폐경 여성에서 호르몬 치료가 자궁 근종의 크기에 미치는 영향
성균관대학교 의과대학 삼성서울병원 산부인과, 충남대학교 통계학과1, 삼성서울병원 건강의학센터2
최석주․김주한1․권점미2․최두석․윤병구
The Effects of Estrogen-progestogen Therapy on Uterine Myomas in Postmenopausal Women
Suk Joo Choi, Joo Han Kim1, Jeom Mi Kwon2, Doo Seok Choi, Byung-Koo Yoon
Department of Obstetrics and Gynecology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Department of Statistics, Chungnam National University, Daejeon1,
Center for Health Promotion, Samsung Medical Center, Seoul, Korea2
Objective: To evaluate the effects of estrogen-progestogen therapy (EPT) on the volume of uterine myomas in postmenopausal women.
Methods: We performed a retrospective analysis of postmenopausal women with uterine myoma during the period between April, 1997 and September, 2004. Postmenopause was defined as amenorrhea for longer than a year or serum follicle stimulating hormone level higher than 40 U/L. Uterine myoma was detected by transvaginal ultrasonography before EPT. Current or recent users of EPT were excluded.
Control group was consisted of postmenopausal women with uterine myoma who had not received any EPT. Follow-up ultrasonography was performed at 6 and 12 months. Volume change was considered clinically significant if it was greater than 30% compared with the previous measurement.
Results: Thirty-one women were included in the study, with 26 in the EPT group and 5 in the control group.
Overall, uterine myoma volume (mean±SD, cm3) in the EPT group was 19.4±24.5 at baseline and those at six and 12 months were 23.6±34.9 and 28.4±55.3, respectively. Myoma volume did not change signifi- cantly with EPT, and these changes were not significantly different from the control group. Myoma volume changes were not significantly different between the subgroups according to the route of estrogen administration and the method of progestogen administration. Clinically significant volume increase during one year of EPT was noted in 30.8% (8/26), however, all except one showed only transient increase.
Conclusion: EPT does not have significant impact on the size of uterine myoma in postmenopausal women.
Key Words: Uterine myoma, Postmenopause, Estrogen-progestogen therapy
6)
책임저자:윤병구, 성균관대학교 의과대학 삼성서울병원 산부 인과
Tel: 02)3410-3519, Fax: 02)3410-0630 E-mail: [email protected]
* 본 연구는 인성의과학연구재단 연구비 (C-A5-811-1)의 일부보 조로 이루어졌음.
여성에서 자궁근종은 가장 흔한 골반종양으로 가 임기 여성에서의 자궁 근종의 유병률은 40~50%이 다1,2. 우리나라의 경우 일반 인구에서의 유병률은 현 재까지 보고된 바 없다. 입원 환자를 대상으로 한 연 구에서 자궁 근종의 빈도는 약 20% 내외로 보고되고 있으나3,4 일반 인구에서의 유병률은 이보다 높을 것
으로 추정된다.
호르몬 치료는 폐경 후 증후군과 비뇨생식기의 위 축에 따른 증상을 호전시켜 삶의 질을 향상시키고, 골다공증의 예방 및 치료에도 우수한 효과를 보인 다. 2002년 Women’s Health Initiative (WHI) 임상 시 험은 conjugated equine estrogen과 medroxyprogeste- rone acetate를 병합한 호르몬 치료가 심혈관 질환 및 유방암의 위험을 증가시킨다고 보고되었다5. 그 이 후 폐경 여성에서 호르몬 치료의 이득과 위험에 대 한 논란은 그치지 않고 있다. 그러나 여전히 많은 수 의 폐경 여성은 갱년기 증상의 호전과 골다공증 예 방을 위해 호르몬 치료를 받고 있다.
자궁 근종은 흔히 에스트로겐 의존적으로 성장하 는 것으로 알려져 있다6,7. 그러므로 자궁 근종을 가 지고 있는 폐경 여성에서 호르몬 치료는 근종 크기 의 증가 또는 근종 증상의 악화에 대한 우려, 그리고 암에 대한 공포 등으로 인하여 의사와 환자 모두에 게 불안 요소가 되고 있다. 그러나 폐경 여성에서 호 르몬 치료가 자궁 근종의 크기와 증상에 미치는 영 향에 대한 연구는 부족한 상태이고, 현재 뚜렷한 결 론은 내려지지 않고 있다8-16. 따라서 본 연구의 목적 은 폐경 여성에서 호르몬 치료가 자궁 근종의 크기 에 미치는 영향을 분석하는 것이다.
