Introduction
Tarsal tunnel syndrome (TTS) is an entrapment neuropathy of the posterior tibial nerve or of its branches (medial plantar, lateral plantar, or calcaneal
발목터널증후군의 영상 및 신경전도검사 특징과 수술적 치료 효과 분석
양지원
1
, 박현미1
, 박홍기2
, 이영배1
가천대학교 길병원 1신경과, 2정형외과
Tarsal Tunnel Syndrome: Analysis for Characteristics of MRI and Nerve Conduction Study, and the Outcome of Decompression Surgery
Jiwon Yang
1, Hyeon-Mi Park
1, Hong-Ki Park
2, Yeong-Bae Lee
1Departments of
1Neurology and
2Orthopedic Surgery, Gachon University Gil Medical Center, Incheon, Korea
Received September 15, 2015
Revised (1st) October 29, 2015, (2nd) November 4, 2015 Accepted November 4, 2015
Corresponding Author: Yeong-Bae Lee
Department of Neurology, Gachon University Gil Medical Center, 21 Namdong-daero 774beon-gil, Namdong-gu, Incheon 21565, Korea Tel: 82-32-460-3346, Fax: 82-32-460-3344, E-mail: [email protected]
Objective: In this retrospective study, the authors aimed to reveal radiological, electrophysiological characteristics of
tarsal tunnel syndrome (TTS), and their usefulness for diagnosis and measuring the treatment outcome. In addition, we assess postoperative outcomes by clinical and electrophysiological tools.Method: Thirty-three patients underwent unilateral tarsal tunnel decompression. Ankle MRI and nerve conduction study
was performed in all patients. Preoperative symptoms, radiological and electrophysiological results were reviewed and follow-up statuses were evaluated.Results: Twenty-eight of 33 (84.8%) patients showed symptomatic recovery and 23 (69.7%) showed improvement
objectively in the nerve conduction study. Preoperative MRI revealed a specific anatomical lesion in 18 patients.Improvements in nerve conduction study parameters were observed mainly in conduction velocity of lateral plantar nerves. There was no significant clinical factor to predict postoperative outcome.
Conclusion: In the present study, postoperative outcomes from the clinical and electrophysiological perspectives
were satisfactory. Nerve conduction study was good to evaluate the disease status and measure the surgical outcome objectively. MRI provided supportive information for diagnosing TTS. Tarsal tunnel decompression is warranted in those patients who remain symptomatic despite prolonged conservative treatment.Key Words: magnetic resonance imaging, nerve conduction study, tarsal tunnel syndrome, treatment outcome, surgical
decompressionCopyright © by Korean Association of EMG Electrodiagnostic Medicine
This is an Open Ac cess article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
ORIGI NAL ART ICLE
ISSN 1229-6066 http://dx.doi.org/10.18214/jkaem.2015.17.2.69 J Korean Assoc EMG Electrodiagn Med 17(2):69-75, 2015
J Korean Assoc
Electrodiagn Med EMG
nerve) under the flexor retinaculum at the medial side of the ankle.
1,2Those with TTS usually complain of a dull aching pain on the plantar aspect of the foot. The condition is distressing, but its accurate diagnosis is difficult because its symptoms are similar to those associated with other lower limb conditions, such as, radiculopathy, polyneuropathy, or local orthopedic problem. Electrophysiological and radiological investigations are currently used to diagnose TTS, determine its etiology, and predict treatment outcomes.
2,3However, some controversy remains regarding false negative electrophysiological studies and undefined etiologies based on radiological studies, and these make it difficult to institute surgical decompression at the proper time. Furthermore, the outcome of decompression varies widely according to published reports.
This retrospective study was undertaken; 1) to reveal radiological, electrophysiological characteristics of tarsal tunnel syndrome (TTS), and 2) to present the results of our TTS patients with respect to electro- physiological and symptomatic changes after decom- pression.
