examining clinical content have been under- taken. However, the techniques are rudimentary and remain
Figure 3. System process. DB: da- tabase, EMR: electronic medical record, OCS: order communication system, PACS: picture archiving and communication sys- tems.
Figure 4. Applicable field of observation results using the pro- posed entry system.
difficult to use by clinical experts and/or need to improve in various cases.
Therefore, in this study, we have proposed a chest X-ray ob- servation entry system that can be interlocked with hospital EMR and PACS systems. Using the entry system, we were able to collect data in a simplified and standardized form.
Moreover, the proposed system is useful in constructing data
marts that are large enough to interlock with EMR and PACS systems. Another advantage of the proposed entry system is its ability to reduce mistakes while checking the chest X-ray.
In some cases, clinical experts can make a diagnosis without due attention to X-ray findings. However, because the pro- posed system shows representative lists for diagnosis, such a mistake could be reduced. Moreover, because the proposed Table 1. The designed index and input options according to indexes
Index Value
1. Unremarkable chest PA ○Yes ○No
2. Cardiomegaly (increased CT ratio) ○Normal ○Mild ○Moderate ○Severe
3. Cardiomegaly ratio ( )
4. Cardiomegaly with tortuous aorta: hypertensive heart confi-guration
○Yes ○No
5. Pulmonary congestion ○Normal ○Mild ○Moderate ○Severe
6. Pleuraleffusion in ○Right ○Left ○None
7. Emphysematous lung disease ○Yes ○No
8. Bronchial wall thickening and crowing in ○RULF ○RMLF ○RLLF ○LULF ○LMLF ○LLLF ○None 9. Pneumonic consolidation in ○RULF ○RMLF ○RLLF ○LULF ○LMLF ○LLLF ○None 10. Subsegmental atelectasis in ○RULF ○RMLF ○RLLF ○LULF ○LMLF ○LLLF ○None
11. Atelectasis in ○RULF ○RMLF ○RLLF ○LULF ○LMLF ○LLLF ○None
12. Old pulmonary tuberculosis in ○RULF ○RMLF ○RLLF ○LULF ○LMLF ○LLLF ○None 13. Mass lesion in (over 3 cm) ○RULF ○RMLF ○RLLF ○LULF ○LMLF ○LLLF ○None
14. Number of mass ( )
15. Nodule lesion in (less 3 cm) ○RULF ○RMLF ○RLLF ○LULF ○LMLF ○LLLF ○None
16. Number of nodule ( )
17. Pneumothorax in ○Right ○Left ○None
18. Mediastinal widening ○Yes ○No
19. X-ray view ○PA ○AP
20. Etc comments ○None ○If Any : ( )
PA: posterior-anterior, CT: computed tomography, AP: anterior-posterior, RULF: right upper lung field, RMLF: right middle lung field, RLLF: right low lung field, LULF: left upper lung field, LMLF: left middle lung field, LLLF: left low lung field.
Figure 5. The configuration of the proposed system. Figure 6. Example of searching for specific patient.
entry system consists of radio buttons according to indexes, it is convenient and user-friendly.
Nonetheless of the advantage of the proposed entry system, it is limited to interpret semantic information from the ob- servation results. Therefore the expended researches based on the entry system in various other fields are required to extract semantic information.
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Acknowledgements
This research was supported by the grant No. RTI04-01-01 from the Regional Technology Innovation Program of Min- istry of Knowledge Economy (MKE).
References
1. Röntgen W. Über eine neue art von strahlen. In: Sit- zungsberichte der Physikalisch-Medicinisch Gesell- schaft zu Würzburg; 1895. p132-141.
2. Anderson D, Flynn K. Picture archiving and communi- cation systems: a systematic review of published stud- ies of diagnostic accuracy, radiology work processes, outcomes of care, and cost. Technology Assessment Program: Report no. 5. Boston, MA: Veterans Health Administration’s Office of Research and Development;
1997.
3. Whittick D, Gill S. Diagnostic imaging electronic health record (DI/EHR) challenges-strategy and planning per- spective. In: 24th International EuroPACS Conference;
2006 June 15-17; Trondheim, Norway.
4. Hripcsak G, Friedman C, Alderson PO, DuMouchel W, Johnson SB, Clayton PD. Unlocking clinical data from narrative reports: a study of natural language process- ing. Ann Intern Med 1995; 122: 681-688.
5. Koehler SB. Symtext: a natural language understanding system for encoding free text medical data [dissertation].
Salt Lake, UT: The University of Utah; 1998.
6. Meystre S, Haug PJ. Automation of a problem list using natural language processing. BMC Med Inform Decis Mak 2005; 5: 30.
7. Leslie H, Heard S, Garde S, McNicoll I. Engaging clini- cians in clinical content: herding cats or piece of cake?
Stud Health Technol Inform 2009; 150: 125-129.
8. Beale T, Heard S. OpenEHR release 1.0.1: archetype definitions and principles [Internet]. London: The OpenEHR Foundation; c2003-2007 [cited at 2010 Dec 10]. Available from: http://www.openehr.org/svn/speci- fication/TRUNK/publishing/architecture/am/arche- type_principles.pdf.
9. Garde S, Knaup P, Hovenga E, Heard S. Towards seman- tic interoperability for electronic health records. Meth- ods Inf Med 2007; 46: 332-343.
10. Bernstein K, Tvede I, Petersen J, Bredegaard K. Can openEHR archetypes be used in a national context? The Danish archetype proof-of-concept project. Stud Health Technol Inform 2009; 150: 147-151.
11. Lapata M, Keller F. The Web as a baseline: evaluating the performance of unsupervised web-based models for a range of NLP tasks. In: Proceedings of the Human Language Technology Conference of the North Ameri- can Chapter of the Association for Computational Linguistics: HLT-NAACL 2004; 2004 May 2-7. Boston, MA: Human Language Technology Conference/North American Chapter of the Association for Computational Linguistics; 2004.
12. Charniak E, Knight K, Yamada K. Syntax-based lan- guage models for statistical machine translation. In:
Proceedings of MT Summit IX; 2003 Sept 23-27. New Figure 8. Results extraction as excel format.
Figure 7. Implemented indexes and input options.
Orleans, LA: International Association for Machine Translation; 2005.
13. OpenEHR Foundation. Clinical knowledge manager [Internet]. London, UK: OpenEHR Foundation; c2010 [cited at 2010 Dec 14]. Available from: http://www.
openehr.org/knowledge.
14. Bernstein K, Andersen U. Managing care pathways combining SNOMED CT, archetypes and an electronic guideline system. Stud Health Technol Inform 2008;
136: 353-358.