대상 및 방법
1997년 4월부터 2004년 9월까지 삼성서울병원 폐 경 클리닉을 방문한 폐경 여성 중 호르몬 치료 전 초음파상 자궁 근종이 발견된 여성을 대상으로 후향 적 고찰을 시행하였다. 폐경은 최종 생리일로부터 1 년 이상 경과하였거나, 혈중 난포자극호르몬 농도가 40 mIU/ mL 이상인 경우로 정의하였다. 초음파상 자 궁 근종의 최대 직경이 2 cm 이상이고 근종의 개수 가 3개 이하인 경우를 연구대상에 포함시켰으며, 근 종의 위치에 따른 제한은 없었다. 호르몬 치료의 금 기증이 있는 여성과 경구용 피임약이나 호르몬 치료 의 과거 혹은 현재 사용자는 제외하였다. 대조군으 로 자궁 근종이 발견된 폐경 여성 중 호르몬 치료를 받지 않은 환자를 추적 관찰하였다.
질식 초음파 검사 (5 MHz probe, Aloka SDD 1700,
Japan)를 이용하여 자궁 근종의 크기를 호르몬 치료 전과 치료 후 6개월과 12개월에 측정하였다. 자궁 근종의 부피 (cm3)는 삼차원의 세 직경을 이용한 0.521×D1×D2×D3 공식을 이용하여 계산하였으며, 임상적으로 유의한 부피 변화는 이전 측정치에 비하 여 30% 이상인 경우로 정하였다.
기초 자료에 대한 통계적 분석을 위해 Mann- whitney U test를 사용하였다. 대상 환자 수가 적고 자료의 분포가 크며 정규분포를 이루지 않아 Wilco- xon two-sample test를 이용하여 자궁 근종의 부피 변 화를 비교하였다. 임상적으로 유의한 자궁 부피의 변화 양상의 비교를 위하여 chi-square test를 적용하 였다. 통계학적 유의성은 P<0.05로 정의하였고, 연 구 결과는 평균±표준편차로 표시하였다.
결 과
연구대상으로 총 31명의 환자를 분석하였으며, 이 중 호르몬 치료군이 26명, 대조군이 5명이었다. 호르 몬 치료군 중 에스트로겐 투여 경로에 따라 경구용 에스트로겐 사용군이 18명, 경피용 에스트로겐 사용 군이 8명이었다. 경구용 에스트로겐 제제는 conju- gated equine estrogen (PremarinⓇ, Wyeth; 0.625 mg/
day)과 estropipate (OgenⓇ, Pharmacia; 0.625 mg/day)을 각각 12명과 6명에서 사용되었다. 경피용 에스트로 겐 제제는 17β-estradiol patch (EstranⓇ, 삼양사 50 μg/day)와 17β-estradiol gel (EstrevaⓇ, 삼일제약 1.5 mg/day)을 각각 4명에서 사용되었다. 프로게스토겐 의 투여법에 따라 매일 투여하는 지속적 요법 (continuous combined method)군과 매월 12일간 추가 되는 순차적 요법 (sequential cyclic method)군이 각각 13명이었다. 프로게스토겐 제제는 medroxyprogeste- rone acetate (CycrinⓇ, 한국 Wyeth 5 mg/day)가 1예에 서 사용되었으며, 나머지 17명은 micronized proges- terone (UtrogestanⓇ, 한화제약 200 mg/day)이 투여되 었다.
