44
서 론
담도암 환자의 초기 증상은 황달인 경우가 많은데1 황달 에 의한 간 기능 저하 및 이에 따른 수술 후 합병증의 위험 때문에 수술 전 담도 배액술을 시행하는 경우가 있지만 이 의 효용성에 대해서는 회의적인 결과를 보이는 연구 결과 가 많이 발표되고 있다.2,3 본 연구는 황달을 주소로 본원을 방문하여 원위 담도암 진단 하에 췌십이장절제술을 시행 받은 환자에서 수술 전 담도 배액술을 시행한 후 혈청 총 빌리루빈이 감소하는 속도에 따라 수술 후 합병증 발생률 및 수술 사망률에 차이가 있는지를 알아보고자 하였다.
방 법
1996년 6월부터 2004년 4월까지 본원에서 원위 담도암 진단 하에 췌십이지장절제술을 시행받은 46명의 환자를 대 상으로 의무기록을 이용한 후향적인 연구를 하였다. 각 환 자의 나이, 성별, 당뇨 여부 등을 확인하였고, 수술 전 담도 배액시행여부, 내원 당시와 수술 직전 혈청 빌리루빈, 수술 전 혈청 알칼리 인산효소(alkaline phosphatase, ALP), 알부 책임저자:이건영, 인천광역시 중구 신흥동 3가 7-206
ꂕ 400-711, 인하대학교 의과대학 외과학교실 Tel: 032-890-2738, Fax: 032-890-3097 E-mail: 196087@inha.ac.kr
제21차 한국간담췌외과학회 추계학술대회에서 구연발표되었음.
Correlations between the Rate of Decrease in Pre- operative Bilirubin and Postoperative Complications after Biliary Drainage for Distal Common Bile Duct Cancer
Eung-Ho Cho, M.D., Keon-Young Lee, M.D., Sun Keun Choi, M.D., Yoon Seok Hur, M.D., Sei Joong Kim, M.D., Young Up Cho, M.D., Seung-Ik Ahn, M.D., Kee-Chun Hong, M.D., Seok- Hwan Shin, M.D., Kyung Rae Kim, M.D. and Ze-Hong Woo, M.D.
Department of Surgery, Inha University College of Medicine, Incheon, Korea
Purpose: This study was aimed at comparing the rate of decrease in preoperative serum bilirubin after biliary drainage and the postoperative complication rate in patients with distal common bile duct (CBD) cancer.
Methods: Forty six patients who had undergone pancreati- coduodenectomy due to distal CBD cancer were included in this study. The patients were divided into the complicated and uncomplicated groups. For the patients who underwent pre- operative biliary drainage, the preoperative bilirubin level and the rate of decrease in serum bilirubin were measured and compared between the two groups.
Results: The postoperative complication and mortality rates were 43.4% (20/46) and 6.5% (3/46), respectively. The com- plication rates were not different between the drainage and non-drainage groups (p=0.48). The preoperative serum biliru- bin levels were also not different between the complicated and uncomplicated groups (p=0.214). In the uncomplicated group, the rate of decrease in the serum total bilirubin level tended to be higher than in the complicated group, but this was not statistically significant (mean: 0.82 vs 0.27 mg/dl/day, respectively, p=0.117). Patients with a higher preoperative bilirubin decrease rate showed a larger bilirubin decrease in the immediate postoperative period (from POD 1 to POD 7,
원위 담도암에서 수술 전 담도 배액 후 총 빌리루빈의 감소 속도와 수술 결과와의 상관관계
인하대학교 의과대학 외과학교실
조응호․이건영․최선근․허윤석․김세중․조영업․안승익․홍기천․신석환․김경래․우제홍
r=0.371, p=0.05).
