INTRODUCTION
Mesenchymal stem cells (MSCs) are cells that have been demonstrated to have the ability to differentiate into distinct mesenchymal tissues such as bones, tendons, muscles, adi- pose tissues, cartilage and nerve tissues as well as to support hematopoiesis (1-5). MSCs have been labeled in a variety of ways since Dexter named them ‘stromal cells’ in the 1980’s (6). Caplan designated the term mesenchymal stem cells in the 1990’s (7), while others still refer to them as marrow stro- mal cells. The methods used for preparation of these cells have not yet been standardized; the differential potential of MSCs has not yet been fully determined due to the limita-
tions of in vitro expansion. Since Noort et al. reported that MSCs promote engraftment of umbilical cord blood-derived CD34+ cells in non-obese diabetic/severe combined immun- odeficiency (NOD/SCID) mice (8, 9) many clinical trials have been pursued to better understand their role in bone marrow transplantation (10). Unlike transplantation of hematopoi- etic stem cells (HSCs) only, the questions regarding in vitro expansion remain unanswered; in particular, questions regard- ing the optimal infusion buffer and whether to use thawed cells or fresh detached cells for cotransplantation of MSCs and HSCs remain unanswered. We studied the optimal ratio of HSCs to MSCs to facilitate engraftment, and tried to deter- mine the appropriate ratio for enhancement of HSCs.
Dong Hyun Kim*,�, Keon Hee Yoo�, Young Sook Yim�, Jaewon Choi�, Soo Hyun Lee�, Hye Lim Jung�, Ki Woong Sung�, Sung-Eun Yang�, Won Il Oh�, Yoon-Sun Yang�, Sang-Hee Kim�, Sang-Yun Choi*, Hong Hoe Koo�
School of Life Sciences and Biotechnology*, Korea University, Seoul; Department of Pediatrics�, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul; Department of Research and Development for Cellular Therapy�, Medipost Biomedical Research Institute, Seoul; Korea Food Research Institute�, Seoul, Korea
Dong Hyun Kim and Keon Hee Yoo contributed equally to this work.
Address for correspondence Hong Hoe Koo, M.D.
Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, 50 Ilwon-dong, Gangnam-gu, Seoul 135-710, Korea Tel : +82.2-3410-3524, Fax : +82.2-3410-0043 E-mail : [email protected]
*This study was supported by a grant from Samsung Biomedical Research Institute grant, #SBRI C-A5-203- 2 and the Korea Health 21 R&D Project, Ministry of Health and Welfare, Republic of Korea (0405-DB000- 0101-0016) and IN-SUNG Foundation for Medical Research.
1000
Cotransplanted Bone Marrow Derived Mesenchymal Stem Cells (MSC) Enhanced Engraftment of Hematopoietic Stem Cells in a MSC-dose Dependent Manner in NOD/SCID Mice
Transplantation of marrow-derived mesenchymal stem cells (MSCs), expanded by culture in addition to whole bone marrow, has been shown to enhance engraftment of human hematopoietic stem cells (HSCs). Our hypothesis was that there might be an optimum ratio range that could enhance engraftment. We examined the per- cent donor chimerism according to the ratio of HSCs to MSCs in non-obese diabetic/
severe combined immunodeficiency (NOD/SCID) mice. We tested a series of ratios of co-transplanted CD34+-selected bone marrow cells, and marrow-derived MSCs into sublethally irradiated NOD/SCID mice. In all experiments, 1×105bone marrow derived human CD34+ cells were administered to each mouse and human MSCs from different donors were infused concomitantly. We repeated the procedure three times and evaluated engraftment with flow cytometry four weeks after each trans- plantation. Serial ratios of HSCs to MSCs were 1:0, 1:1, 1:2 and 1:4, in the first ex- periment, 1:0, 1:1, 1:2, 1:4 and 1:8 in the second and 1:0, 1:1, 1:4, 1:8 and 1:16 in the third. Cotransplantation of HSCs and MSCs enhanced engraftment as the dose of MSCs increased. Our results suggest that the optimal ratio of HSCs and MSCs for cotransplantation might be in the range of 1:8-1:16; whereas, an excessive dose of MSCs might decrease engraftment efficiency.
Key Words : Hematopoietic Stem Cells; Mesenchymal Stem Cells; Transplantation; Mice, SCID; Engraftment
Received : 8 March 2006 Accepted : 16 May 2006
MATERIALS AND METHODS Human CD34+ cells and MSCs isolation
Human CD34+ cells were collected by bone marrow aspi- ration from 34 to 57 yr-old healthy volunteers (Table 1) under an Institutional Review Board approval protocol of Samsung Medical Center, Korea. CD34+ cells were isolated using the MACS sort system (Miltenyi Biotec GmbH, Germany). The purity of the CD34+-selected cells was more than 90%. MSCs were cultured as previously described (11). We used bone marrow derived MSCs that were not exceeded over 3 passages.