연구대상 전체의 연령은 55.2±5.5세, 초경은 15.5
±1.6세, 폐경은 50.8±3.4세, 폐경 후 기간은 4.6±5.0 년이었다. 기초특성 상 호르몬 치료군과 대조군 간 에 차이가 없었고, 호르몬 치료군에서 경구용 에스
Table 1. Baseline characteristics of the study patients
Control (n=5)
Estrogen-progestogen therapy (n=26)
P value*
Oral estrogen (n=18)
Parenteral estrogen (n=8)
Total (n=26) Age (year)
Weight (kg) Height (cm)
Age of menarche (year) Gravida
Age of menopause (year) Years since menopause
59.4±7.5 57.3±7.2 156.2±4.5 15.6±1.1 3.6±2.1 51.4±4.5 8.0±9.8
55.1±4.2 60.6±6.8 156.2±5.3 15.3±1.8 4.6±1.9 51.0±3.2 4.3±3.4
52.9±6.0 60.5±10.7
158.3±3.8 15.9±1.3 6.0±3.6 50.0±3.4 3.1±3.4
54.4±4.8 60.6±8.0 156.8±4.9 15.5±1.6 5.0±2.6 50.7±3.2 3.9±3.4
NS NS NS NS NS NS NS Data are expressed as mean±standard deviation.
NS: not significant (control vs. hormone replacement therapy group and oral vs. parenteral estrogen group).
*Mann-Whitney U test.
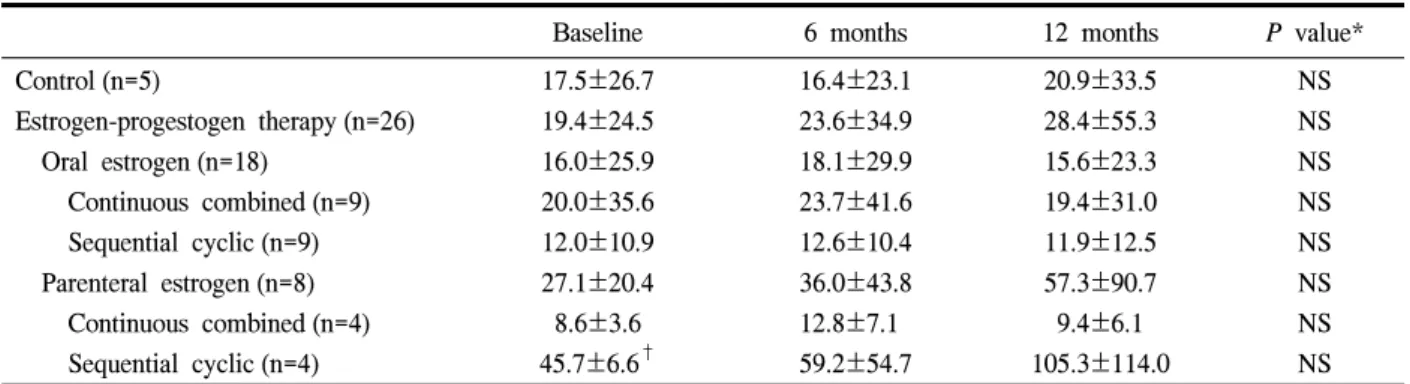
Table 2. Changes in the volume of uterine myoma with estrogen-progestogen therapy
Baseline 6 months 12 months P value*
Control (n=5)
Estrogen-progestogen therapy (n=26) Oral estrogen (n=18)
Continuous combined (n=9) Sequential cyclic (n=9) Parenteral estrogen (n=8) Continuous combined (n=4) Sequential cyclic (n=4)
17.5±26.7 19.4±24.5 16.0±25.9 20.0±35.6 12.0±10.9 27.1±20.4 8.6±3.6 45.7±6.6†
16.4±23.1 23.6±34.9 18.1±29.9 23.7±41.6 12.6±10.4 36.0±43.8 12.8±7.1 59.2±54.7
20.9±33.5 28.4±55.3 15.6±23.3 19.4±31.0 11.9±12.5 57.3±90.7 9.4±6.1 105.3±114.0
NS NS NS NS NS NS NS NS Data are expressed as mean±standard deviation, cm3.
NS: not significant between each time-interval.
*Wilcoxon two-sample test, †P=0.029, Wilcoxon two-sample test, sequential vs. continuous combined in parenteral estrogen group.
Fig. 1. Distribution of myoma volume changes with estrogen- progestogen therapy.
트로겐과 경피용 에스트로겐 사용군 간에도 차이가 없었다 (Table 1).