Conclusion: The preoperative biliary drainage and the serum bilirubin level were not correlated with the postoperative complication rate. Patients with higher preoperative bilirubin decrease rates showed a larger bilirubin decrease in the immediate postoperative period, which can be interpreted as having a faster recovery of their liver function. Further study with a larger number of cases is required to see if the preoperative bilirubin decrease rate could be used as a prognostic indicator after pancreaticoduodenectomy. (Korean J HBP Surg 2005;9:44-48)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Key Words: Drainage
Bilirubin Rate
Pancreaticoduodenectomy
중심 단어: 배액, 빌리루빈, 속도, 췌십이지장절제술
민, 혈색소, 크레아티닌 수치 등을 기록하였고, 수술 후 1일, 7일, 14일째 각각의 혈청 빌리루빈 수치를 확인하여 감소 추세를 확인하였다. 수술 전 담도 배액을 시행한 경우 빌리 루빈의 감소속도((배액 전 빌리루빈치- 배액 후 빌리루빈 치)/배액 기간, mg/dl/day)를 확인하였다. 수술 후 2주가 경 과한 후 복강 배액관을 통한 배액 물에서 아밀라제 수치가 높은 수준으로 확인되는 경우를 췌공장문합부 누출(pan- creaticojejunal leak)이 발생한 합병증으로 정의하였고4,5 수 술 후 30일 이내에 사망한 경우 수술 후 사망으로 정의하였 다. 통계 처리는 Windows 용 SPSS 11.5를 이용하여 비교대 상이 적은 경우 비모수 검정(chi square test, Kruskal- Wallis test)을 실시하였고 빌리루빈 감소속도 간의 상관분석시는 모수 검정(Pearson's correlation test)을 실시하였다. p-value는 0.05 이하일 경우 통계적인 유의성이 있는 것으로 판정하였 다.
결 과
환자의 평균 나이는 62.3세(범위 35∼75세), 남자는 36명, 여자가 10명이었다. 수술은 표준 휘플 수술(Whipple's oper- ation)이 26명, 유문 보존 췌십이장절제술(pylorus preserving pancreaticoduodenectomy, PPPD)가 20명에서 시행되었는데, 휘플 수술 환자 중 2명에서 암세포의 좌측 간 내 담도 침범 이 발견되어 간 좌엽절제술을 동시에 실시하였다(hepatico- pancreaticoduodenectomy, HPD)(Table 1). 총 46명의 환자 중 수술 후 합병증이 발생한 환자는 20명이었으며(43.4%) 이 중 수술 후 사망은 3명(6.5%)이었는데 합병증 및 사망원인 은 Table 2와 같다.
환자의 성별 혹은 당뇨 유무에 따라서 합병증 발생률에 차이가 없었으며 총 46명의 환자 중 수술 전 담도 배액 술을
시행 받은 환자는 36명이었는데 내시경적 경비 담관배액술 (Endoscopic nasobiliary drainage, ENBD)이 24명 그리고 경피 경간 담도배액술(Percutaneous transhepatic biliary drainage, PTBD)이 12명에서 시행되었다(Table 1). 배액군과 비 배액 군 간에도 합병증 발생률의 통계적인 차이는 없었다(Table 3).
합병증 발생환자와 합병증이 발생하지 않은 환자들 사이 에 수술 직전 혈청 빌리루빈 수치, 수술 전 혈청 알칼리 인 산효소, 알부민, 혈색소, 크레아티닌 수치, 그리고 수술 중 적혈구 수혈량 및 수술 시간사이에 통계적인 차이는 없었 다(Table 4).