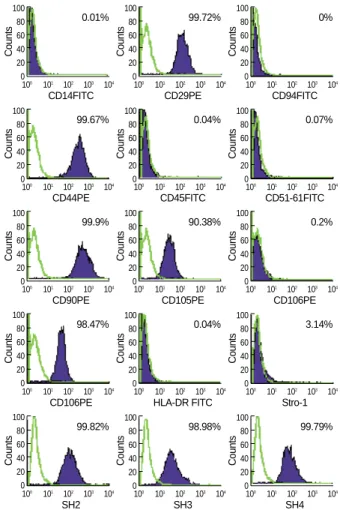
MSCs were confirmed to be negative for hematopoietic mar- kers by flow cytometry. For further clarification of MSCs, the following antibodies were used: CD14 (BD-Pharmingen, Palo Alto, CA, U.S.A.), CD29, CD34, CD44, CD45, CD51- 61, CD90, CD105, CD106, CD166, HLA-DR, Stro-1, SH2- M2, SH3-M2 and SH4-M2.
Cotransplantation of MSCs and HSCs into NOD/SCID mouse
NOD/SCID mice, purchased from Jackson Laboratories (MA, U.S.A.) were maintained in microisolator cages in spe- cific pathogen free conditions. Eight-week old mice received sublethal total-body irradiation with 300 cGy from 137-Cs source within 24 hr before transplantation. In all experiments, 1×105bone marrow derived human CD34+ cells were ad-
HSCs Sex Age (yr)
MSCs Sex Age (yr)
Exp. 1 Male 40 Male 35
Exp. 2 Male 35 Male 34
Exp. 3 Female 57 Male 35
Table 1.Donor information of each experiment
FL2-Height
104
103
102
101
100
100 101 102 103 104 FL1-Height
Isotype
1029.001
Fig. 1.Isolation of HSCs from bone marrow and results of FACS analyses. HSCs were isolated by MACS sort system from bone marrow.
The purity of HSCs infused to NOD/SCID mice was more than 90%. (A) Isotypes were stained with FITC-anti-mouse IgG1 and PE-anti- mouse IgG1. (B) Dot plots show FITC-anti-human CD34 on x-axis and PE-anti-human CD38 on y-axis. (C) Isolated CD34+ cells were sta- ined PE-anti-human CD34 only on y-axis.
A
FL2-Height
104
103
102
101
100
100 101 102 103 104 FL1-Height
CD 34/38
1029.002
22.38% 38.75%
36.09%
B
FL2-Height
104
103
102
101
100
100 101 102 103 104 FL1-Height
CD 34PE
1029.003
C 95.72%
Counts
100 80 60 40 20 0
100 101 102 103 104 CD14FITC
0.01%
Counts
100 80 60 40 20 0
100 101 102 103 104 CD29PE
99.72%
Counts
100 80 60 40 20 0
100 101 102 103 104 CD94FITC
0%
Counts
100 80 60 40 20 0
100 101 102 103 104 CD44PE
99.67%
Counts
100 80 60 40 20 0
100 101 102 103 104 CD45FITC
0.04%
Counts
100 80 60 40 20 0
100 101 102 103 104 CD51-61FITC
0.07%
Counts
100 80 60 40 20 0
100 101 102 103 104 CD90PE
99.9%
Counts
100 80 60 40 20 0
100 101 102 103 104 CD105PE
90.38%
Counts
100 80 60 40 20 0
100 101 102 103 104 CD106PE
0.2%
Counts
100 80 60 40 20 0
100 101 102 103 104 CD106PE
98.47%
Counts
100 80 60 40 20 0
100 101 102 103 104 HLA-DR FITC
0.04%
Counts
100 80 60 40 20 0
100 101 102 103 104 Stro-1
3.14%
Counts
100 80 60 40 20 0
100 101 102 103 104 SH2
99.82%
Counts
100 80 60 40 20 0
100 101 102 103 104 SH3
98.98%
Counts
100 80 60 40 20 0
100 101 102 103 104 SH4
99.79%
Fig. 2.Results of MSCs phenotypes by FACS analysis. MSCs that were used in this test were positive for CD29 (BD-Pharmingen, Palo Alto, CA, U.S.A.), CD44, CD90, CD105, CD166, SH2, SH3, and SH4, while negative for CD14, CD34, CD45, CD51-61, CD106 and HLA-DR. Stro-1 was weakly expressed. Blank peaks indicate the isotype of each cell and closed peaks represent expression of each marker.
ministered to each mouse and MSCs were used concomitantly.