자궁 근종 부피의 기저치는 호르몬 치료군과 대조 군 간 차이가 없었고, 각 군에서 추적 검사 상 유의 한 변화는 없었다. 치료 전과 6개월 사이, 6개월과 12개월 사이 및 치료 전과 12개월 사이의 자궁 근종 의 부피 변화도 두 군간 유의한 차이를 보이지 않았 다. 그리고 에스트로겐 투여 경로와 프로게스토겐 투여법에 따른 자궁 근종의 부피 변화 상 차이도 없 었다 (Table 2).
호르몬 치료군에서 6개월, 6개월과 12개월, 그리 고 12개월 사이 부피의 유의한 변화 상 불변 또는
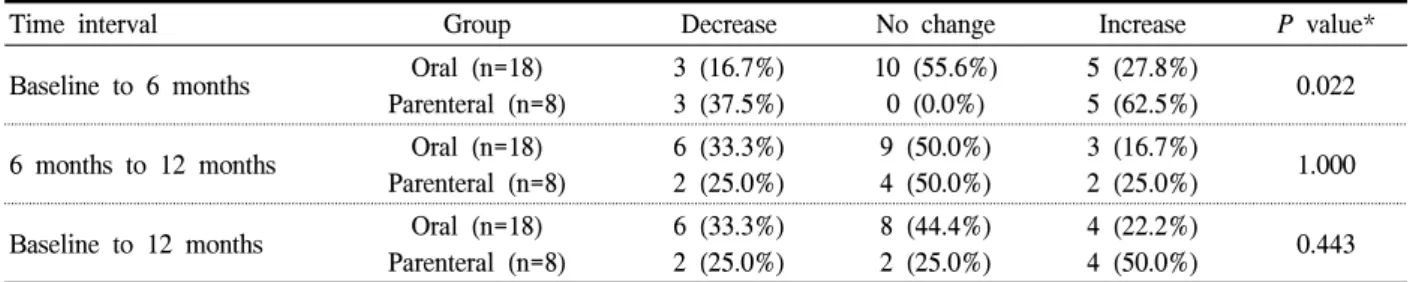
Table 3. Distribution of myoma volume change according to the route of estrogen administration
Time interval Group Decrease No change Increase P value*
Baseline to 6 months Oral (n=18) Parenteral (n=8)
3 (16.7%) 3 (37.5%)
10 (55.6%) 0 (0.0%)
5 (27.8%)
5 (62.5%) 0.022
6 months to 12 months Oral (n=18) Parenteral (n=8)
6 (33.3%) 2 (25.0%)
9 (50.0%) 4 (50.0%)
3 (16.7%)
2 (25.0%) 1.000
Baseline to 12 months Oral (n=18) Parenteral (n=8)
6 (33.3%) 2 (25.0%)
8 (44.4%) 2 (25.0%)
4 (22.2%)
4 (50.0%) 0.443
*χ2 test
Table 4. Pattern of myoma volume changes with estrogen-progestogen therapy (EPT) A. Changes with one-year EPT according to those from 6 to 12 months
One-year change Change from 6 to 12 months
Total Decrease No change Increase
Decrease No change Increase
5 2 1
3 5 5
0 3 2
8 (30.8%) 10 (38.5%) 8 (30.8%)
Total 8 (30.8%) 13 (50.0%) 5 (19.2%) 26 (100%)
P=0.2077, χ2 test
B. Changes during initial 6 months and subsequent 6 months in the total EPT group
Change from baseline to 6 months Change from 6 to 12 months
Total Decrease No change Increase
Decrease No change Increase
1 3 4
3 5 5
2 2 1
6 (23.1%) 10 (38.5%) 10 (38.5%)
Total 8 (30.8%) 13 (50.0%) 5 (19.2%) 26 (100%)
P=0.8687, χ2 test
C. Changes during initial 6 months and subsequent 6 months in the oral estrogen group
Change from baseline to 6 months Change from 6 to 12 months
Total Decrease No change Increase
Decrease No change Increase
1 3 2
1 5 3
1 2 0
3 (16.7%) 10 (55.6%) 5 (27.8%)
Total 6 (33.3%) 9 (50.0%) 3 (16.7%) 18 (100%)
P=0.8982, χ2 test
D. Changes during initial 6 months and subsequent 6 months in the parenteral estrogen group
Change from baseline to 6 months Change from 6 to 12 months
Total Decrease No change Increase
Decrease No change Increase
0 0 2
2 0 2
1 0 1
3 (37.5%) 0 (0.0%) 5 (62.5%)
Total 2 (25.0%) 4 (50.0%) 2 (25.0%) 8 (100%)
P=0.7143, χ2 test
감소 분포양상은 유의한 차이가 없었다 (Fig. 1). 그 러나 경구용 에스트로겐 사용군과 경피용 에스트로 겐 사용군으로 나누어 분석한 결과, 기저치와 6개월 사이의 자궁 근종 부피의 변화 양상은 두 군간 유의 한 차이를 나타내었다 (Table 3).