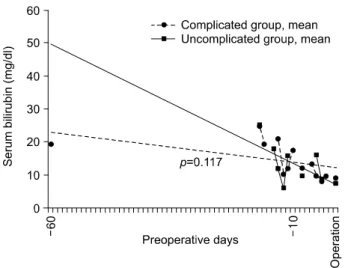
담도 배액 환자군에서 1일당 혈청 빌리루빈의 감소속도는 평균 0.57 mg/dl/day (-3.5∼1.58 mg/dl/day)였는데, 담도 배 액 환자군 중 수술 후 정상 회복군에서 합병증 발생 환자군 보다 혈청 빌리루빈 감소 속도가 더 빠른 경향을 보였으나 통계적인 차이는 없었다(Table 4, Fig. 1). 수술 후 1일 혈청 빌리루빈 수치는 합병증 발생군과 정상 회복군간에 차이가 없었으나 수술 후 7, 14일에 각각 정상 회복군에서 더 빨리 감소하였다(p=0.017, 0.002). 또한 수술 후 1∼7일의 빌리루 빈 감소는 정상 회복군에서 유의하게 빨랐다(p=0.015) (Table 4, Fig. 2). 담도 배액 환자군의 혈청 빌리루빈 감소속
Table 1. Patients information
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Age (years) 62.3±10.12
Sex (M:F) 36:10
Underlying disease Diabetes mellitus 8
Preoperative Not done 10
biliary drainage Done 36
PTBD* 12
ENBD† 24
Operation Whipples' operation 24
PPPD‡ 20
HPD§ 2
(all left hepatic lobectomy) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*PTBD = percutaneous transhepatic biliary drainage; †ENBD = endoscopic nasobiliary drainage; ‡PPPD = pylorus preserving pan- creaticoduodenectomy; §HPD = hepaticopancreaticoduodenectomy.
Table 2. Complication and mortality
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Complication Total 20 (43.4%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Pancreatic fistula 5 (10.1%) Intraperitoneal abscess 6 (13.4%)
Bleeding 7 (15.2%)
Pulmonary complication 2 (4.3%) Biliary leak 1 (2.2%) Pancreatitis 1 (2.2%) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Operative mortality Total 3 (6.5%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Bleeding 2
Sepsis 1
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
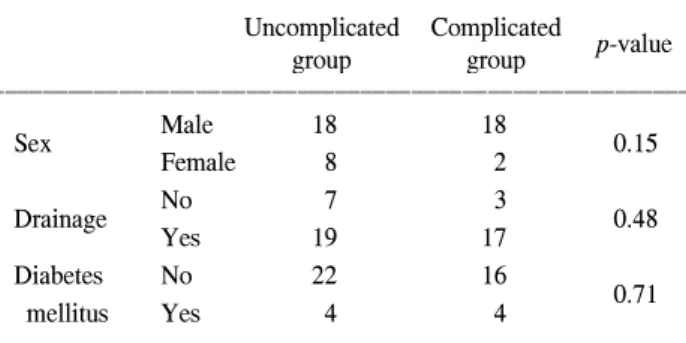
Table 3. Risk factors for complications (chi-square test) ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Uncomplicated Complicated
p-value
group group
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Male 18 18
Sex 0.15
Female 8 2
No 7 3
Drainage 0.48
Yes 19 17
Diabetes No 22 16
mellitus Yes 4 4 0.71
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Table 4. Risk factors for complications (Kruskal-Wallis test)
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ Mean (range)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ p-value Uncomplicated group Complicated group
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Age (years) 60.55 (35∼75) 64.50 (44∼76) 0.214
Initial serum bilirubin (mg/dl) 12.4 (1.4∼39.1) 13.4 (2.2∼24.9) 0.508
Preop. bilirubin (mg/dl) 6.40 (0.7∼15.6) 8.17 (0.3∼17) 0.214
Preop. biliary drainage
7.5 (3∼13) 11.4 (2∼60) 0.238
duration (days)
Bilirubin decrease rate* (mg/dl/day) 0.82 (0.06∼1.58) 0.27 (-3.5∼1.34) 0.117
Preop. ALP (IU/L) 713.00 (210∼2403) 642.15 (108∼1926) 0.773
Preop. albumin (g/dl) 3.40 (2.5∼3.9) 3.41 (2.3∼4.3) 0.947
Preop. creatinine (mg/dl) 0.81 (0.3∼1.4) 0.82 (0.5∼1.1) 0.603
Preop. hemoglobin (g/dl) 11.62 (8.2∼14.1) 12.48 (9.1∼14.5) 0.090
Intraoperative RBC
461.50 (0∼1600) 700 (0∼2200) 0.136
transfusion (ml)
Operation time (min) 491.20 (300∼780) 514.50 (360∼780) 0.442
Serum bilirubin POD1 (mg/dl) 5.31 (0.7∼12.8) 5.55 (1.1∼10.3) 0.572
Serum bilirubin POD7 (mg/dl) 3.81 (0.4∼15.9) 6.64 (0.9∼15.1) 0.017
Serum bilirubin POD14 (mg/dl) 2.00 (0.2∼6.3) 6.52 (1.0∼17.1) 0.002
Postop. bilirubin decrease (POD 1∼7)† 1.49 -1.11 0.015
Postop. bilirubin decrease (POD 7∼14)‡ 1.81 0.12 0.381
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*Bilirubin decrease rate = (initial bilirubin-preop. bilirubin)/preop. biliary drainage duration; †Postop. bilirubin decrease (POD 1∼7) = Serum bilirubin POD1∼Serum bilirubin POD7; ‡Postop. bilirubin decrease (POD 7∼14) = Serum bilirubin POD7∼Serum bilirubin POD14.