Bone marrow derived CD34+ cells and MSCs were inject- ed in a final volume of 500 to 1,000 L HBSS (Bio-Whit- taker, Baltimore, MD, U.S.A.) per mouse and were infused via tail vein injection. Three experiments were performed repeatedly. Serial ratios of bone marrow derived CD34+ cells to MSCs were 1:0, 1:1, 1:2 and 1:4, in the first experiment (4 mice), 1:0, 1:1, 1:2, 1:4 and 1:8 in the second (10 mice) and 1:0, 1:1, 1:4, 1:8 and 1:16 in the third (15 mice).
Analysis of human CD34+ cell engraftment
Mice were sacrificed 4 weeks posttransplant and cells from the bone marrow were analyzed by flow cytometry. Cells were then incubated with PE-mouse anti-human CD45 (BD-Phar- mingen, Palo Alto, CA, U.S.A.) for 30 min at 4℃, washed, resuspended in 1% paraformaldehyde in phosphate-buffered saline, and analyzed on a flow cytometry (FACS Vantage, Becton Dickinson, Palo Alto, CA, U.S.A.).
Statistical analysis
Mann-Whitney test (SPSS 12.0 for Windows. SPSS Inc.) was used to calculate differences between the HSCs only group and the cotransplant group. A p-value of less than 0.05 was considered statistically significant.
RESULTS
The immunophenotye of bone marrow derived HSCs We isolated CD34+ HSCs from bone marrow using CD- 34+ cell directed kit (Miltenyi Biotec GmbH, Germany), and at the same time, isolated MSCs from CD34- population.
The CD34+ cells infused had purities over 90% and CD34+/
CD38- cells were in the range of 30±5-40±5% (data not shown) (Fig. 1).
The immunophenotyes of bone marrow derived MSCs
FACS results showed that CD29, CD44, CD90, CD105, CD166, SH2, SH3, and SH4 were expressed in more than 90% of MSCs. Typical hematopoietic antigens (CD14, CD34 and CD45) as well as CD51-61, CD106 and HLA-DR known to be negative markers for MSCs (2, 12, 13) were hardly ex- pressed. On the other hand, Stro-1, known to be related with homing to bone marrow (14), was expressed in 3.14% of MSCs (Fig. 2).
Effect of MSCs on engraftment according to cell dose
We observed that the engraftment efficiency after cotrans- plantation was improved as the MSCs dose was increased up to a certain level in all three independent experiments. The
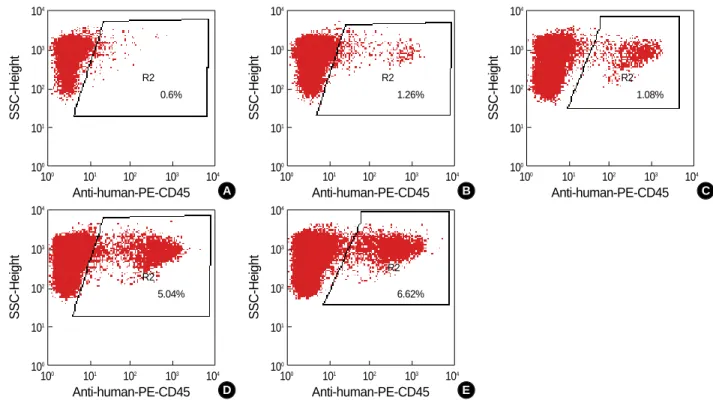
Fig. 3.MSCs enhanced human cell engraftment in bone marrow of NOD/SCID mice in a dose-dependent manner at 4 weeks posttrans- plant. (A) CD34+ only group (1.0×105cells). (B) The ratio of CD34+ to MSCs was 1:1 (1.0×105cells each). (C) The ratio of CD34+ to MSCs was 1:2 (1.0×105:2.0×105cells). (D) The ratio of CD34+ to MSC was 1:4 (1.0×105:4.0×105cells). (E) The ratio of CD34+ to MSC was 1:8 (1.0×105:8.0×105cells). This is representative of 2 analyses in the experiment 2.