호르몬 치료군에서 치료 전과 12개월 사이에 자궁 근종의 부피가 유의하게 증가한 경우는 8예 (30.8%) 이었다 (Table 4A). 8예 중 6예에서 자궁 근종의 부피 가 첫 6개월에는 유의하게 증가하였으나 후반 6개월 사이에는 변화가 없거나 감소하였다. 후반 6개월 사 이에 증가한 2예 중 1예는 치료 18개월에 추적 조사 한 결과 더 이상의 부피 증가는 없었다 (Table 4B, 4C, 4D). 나머지 1예는 경피용 에스트로겐이 투여된 환자로 자궁 근종의 부피가 계속 증가하였고, 환자 가 원하여 전자궁절제술을 시행하여 병리학적 소견 상 양성 자궁 근종을 확인하였다.
고 찰
자궁 근종의 발생 원인은 명확히 알려져 있지 않 다. 그러나 초경 이전의 여성에서는 자궁 근종의 발 생이 보고된 바가 없고, 폐경 후 자궁 근종의 크기가 감소하는 것으로 보아 혈중 난소 호르몬 농도의 생 리적 변화와 밀접한 관련이 있을 것으로 생각된다6. 자궁 근종이 에스트로겐 의존성 발생 및 성장을 한 다는 것은 잘 알려져 있다17. 최근에는 자궁 근종의 증식에 프로게스테론의 역할이 대두되고 있다18-20. 자궁 근종의 발생과 성장에서 에스트로겐과 프로게 스테론의 역할은 근종 조직에서 두 호르몬 수용체의 증가와 밀접하게 관련되어 있다19,21,22. 폐경 이후 자 궁 근종의 크기는 감소하고 이는 에스트로겐과 프로 게스테론의 혈중 농도의 감소와 관련된 것으로 생각 된다. 그러나 폐경 여성에서 외인성 호르몬 투여가 자궁 근종의 크기에 어떠한 영향을 주는지는 명확한 결론이 없다. 본 연구 결과, 폐경 여성에서 호르몬 치료에 따른 자궁 근종 부피는 유의한 변화가 없었 다. 또한 에스트로겐 투여 경로와 프로게스토겐 투 여법에 따른 차이도 없었다.
호르몬 치료가 폐경 후 자궁 근종의 변화에 미치 는 영향은 다양하게 보고되고 있다8-16. 이는 각 연구
에서 사용된 에스트로겐의 다양한 투여경로와 용량, 그리고 병합한 프로게스토겐의 종류와 용량에 따라 자궁 근종의 크기에 서로 다른 영향을 미치기 때문 인 것으로 생각된다. 대부분의 연구에서 경구용 에 스트로겐은 자궁 근종의 크기를 증가시키지 않으
나8,9,15,16 경피용 에스트로겐의 영향은 다양하다8-11.
Colacurci 등10과 Palomba 등11은 경피용 17β-estradiol patch의 사용이 자궁 근종 부피를 증가시키지 않는 다고 보고하였다. 한편, Polatti 등8과 Sener 등9의 연 구에서는 경구용 에스트로겐 사용군에 비해 경피용 에스트로겐 사용군에서 자궁 근종의 부피가 증가하 였다. 그러나 Polatti 등8과 Sener 등9의 연구에서 경 구용 에스트로겐 사용군과 경피용 에스트로겐 사용 군의 프로게스토겐 용량 또는 용법이 서로 다르므로 자궁 근종의 부피 증가가 에스트로겐의 투여 경로에 따른 것인지 프로게스토겐의 투여 방법 차이에 의한 것인지 알 수 없다. Sener 등9은 두 군의 혈중 에스트 로겐 농도가 차이가 없음을 보여 자궁 근종의 부피 증가가 에스트로겐 투여 경로의 차이보다는 프로게 스토겐 용량 차이 (medroxyprogesterone acetate 5 mg vs. 2.5 mg)에 의한 결과일 것이라고 주장하였다.