Materials and Methods
1) Subjects
Thirty-three patients (16 men and 17 women, mean age 49 years; range 20~72) that underwent tarsal tunnel release between January 2011 and December 2012 were reviewed in their medical records. This study was approved by our institutional review board.
Diagnosis was based on the clinical ground. All subjects complained of a disabling burning or tingling sensation or dysesthesia on the sole of foot. They were decided to undergo surgery when they did not feel better at all despite of taking medicine and life style change (rest, using soft footwear, etc) for more than 1 month. To exclude TTS-mimicking disease, patients underwent nerve conduction study (NCS) and electromyography (EMG) in bilateral lower limbs before
and after operation. None of 33 had radiculopathy, plexopathy or had systemic disease which would be capable of causing polyneuropathy. All subjects underwent ankle MRI at the symptomatic foot.
2) Nerve conduction study
Routine NCS was performed on the peroneal nerve (motor), posterior tibial nerve (motor), sural nerve (sensory), medial plantar nerve (MPN, [motor and sensory]), and lateral plantar nerve (LPN, [motor and sensory]). Distal motor latency (DML), motor and sensory nerve conduction velocity (NCV) and compound muscle action potential (CMAP) was measured.
4Electromyography was performed in muscles subserved by the tibial and peroneal nerves, and the dorsal rami of the spinal nerve distribution. All tests were performed using a Nicolet Viking IV EMG machine (Viasys Health Care, Madison, Wisconsin) by a single electromyographer. The foot skin temperature was measured at the start of the assessment, and kept at 32~34
oC.
We considered the values abnormal as below: 1) normal DML and NCV of posterior tibial nerve + delayed distal latency or reduced NCV of both plantar (MPN and LPN) nerves, 2) absence of significant plantar nerve action potential despite of repetitive stimulation.
And it was considered abnormal if it was 8 m/s slower than the asymptomatic MPN and/or the distal NCV of the sural nerve of the same side or a CMAP amplitude decrement of more than 30% across the tarsal tunnel.
5,6Furthermore, we sorted the objective severity of TTS
by electrophysiological parameters. Feet with abnormal
plantar NCS results were classified as: 0, normal
CV and DML; 1, normal absolute CV with abnormal
comparative tests;
5,62, slowing of plantar (sensory
or motor nerve) CV with normal DML; 3, slowing of
CV and prolonged DML; 4, absence of plantar SAP
and abnormal DML; 5, absence of sensory and motor
responses.
73) Clinical outcome measurement
Clinical outcome was measured by physician- patient interview at the time of the operating surgeon’s preoperative and postoperative follow-up visits. The postoperative status was obtained by inquring into the change of numeric rating scale for pain, disappearance of spontaneous pain, recovery from pain aggravation with walking. Clinical improvement was considered when a patient got more than 60% of pain relief and well-being sense in daily life after operation.
4) Statistics
Statistical analysis was conducted using Wilcoxon’s signed rank test, Mann-Whitney U test, or Fisher’s exact test as appropriate. The basic package of SPSS (version 18, Chicago, IL) was used for analysis. p-values of < 0.05 were considered significant.
Results
1) Demographic data
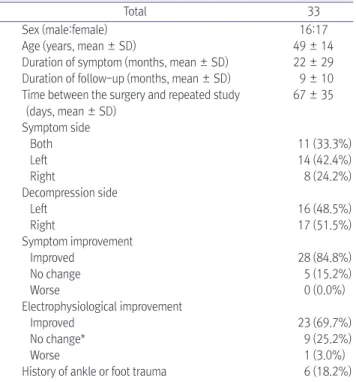
Thirty-three patients (16 men and 17 women) under- went surgical intervention when there is no clinical improvement after conservative treatment for at least one month. Mean patient age was 49 ± 14 years and mean symptom duration was 22 ± 29 months. Mean follow-up duration after operation was 9 ± 10 months.