Fig. 1. Comparison of preoperative bilirubin decrease rate between uncomplicated and complicated groups. Slope of the lines implicate the bilirubin decrease rate. Serum bilirubin of uncomplicated patients tended to decrease faster, but there was no statistically significant difference between the two groups.
Fig. 2. Comparison of postoperative bilirubin decrease rate between uncomplicated and complicated groups. Serum bilirubin of uncomplicated patients decreased faster in the immediate postoperative days.
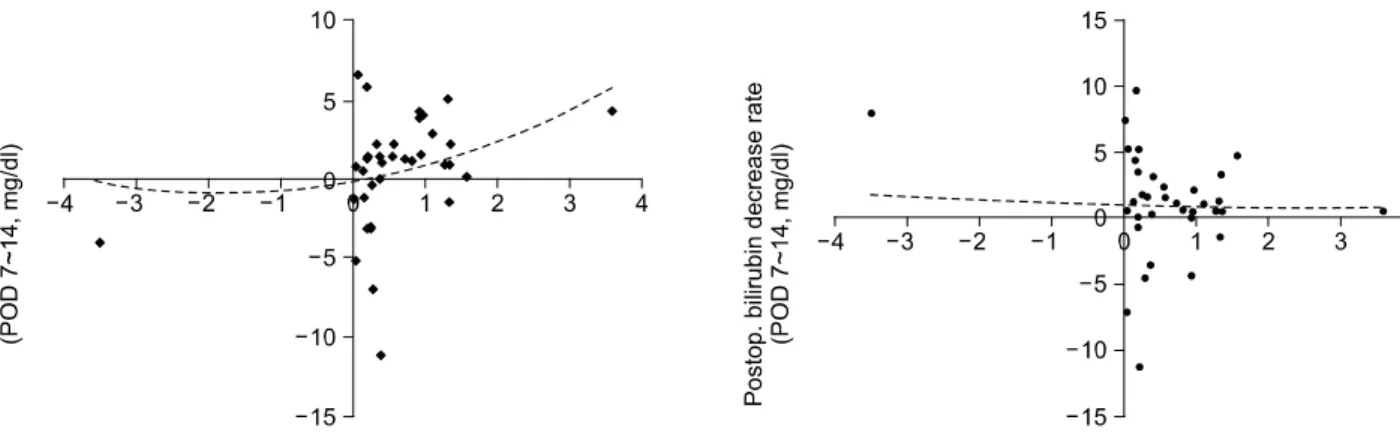
도와 수술 후 1일부터 7일까지 혈청 빌리루빈 감소 속도와 는 상관관계가 있었으나(r=0.371, 유의확률 0.05)(Fig. 3) 7 일부터 14일까지의 감소 속도와는 상관관계가 없었다(r=
-0.219)(Fig. 4).