Palomba 등23은 30명의 폐경 여성을 대상으로 시행 한 무작위 연구 결과 micronized estradiol 2 mg과 함 께 medroxyprogesterone acetate를 각각 2.5 mg과 5 mg 투여하였을 때 5 mg 투여군에서 자궁 근종 크기가 유의하게 증가한다고 보고하였다. 본 연구에서 경구 용 에스트로겐 사용군과 경피용 에스트로겐 사용군 간에 프로게스토겐의 용법과 용량은 유사하였으나 치료 전과 6개월 사이의 자궁 근종 부피의 변화 양 상은 유의한 차이를 보였다.
본 연구에서 주목할 점은 자궁 근종 부피의 증가, 불변 그리고 감소의 분포가 다양하고 일정한 양상을 보이지 않는다는 것이고, 이는 폐경 여성에서 호르 몬 치료의 직접 영향이 그다지 크지 않을 수도 있음 을 시사한다. 호르몬 치료 중 자궁 근종의 크기 증가 는 호르몬 치료를 중단케 하는 원인이 될 수 있다.
본 연구에서는 30% 이상의 변화를 의미 있다고 정 의하였다. 치료 전과 12개월 사이를 비교한 결과 30.8%에서 부피 증가가 관찰되었다. 부피증가는 첫 6개월에 38.5%이었으나 후반 6개월에는 19.2%로 감
소하는 경향을 보였다. 호르몬 치료 중 자궁 근종의 부피가 증가하는 경우 주의 깊은 추적 관찰이 중요하 다. Colacurci 등은10 3개월 간격의 추적 초음파 검사 가 자궁 근종의 부피 증가를 평가하는데 도움이 된 다고 하였고, Doppler 파형검사 상 호르몬 치료 후 자궁 동맥의 저항이 감소한 경우 자궁 근종의 크기 증가와 관계가 있다고 하였다.
초음파 검사를 포함하는 영상의학 검사만으로는 자궁 근종과 자궁 육종을 감별하기 매우 어렵기 때 문에 호르몬 치료 중 자궁 근종이 계속해서 자라는 경우 의사와 환자 모두에게 불안감을 흔히 유발시킨 다. 자궁 육종은 자궁의 악성 종양 중 1% 미만으로 발생하는 매우 드문 악성 종양으로서 예후가 매우 불량하다24. 수술 전 자궁 근종으로 진단된 여성에서 수술 후 병리 검사 상 자궁 육종이 발견된 빈도는 0.5% 미만으로 매우 낮고25, 자궁 육종이 자궁 근종 세포로부터 악성 변화한 것인지 또는 자궁 근종과 무관하게 자궁 근육 세포에서 자궁 육종으로 발달하 는 것인지는 명확히 밝혀진 바 없다. 또한 외인성 에 스트로겐이 자궁 육종의 발생 빈도를 높인다는 증거 는 없다26. 단, 자궁 근종의 크기가 증가하는 경우 추 적 관찰이 필수적이며, 계속 증가하는 경우 약제를 변경하거나 일시적으로 중단한 후 결과를 관찰할 수 있다.
본 연구는 의무기록에 의존한 후향적 연구이라는 점과 연구 대상의 숫자가 적다는 것에서 한계점을 지니고 있다. 또한 초음파 검사를 시행한 검사자가 서로 다르기 때문에 검사자간 오차를 극복하지 못한 것도 본 연구의 단점으로 지적될 수 있다. 그리고 단 일화된 호르몬 치료 방법을 사용하질 않았으므로 다 양한 호르몬 제제의 서로 다른 영향을 배제할 수 없 다. 따라서 향후 보다 많은 수의 환자를 대상으로 다 양한 전향적 무작위 연구가 필요하다.