Average time to repeat nerve conduction study after decompression was 67 ± 35 days. Bilateral symp- toms were present in 11 of 33 (33.3%) patients. In patients with unilateral symptom, the left foot was affected in 14 (42.4%) and the right foot in 8 (24.2%).
Operation was performed on the worse symptomatic foot when bilateral symptoms appeared, and thus, it was conducted on the left foot in 16 (48.5%) and on the right foot in 17 (51.5%). Clinical improvement rated by the extent of pain relief and returns to usual life, was observed in 28 (84.8%) patients, but little or no improvement was evident in the other 5 (15.2%) (Table 1). Operational complication was seen in 4 patients, usually with painful swelling at the ankle and
resolved in a week. There were no wound infections, deep venous thrombosis or overnight anesthetic administrations.
2) Electrophysiological results
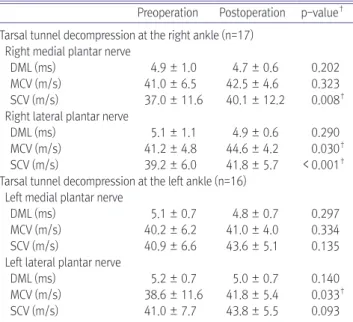
Twenty-five patients had NCS results consistent with tarsal tunnel syndrome and eight had normal NCS results. Of the 8 patients with normal NCS, five had bilateral symptoms. Of the 25 patients with an abnormal NCS, 9 had involvements of both motor and sensory plantar nerves, 12 had sensory nerve involvement only, and 4 had motor nerve involvement only. Most patients (n = 22, 66.7%) had grade 2 of electrophysiological severity. After decompressive operations, all parameters of NCS were improved than before the surgery. With the right tarsal tunnel decompression, medial plantar sensory CV was improved from 37.0 ± 11.6 m/s to 40.1 ± 12.2 (p = 0.008), lateral plantar motor and sensory CV was also significantly improved (motor CV: 41.2 ± 4.8 m/s to 44.6 ± 4.2 m/s, p = 0.030; sensory CV: 39.2 ± 6.0 m/s
Table 1. Demographic Characteristics
Total 33
Sex (male:female) 16:17
Age (years, mean ± SD) 49 ± 14
Duration of symptom (months, mean ± SD) 22 ± 29 Duration of follow-up (months, mean ± SD) 9 ± 10 Time between the surgery and repeated study
(days, mean ± SD)
67 ± 35
Symptom side
Both 11 (33.3%)
Left 14 (42.4%)
Right 8 (24.2%)
Decompression side
Left 16 (48.5%)
Right 17 (51.5%)
Symptom improvement
Improved 28 (84.8%)
No change 5 (15.2%)
Worse 0 (0.0%)
Electrophysiological improvement
Improved 23 (69.7%)
No change* 9 (25.2%)
Worse 1 (3.0%)
History of ankle or foot trauma 6 (18.2%) SD: standard deviation
*including numbers of normal nerve conduction study before operation (n = 8)
to 41.8 ± 5.7 m/s, p < 0.001). With the left tarsal tunnel decompression, lateral plantar motor CV was improved from 38.6 ± 11.6 m/s to 41.8 ± 5.4 m/s (p = 0.033).
In terms of severity, patients of 13 in 22 with grade 2 recovered as normal NCS (Table 2 and Fig. 1).
3) Relations between clinical and electrophy- siological results
Of 25 patients with abnormal NCS before operation, 23 showed improvements in both clinical and electrophysiological results. On the other hand, 1 patient showed symptom recovery without NCS improvement, and the other showed unimproved symptom and NCS. Of 8 patients with normal NCS before and after operation, 4 showed symptomatic improvement and the others did not. No significance could be attached to trauma history (p = 0.652), the presence of an anatomical causative lesion (p = 1.000), symptom duration (p = 0.365), age (p = 0.975), or sex (p = 0.688) with respect to clinical outcomes. Of 5 patients that did not experience symptom recovery, patients with preoperative normal NCS (n = 4, p =
0.008) and bilateral symptom (n = 3, p = 0.304) showed no clinical improvement.