고 찰
췌십이장절제술은 팽대부 주위암(periampullary cancer)에 대한 표준 수술이나 수술에 따른 유병율과 사망률은 비교 적 높은 편이다. 수술 후 사망률은 최근에는 0.7∼2%로 감 소하였으나6,7 수술 술기 및 수술 전후 환자관리의 발전에도 불구하고 수술 후 합병증 발생률은 30∼43%로 아직까지 높 은 편이며 수술 후 합병증 중에서 가장 흔하고 또한 관리가 어려운 것은 췌공장문합부 누출 혹은 누공으로서 약 10∼
21.8%까지 발생하는 것으로 보고되고 있다.4,6,7-10 췌십이장 절제술 후 합병증 발생과 연관된 인자에 관한 보고는 다양 한데 혈청 크레아티닌 수치를 포함한 수술 전 신기능, 수술 중 적혈구 수혈, 그리고 연관된 다른 장기의 절제 등이 보고 되고 있다.7,8,11
원위 담도암 환자의 주증상은 황달(85%) 및 체중감소 (43%)이고 또한 환자의 대부분이 고빌리루빈 혈증 소견을 보인다.1 고빌리루빈 혈증과 연관된 대수술의 합병증에 관 한 보고가 많이 발표되고 있는데 고빌리루빈 혈증이 급성 신부전 환자 혹은 범발성 복막염으로 수술을 받는 환자의 사망률을 높이는 요인이 된다고 알려지고 있다.12,13 또한 담 도 폐쇄에 의한 황달 환자에서 장기간의 담도 폐쇄에 의하 여 간 세포 손상을 입을 수 있고 이런 경우 담도의 감압 후 에도 혈청 빌리루빈 수치의 감소가 늦어질 것이 예상되고 간기능의 회복이 늦어지거나 회복자체가 안 될 가능성도
있다는 연구발표도 있다.14 이런 이유 때문에 팽대부 주위암 환자에서 췌십이지장 절제술 전 담도 감압을 하여 혈청 빌 리루빈 수치를 낮춘 경우 수술 후 합병증의 발생률에 영향 을 미칠 수 있는가에 대한 연구가 많이 진행되었는데 담도 감압 후 합병증이 감소하였다는 보고가 있었으나11 최근 많은 연구에서는 수술 전 담도 감압여부와 수술 후 합병증 발생 률에는 상관관계가 없다고 보고되고 있으며2,3,15 오히려 담 도감압 방법에 따라서는 감압 도관에 의한 감염성 합병증 의 위험성이 높아진다는 보고도 있었다.15 현재까지의 결과 수술 전 담도 감압술이 췌십이지장 절제술 후 합병증의 발 생률을 낮출 수 있는 방법인가에 대해서는 논란의 여지가 있다.11 그러나 일부 논문에서 범발성 복막염으로 수술 후 고빌리루빈 혈증이 발생하면 수술 후 사망률이 높지만 수 술 후 3∼5일 사이에 혈청 빌리루빈 수치가 감소하면 생존 률이 높다는 보고를 하고 있다.13
본 연구에서는 원위 담도암 환자들에서 수술 전 담도 감 압술을 시행한 경우 합병증의 발생에 영향을 미치는가에 대해 분석을 하였으나 담도 감압술 시행 자체로는 합병증 발생에 영향이 없다는 결과가 나왔으며 수술 후 합병증이 없었던 군에서 수술 전 담도 감압 시 혈청 빌리루빈 수치의 감소율이 높은 경향을 보였으나 통계적인 유의성은 없었다 (p=0.117). 다만, 수술 전 빌리루빈 감소율이 높은 환자들에 서 수술 후 초기(1∼7일) 빌리루빈 감소 속도가 빠르고 (r=0.371, p=0.05) 수술 후 합병증 발생군보다 정상 회복군에 서 초기 빌리루빈 감소가 빠른 소견을 보이므로(p=0.015) 이들 결과를 종합하면 수술 전 담도감압을 한 환자에서 빌 리루빈 수치가 빨리 감소되는 환자들은 수술 후 간 기능이 빠르게 회복된다고 해석할 수 있다. 간 기능의 회복속도가 췌십이지장절제술 후 합병증 발생률 및 사망률에 영향을 Fig. 3. Correlations between pre- and postoperative bilirubin
decrease rates (POD #1∼POD #7). The rate of decrease in the preoperative serum bilirubin levels were correlated with that of immediate postoperative days (Pearson correlation, r=0.371, significant at the level of p=0.05).