결론적으로 본 연구에서 폐경 여성에서 호르몬 치 료는 자궁 근종의 크기 변화에 유의한 영향을 주지 않으며, 에스트로겐 투여 경로와 프로게스토겐 투여 방법에 따른 차이도 없었다. 또한, 호르몬 치료에 따 른 자궁 근종 부피의 증가, 불변 그리고 감소의 분포 는 다양한 양상을 보이므로 예측하기 어려우나 자궁 근종의 부피가 지속적으로 증가하는 경우에는 주의
깊은 추적 관찰이 필요할 것으로 생각된다.
요 약
목적: 본 연구의 목적은 호르몬 치료가 폐경 여성 의 자궁 근종의 크기에 대한 영향을 평가하는 것이 다.
방법: 1997년 4월부터 2004년 9월까지 폐경 클리 닉을 방문한 폐경 여성 중 호르몬 치료 전 초음파 검사 상 자궁 근종이 발견된 여성을 대상으로 후향 적 고찰을 시행하였다. 폐경은 최종 생리로부터 1년 이 경과하거나 혈중 FSH 농도가 40 U/L 이상인 경우 로 정의하였다. 호르몬 치료 중 자궁 근종의 부피를 각각 6개월, 12개월에 측정하였고, 이전 측정치보다 30% 이상 변화한 경우 임상적으로 유의한 변화로 정하였다.
결과: 총 32명의 환자를 대상으로 분석을 시행하 였으며, 이 중 호르몬 치료군에 26명, 대조군에 5명 이 각각 포함되었다. 호르몬 치료군에서 자궁 근종의 부피 (평균±표준편차, cm3)는 치료 전 (19.42±24.46) 과 6개월 후 (23.62±34.88) 및 12개월 후 (28.43±5.26) 사이에 유의한 차이가 없었고, 대조군과의 비교에서 도 유의한 차이를 보이지 않았다. 에스트로겐 투여 경로와 프로게스토겐 투여 방법에 따른 자궁 근종의 부피도 의미 있는 변화를 보이지 않았다. 치료 전과 12개월 사이에 임상적으로 유의한 부피 증가는 30.8% (8/26)에서 관찰되었다. 증가, 불변, 감소 등 부 피 변화 지표의 분포양상은 전체, 군내 및 군간 분석 에서 차이가 없었으나 경구용 또는 경피용 에스트로 겐 사용군 간에 치료 전과 6개월 사이에 유의한 차 이를 보였다.
결론: 폐경 여성에서 호르몬 치료는 자궁 근종의 부피에 유의한 영향을 주지 않는다.
중심단어: 자궁 근종, 폐경, 호르몬 치료
참 고 문 헌
1. Marshall LM, Spiegelman D, Barbieri RL, Gold- man MB, Manson JE, Colditz GA, et al. Variation in the incidence of uterine leiomyoma among
premenopausal women by age and race. Obstet Gynecol 1997;90:967-73.
2. Schwartz SM. Epidemiology of uterine leiomyo- mata. Clin Obstet Gynecol 2001;44:316-26.
3. 서호성, 남철, 김창수, 장병곤, 양희동, 박세준.
자궁근종에 대한 임상통계학적 연구. 대한산부 회지 1996;39:1047-57.
4. 이중희. 자궁근종의 임상통계적 관찰. 대한산부 회지 1968;11:65-73.
5. Rossouw JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML, et al. Risks and benefits of estrogen plus progestin in healthy post- menopausal women: principal results From the Women's Health Initiative randomized controlled trial. JAMA 2002;288:321-33.
6. Stewart EA. Uterine fibroids. Lancet 2001;357:
293-8.
7. Ang WC, Farrell E, Vollenhoven B. Effect of hor- mone replacement therapies and selective estrogen receptor modulators in postmenopausal women with uterine leiomyomas: a literature review. Climacteric 2001;4:284-92.
8. Polatti F, Viazzo F, Colleoni R, Nappi RE. Uterine myoma in postmenopause: a comparison between two therapeutic schedules of HRT. Maturitas 2000;
37:27-32.