4) Radiological and operative evaluation findings All 33 patients underwent ankle MRI at the sympto- matic foot before decompression. Eighteen patients (54.5%) had abnormal radiological finding involving the tarsal tunnel, that is, ganglion cyst (n = 5), vein engorgement (n = 4), bony coalition (n = 3), accessory muscle belly (n = 3), or tenosynovitis (n = 3). Operative finding revealed more causative lesions involving the tarsal tunnel that were not observed by preoperative radiology, and some of them were overlapped. These were hypertrophied muscle or thickened fascia (n = 8), vein engorgement (n = 13), ganglion cyst (n = 5), bony coalition or mass (n = 4), nerve branch entrapment (n
= 1), and accessory muscle belly (n = 3). Six patients (18.2%) had no specific lesion in MRI or surgical field, and underwent simple adhesiolysis (Supplementary Table and Fig. 2).
Discussion
Tarsal tunnel syndrome (TTS) is caused by nerve compression in the tarsal tunnel, and can arise from ankle trauma, space-occupying lesions, bony defor-
Table 2. Comparison NCS Results before and after Operation
Preoperation Postoperation p-value
†Tarsal tunnel decompression at the right ankle (n=17)
Right medial plantar nerve
DML (ms) 4.9 ± 1.0 4.7 ± 0.6 0.202
MCV (m/s) 41.0 ± 6.5 42.5 ± 4.6 0.323 SCV (m/s) 37.0 ± 11.6 40.1 ± 12.2 0.008
†Right lateral plantar nerve
DML (ms) 5.1 ± 1.1 4.9 ± 0.6 0.290
MCV (m/s) 41.2 ± 4.8 44.6 ± 4.2 0.030
†SCV (m/s) 39.2 ± 6.0 41.8 ± 5.7 < 0.001
†Tarsal tunnel decompression at the left ankle (n=16)
Left medial plantar nerve
DML (ms) 5.1 ± 0.7 4.8 ± 0.7 0.297
MCV (m/s) 40.2 ± 6.2 41.0 ± 4.0 0.334 SCV (m/s) 40.9 ± 6.6 43.6 ± 5.1 0.135 Left lateral plantar nerve
DML (ms) 5.2 ± 0.7 5.0 ± 0.7 0.140
MCV (m/s) 38.6 ± 11.6 41.8 ± 5.4 0.033
†SCV (m/s) 41.0 ± 7.7 43.8 ± 5.5 0.093 NCS: nerve conduction study, DML: distal motor latency, MCV: motor nerve conduction velocity, SCV: sensory nerve conduction velocity, SAP: sensory action potential
*All values were expressed as mean ± standard deviation.
†p < 0.05
Pre-operation 4
3
2
Severity grade 1
0
Post-operation 24
Fig. 1. Changes of electrophysiological severity before and after opera-
tion. According to the result of plantar nerve conduction velocity (CV)
and distal motor latency (DML), electrophysiological severity was
scored and compared before and after operation. After operation,
median grade of electrophysiological severity was improved from 2
to 0 (normal) using Wilcoxon signed rank test (p < 0.001).
mities, hypertrophied muscle or tendinopathy, hind foot varus or valgus, a systemic condition, such as, diabetes, hypothyroidism, rheumatoid arthritis, gout, pregnancy, or others.
2,8Many cases of TTS remain idiopathic, but recent advances in diagnostic radiology increasingly enable the identification of structural abnormalities.
In particular, MR imaging with its excellent soft tissue contrast and ability to demonstrate musculotendinous and neurovascular structures, clearly demonstrates the anatomy of the tarsal tunnel and its contents and the presence and extent of causative lesions.
9In one MRI study, abnormal findings were observed in 85% of patients with TTS.