Fig. 4. Correlations between pre- and postoperative bilirubin decrease rates (POD #7∼POD #14). Preoperative bilirubin de- crease rate and postoperative bilirubin decrease rate from postoperative day 7 to postoperative day 14 showed no significant correlation (Pearson correlation r=-0.219, p>0.05).
미칠 수 있는가에 대하여는 더욱 많은 증례를 포함하는 연 구가 필요할 것으로 생각된다.
참 고 문 헌
1) Chung C, Bautista N, O'Connell TX. Prognosis and treatment of bile duct carcinoma. Am Surg 1998;64:921-925.
2) Martignoni ME, Wagner M, Krahenbuhl I, et al. Effect of preoperative biliary drainage on surgical outcome after pancreaticoduodnectomy. Am J Surg 2001;181:52-59.
3) Sewnath ME, Birjmohun RS, Rauws EA, et al. The effect of preoperative biliary drainage on postoperative complications after pancreaticoduodenectomy. J Am Coll Surg 2001;192:
726-734.
4) Hashimoto N, Yasuda C, Ohyanagi H. Pancreatic fistula after pancreatic head resection: incidence, significance and manage- ment. Hepatogastroenterol 2003;50:1658-1660.
5) Fischer A, Benz S, Baier P, Hopt UT. Endoscopic management of pancreatic fistula secondary to intraabdominal operation.
Surg Endosc 2004;18:706-708.
6) Hodul P, Creech S, Pickleman J, Aranha GV. The effect of preoperative biliary stenting on postoperative complications after pancreaticoduodenectomy. Am J Surg 2003;186:420-425.
7) Gouma DJ, Green van RCI, Gulik van TM, et al. Rates of complications and death after pancreaticoduodenectomy: Risk factors and the impact of hospital volume. Ann Surg 2000;232:
786-795.
8) Adam U, Makowiec F, Riediger H, Benz S, Liebe S, Hopt UT. Pancreatic leakage after pancreas resection. An analysis of 345 operated patients. Chirurg 2002;73:466-473.
9) Tocchi A, Lepre L, Mazzoni G, et al. Pancreatic anastomotic fistula after pancreaticodoudenectomy: incidence, significance and treatment. G Chir 2002;23:185-189.
10) Molino D, Perrotti P, Napoli V, et al. Surgical complications following pancreaticoduodenectomy : results of a single center experience. G Chir 2002;23:405-412.
11) Adam U, Makowiec F, Riediger H, Schareck WD, Benz SM, Hopt UT. Risk factors for complications after pancreatic head resection. Am J Surg 2004;187:201-208.
12) Cherotow GM, Lazarus JM, Paganini EP, Allgren RL, Lafa- yette RA, Sayegh MH. Predictors of mortality and the provision of dialysis in patients with acute tubular necrosis.
The Auriculin Anaritide Acute Renal Failure Study Group. J Am Soc Nephrol 1998;9:692-698.
13) Nishida T, Fujita N, Megawa T, Nakahara M, Nakao K.
Postoperative hyperbilirubinemia after surgery for gastrointers- tinal perforation. Surg Today 2002;32:679-684.
14) Chen CY, Shiesh SC, Lin XZ. Indicators of liver excretory function in patients undergoing biliary decompression for obstructive jaundice. Hepatogastroenterol 1998;45:786-790.
15) Goyal V, Mehta JM, Jenaw RK. Does preoperative biliary stenting affect the outcome of pancreaticoduodenectomy? In- dian J Gastroenterol 2003;22:164-165.