9. Sener AB, Seckin NC, Ozmen S, Gokmen O, Dogu N, Ekici E. The effects of hormone replacement therapy on uterine fibroids in postmenopausal women. Fertil Steril 1996;65:354-7.
10. Colacurci N, De Franciscis P, Cobellis L, Nazzaro G, De Placido G. Effects of hormone replacement therapy on postmenopausal uterine myoma. Matu- ritas 2000;35:167-73.
11. Palomba S, Sena T, Noia R, Di Carlo C, Zullo F, Mastrantonio P. Transdermal hormone replacement therapy in postmenopausal women with uterine leiomyomas. Obstet Gynecol 2001;98:1053-8.
12. Fedele L, Bianchi S, Raffaelli R, Zanconato G. A randomized study of the effects of tibolone and
transdermal estrogen replacement therapy in post- menopausal women with uterine myomas. Eur J Obstet Gynecol Reprod Biol 2000;88:91-4.
13. Simsek T, Karakus C, Trak B. Impact of different hormone replacement therapy regimens on the size of myoma uteri in postmenopausal period: tibolone versus transdermal hormonal replacement system.
Maturitas 2002;42:243-6.
14. Yang CH, Lee JN, Hsu SC, Kuo CH, Tsai EM.
Effect of hormone replacement therapy on uterine fibroids in postmenopausal women--a 3-year study.
Maturitas 2002;43:35-9.
15. De Aloysio D, Altieri P, Penacchioni P, Salgarello M, Ventura V. Bleeding patterns in recent post- menopausal outpatients with uterine myomas: com- parison between two regimens of HRT. Maturitas 1998;29:261-4.
16. Schwartz LB, Iazer S, Mark M, Natchticall LE, Horan C, Goldstein SR. Does the use of postmeno- pausal hormone replacement therapy influence the size of uterine leiomyomata? A preliminary report.
Menopause 1996;3:38-43.
17. Maruo T, Ohara N, Wang J, Matsuo H. Sex ste- roidal regulation of uterine leiomyoma growth and apoptosis. Hum Reprod Update 2004;10:207-20.
18. Ichimura T, Kawamura N, Ito F, Shibata S, Mina- kuchi K, Tsujimura A, et al. Correlation between the growth of uterine leiomyomata and estrogen and progesterone receptor content in needle biopsy specimens. Fertil Steril 1998;70:967-71.
19. Rein MS. Advances in uterine leiomyoma research:
the progesterone hypothesis. Environ Health Pers- pect 2000;108(Suppl 5):791-3.
20. Schweppe KW. Progestins and uterine leiomyoma.
Gynecol Endocrinol 1999;13(Suppl 4):21-4.
21. Tamaya T, Fujimoto J, Okada H. Comparison of cellular levels of steroid receptors in uterine leio- myoma and myometrium. Acta Obstet Gynecol Scand 1985;64:307-9.
22. Chrapusta S, Sieinski W, Konopka B, Szamborski
J, Paszko Z. Estrogen and progestin receptor levels in uterine leiomyomata: relation to the tumour histology and the phase of menstrual cycle. Eur J Gynaecol Oncol 1990;11:381-7.
23. Palomba S, Sena T, Morelli M, Noia R, Zullo F, Mastrantonio P. Effect of different doses of pro- gestin on uterine leiomyomas in postmenopausal women. Eur J Obstet Gynecol Reprod Biol 2002;
102:199-201.
24. Giuntoli RL 2nd, Metzinger DS, DiMarco CS, Cha SS, Sloan JA, Keeney GL, et al. Retrospective review of 208 patients with leiomyosarcoma of the
uterus: prognostic indicators, surgical management, and adjuvant therapy. Gynecol Oncol 2003;89:460- 9.
25. Leibsohn S, d'Ablaing G, Mishell DR Jr, Schlaerth JB. Leiomyosarcoma in a series of hysterectomies performed for presumed uterine leiomyomas. Am J Obstet Gynecol 1990;162:968- 74; discussion 74-6.
26. Schwartz SM, Weiss NS, Daling JR, Gammon MD, Liff JM, Watt J, et al. Exogenous sex hormone use, correlates of endogenous hormone levels, and the incidence of histologic types of sarcoma of the uterus. Cancer 1996;77:717-24.