10Furthermore, this information aids when deciding on surgical treatment and determining the extent of decompression required. In the present study, anatomical lesions were evident in 18 patients by ankle MRI, and 15 of these concurred with operative findings; in the other 3 findings differed (case No. 8,
11, and 23). Nine causative lesions, which were not remarkable by MRI, were newly identified during operation. Operative findings confirmed the presence of two or more causative lesions in 7 patients. The most commonly reported anatomical etiology of TTS by small operational case series varies. One research reported that etiology frequencies of ganglion cyst (36%), talocalcaneal coalition (30%), idiopathic (18%), and traumatic (10%).
11In our series, hypertrophied muscle or thickened fascia and vessel engorgement was the most prevalent, and no relation was found between type of etiology and postoperative outcome. MRI results showed good accuracy for determining the presence of a ganglion cyst, an accessory muscle, or bony coalition, whereas demonstrated relatively low detection rate of a vessel engorgement or a thickened fascia. In view of the limitations of electrophysiological studies, which cannot suggest candidates for operative treatment, MRI
Fig. 2. MRI and operative findings of
one patient (case No. 20). Her ankle
MRI revealed complicated ganglion
cyst within flexor retinaculum and
consisted with operative result. It was
excised and the pathologic result was
compatible with ganglion cyst.
is still necessary for the proper evaluation of TTS.
A complete electrophysiological study involves a nerve conduction study (NCS) and electromyography (EMG), and may provide further information about the degree of individual nerve functional deficits, exclude other associated peripheral neuropathies, and allow assessments of temporal changes after treatment, and thus, they are essential diagnostic tools. Although no international guidelines have been issued regarding clinical and electrophysiological diagnostic criteria,
12slow sensory nerve conduction and the absence of sensory action potentials of plantar nerves are the most consistent diagnostic findings for TTS, and are present in 90.5% of patients.
13-15Measurements of motor NCVs and prolonged distal motor latencies are easily obtained and aid the diagnosis,
16but are less sensitive and are only present in 52.4%.
13The clinical and electrophysiological outcomes of tarsal tunnel decompression have been reported on a few occasions. Proportions of clinical successes have been reported to be 44% (14 of 32 cases), 43% (9 of 21 cases), or 51%, whereas electrophysiological improvement were higher.
17-19In this study, symptomatic improve- ment was achieved in 28 feet (84.8%), and 23 feet (69.7%) had good electrophysiological outcomes after decompression. These surgical outcomes are more satisfactory than those reported in previous studies.
The present study concurs with other studies that abnormalities in sensory nerve conduction (21 of 33, 63.6%) are more frequently detected than abnormalities in motor nerve conduction (13 of 33, 39.4%). However, unlike previous studies, in which abnormalities were more frequently associated with the lateral plantar nerve than the medial plantar nerve,
13,14in the present study, abnormalities were associated equally with these both plantar nerves before decompression.
Historically, the success rate of tarsal tunnel decom pression has been reported to vary from 44% to 96%.
11,17,18,20The factors that contribute to a poor prognosis are old age, chronic symptoms, accompanying muscle weakness and atrophy, a female gender, and an idiopathic or
posttraumatic etiology.
17,21-23Alternatively, the presence of a space-occupying lesion and a positive Tinel’s sign are strongest predictors of a favorable outcome.
11,22,24In the present study, decompression showed favorable outcome in clinical symptoms and electrophysiological results. Somewhat surprisingly, no factor was found to be significantly related with outcome. Nevertheless, we speculate that preoperative normal NCS results and bilateral symptoms predict a poor surgical response by looking into our case series.
This study has some limitations that should be considered, that is, a small number of patients were recruited, and the subjects were not evenly distributed in terms of their preoperative functional or electro- physiological severity. Despite this, we believe that tarsal tunnel decompression can be considered favorable treatment option and warranted when the effect of conservative treatment is not obtained.
Conclusion
Summarizing, 28 of the 33 TTS patients (84.8%) that underwent decompressive operation achieved enough pain relief and 23 of the 33 (69.7%) had improved electrophysiological results after operation.
Preoperative MR results were found to be positive in 18 of the 33 patients (54.5%). It appears that tarsal tunnel decompression is warranted in patients that remain symptomatic after prolonged conservative treatment.
Supplementary Materials
Supplementary materials can be found via http://dx.
doi.org/10.18214/jkaem.2015.17.2.69
References
1. Antoniadis G, Scheglmann K. Posterior tarsal tunnel syndrome: diagnosis and treatment. Deutsches Arzteblatt international 2008: 105: 776-781
2. Ahmad M, Tsang K, Mackenney PJ, Adedapo AO. Tarsal
tunnel syndrome: A literature review. Foot and ankle surgery:
official journal of the European Society of Foot and Ankle Surgeons 2012: 18: 149-152
3. Amato A, Dumitru D, Zwarts M: Electrodiagnostic medicine, 2nd ed, Philadelphia: HANLEY & BELFUS; 2002, pp216-217 4. Oh S: Clinical electromyography: nerve conduction studies,
3th ed Philadelphia: Lippincott Williams & Wilkins; 2003, pp281-282
5. Mondelli M, Giannini F, Reale F. Clinical and electrophy- siological findings and follow-up in tarsal tunnel syndrome.
Electroencephalogr Clin Neurophysiol 1998: 109: 418-425 6. Felsenthal G, Butler DH, Shear MS. Across-tarsal-tunnel
motor-nerve conduction technique. Arch Phys Med Rehabil 1992: 73: 64-69
7. Mondelli M, Morana P, Padua L. An electrophysiological severity scale in tarsal tunnel syndrome. Acta Neurol Scand 2004: 109: 284-289
8. DeLisa JA, Saeed MA. The tarsal tunnel syndrome. Muscle Nerve 1983: 6: 664-670
9. Finkel JE. Tarsal tunnel syndrome. Magn Reson Imaging Clin N Am 1994: 2: 67-78
10. Frey C, Kerr R. Magnetic resonance imaging and the evaluation of tarsal tunnel syndrome. Foot & ankle 1993: 14:
159-164
11. Takakura Y, Kitada C, Sugimoto K, Tanaka Y, Tamai S. Tarsal tunnel syndrome. Causes and results of operative treatment. J Bone Joint Surg Br 1991: 73: 125-128
12. Bilbao A, Wilcox MS. Tarsal tunnel revisited. Muscle Nerve 1995: 18: 791
13. Oh SJ, Sarala PK, Kuba T, Elmore RS. Tarsal tunnel syndrome:
electrophysiological study. Ann Neurol 1979: 5: 327-330 14. Galardi G, Amadio S, Maderna L, Meraviglia MV, Brunati L,
Dal Conte G, et al. Electrophysiologic studies in tarsal tunnel
syndrome. Diagnostic reliability of motor distal latency, mixed nerve and sensory nerve conduction studies. Am J Phys Med Rehabil 1994: 73: 193-198
15. Patel AT, Gaines K, Malamut R, Park TA, Toro DR, Holland N.
Usefulness of electrodiagnostic techniques in the evaluation of suspected tarsal tunnel syndrome: an evidence-based review. Muscle Nerve 2005: 32: 236-240
16. Fu R, DeLisa JA, Kraft GH. Motor nerve latencies through the tarsal tunnel in normal adult subjects: standard determinations corrected for temperature and distance. Arch Phys Med Rehabil 1980: 61: 243-248
17. Pfeiffer WH, Cracchiolo A, 3rd. Clinical results after tarsal tunnel decompression. J Bone Joint Surg Am 1994: 76: 1222- 1230.
18. Kaplan PE, Kernahan WT, Jr. Tarsal tunnel syndrome: an electrodiagnostic and surgical correlation. J Bone Joint Surg Am 1981: 63: 96-99
19. Gondring WH, Shields B, Wenger S. An outcomes analysis of surgical treatment of tarsal tunnel syndrome. Foot Ankle Int 2003: 24: 545-550
20. Hendrix CL, Jolly GP, Garbalosa JC, Blume P, DosRemedios E.
Entrapment neuropathy: the etiology of intractable chronic heel pain syndrome. J Foot Ankle Surg 1998: 37: 273-279 21. Lam SJ. A tarsal-tunnel syndrome. Lancet. 1962: 2: 1354-1355 22. Sammarco GJ, Chang L. Outcome of surgical treatment of
tarsal tunnel syndrome. Foot Ankle Int 2003: 24: 125-131 23. Skalley TC, Schon LC, Hinton RY, Myerson MS. Clinical results
following revision tibial nerve release. Foot Ankle Int 1994:
15: 360-367
24. Nagaoka M, Satou K. Tarsal tunnel syndrome caused by
ganglia. J Bone Joint Surg Br 1999: 81: 607-610
Case No.
Sex/
Age
MRI finding Operative finding Clinical outcome NCS outcome
1 F/55 No remarkable finding
Flexor retinaculum hypertrophy
Improved Worse
2 F/45
Accessory muscle belly in flexor retinaculum
Same Improved Improved
3 F/23 Ganglion cysts Same Improved Improved
4 M/32 No remarkable finding Adhesion No change No change
†5 F/48 Ganglion cyst
1. Ganglion cyst 2. Tortuous vein
Improved Improved
6 M/58 No remarkable finding
1. Varicose vein 2. Thickened FHL & AH
fascia
Improved No change
*7 F/52 Ganglion cyst Same Improved Improved
8 M/65
Tenosynovitis (tibialis posterior)
1. Flexor retinaculum hypertrophy 2. Thickened AH fascia 3. Vein engorgement and
adhesion
Improved Improved
9 F/62 No remarkable finding
1. Varicose vein 2. Thickened abductor
hallucis fascia 3. Peroneous brevis
muscle tendon tear
No change Improved
10 F/59 No remarkable finding Adhesion Improved Improved
11 F/58
Tenosynovitis (tibialis posterior)
1. Varicose vein 2. Adhesion
Improved Improved
14 M/20 No remarkable finding Adhesion Improved Improved
15 F/56 Talocalcaneal coalition Same Improved Improved
16 M/50 No remarkable finding
Flexor retinaculum hypetrophy
Improved Improved
17 M/58 Vein engorgement
1. Thickened AH fascia 2. Enlarged posterior
tibial artery
Improved Improved
18 M/59 Vein engorgement
Tortuous posterior tibial artery and vein
Improved No change
†19 M/48 No remarkable finding Adhesion Improved Improved
20 M/62 Ganglion cyst Same Improved Improved
21 M/38 No remarkable finding
Hypertrophied AH muscle
Improved Improved
22 F/72 No remarkable finding
Lateral plantar nerve entrapment and severe
degeneration
Improved No change
†23 F/59
Tenosynovitis (tibialis posterior)
Varicose vein No change No change
†24 M/25
FDL accessory muscle belly in the tarsal tunnel
Same No change No change
†25 M/46
FDL accessory muscle belly in the tarsal tunnel
1. Same 2. Round bony mass at
the medial malleolus
Improved Improved
26 F/63 No remarkable finding Adhesion Improved No change
†27 M/53
Varicose vein Tenosynovitis (tibialis
posterior)
1. Varicose vein 2. Adhesion
Improved Improved
28 F/27 No remarkable finding
3. Lateral plantar nerve hypertrophy
Improved Improved
29 F/53 No remarkable finding Adhesion Improved No change
†30 F/57 No remarkable finding Varicose vein Improved Improved
31 F/63 No remarkable finding Varicose vein Improved No change
†32 M/24 Talocalcaneal coalition Same Improved Improved
33 F/46 Ganglion cyst Same Improved Improved
NCS: nerve conduction study, AH: abductor hallucis, FDL: flexor digitorum longus, FHL: flexor hallucis longus
*