SSC-Height
104
103
102
101
100
100 101 102 103 104 Anti-human-PE-CD45
0.6%
R2
A
SSC-Height
104
103
102
101
100
100 101 102 103 104 Anti-human-PE-CD45
1.26%
R2
B
SSC-Height
104
103
102
101
100
100 101 102 103 104 Anti-human-PE-CD45
1.08%
R2
C
SSC-Height
104
103
102
101
100
100 101 102 103 104 Anti-human-PE-CD45
5.04%
R2
D
SSC-Height
104
103
102
101
100
100 101 102 103 104 Anti-human-PE-CD45
6.62%
R2
E
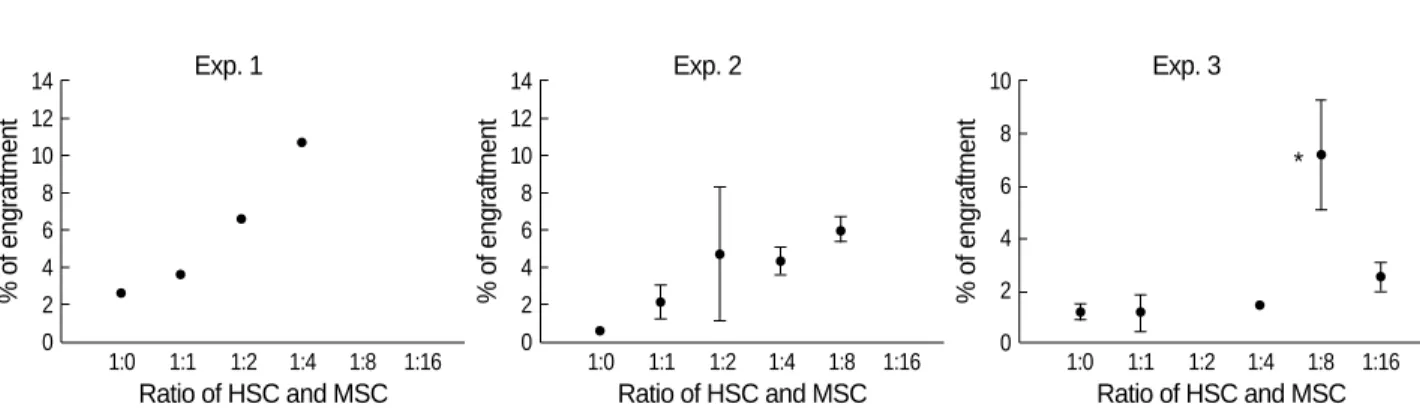
engraftment fold-increase of the 1:4 group was 3.99, 19.78 and 6.03 compared to the HSCs only group in experiment 1, 2 and 3, respectively (Table 2). The percent donor chime- rism of the 1:16 group was inferior to that of the 1:8 ratio group (Fig. 3). The 1:4 and 1:8 ratio groups were associated with a higher percent donor chimerism than any other group studied (Fig. 4).
DISCUSSION
MSCs have recently been used experimentally in clinical trials of cardiovascular repair (15, 16), treatment of lung fibro- sis (17), spinal cord injury (18) and bone and cartilage repair (4, 19) as a stem cell source. MSCs have been successfully used for therapeutic application when they are derived from bone marrow (20).
Generally, an accepted range of HSC dose for engraftment after bone marrow transplantation is 3-4×106CD34+ cells/kg of recipient body weight for humans. Considering that a mouse weighs about 30 g on average, we postulated that 9-12×104
CD34+ cells should be a reasonable dose range for a mouse, and therefore infused 1×105CD34+ cells.
Usually, the fluorescence intensity of CD34+ cells when conjugated with FITC is weaker than that when conjugated with PE using flow cytometry. Therefore, it is a matter of course that the percentage of CD34+ fraction may is differ- ent to some extent according to the conjugated materials even though the testing samples are exactly the same. Authors usu- ally evaluate the purity of overall CD34+ cell fraction stained with PE according to the manufacturer’s protocol of CD34 sort kit (Miltenyi Biotec, Germany). Fig. 1B is intended to show the percentage of CD34+/CD38- fraction which is known to be more primitive and have higher engraftment potential than CD34+/CD38+ fraction using PE-conjugat- ed CD38 and FITC-conjugated CD34.
At present we do not know how long MSCs will maintain innate characteristics including the ability to differentiate and cytokine production; nor do we know what the best compo- sition culture media should contain for maintaining MSCs.
We used early MSCs not exceeding 3 passages based on the assumption that early passage cells would be more likely to have the innate characteristics of MSCs.
Cotransplantation of HSCs and MSCs enhanced engraft- ment as the dose of the MSCs were increased up until a 1:8 ratio. The percent donor chimerism in the 1:16 group, how- ever, was lower than that of the 1:8 group even though it was still higher than the HSCs only group as shown in the expe- riment 3. These findings suggest that HSCs and MSCs have a threshold ratio of HSCs to MSCs for enhancing engraftment when cotransplanted into a NOD/SCID mouse. Our findings suggest that the optimal ratio of HSCs to MSCs in cotrans- plantation might be between 1:8 and 1:16 and we are con- ducting further experiments using these ratios. We confirmed MSCs engraftment enhancing ability in 3 experiments. Each experiment was performed with bone marrow-derived MSCs obtained from a different volunteer donor, and showed differ- ent enhancing abilities. For example, the mean fold-increase of the 1:4 ratio group was 3.99 compared with the HSCs only group in the experiment 1, while it was 7.21 in the experi- ment 2, and 1.21 in the experiment 3. The CD34+ cells were
Fig. 4.Results of contransplantation. In all experiments, the engraftment in bone marrow was increased as the MSCs dose was increased.
In experiment 3, the engraftment in the group of a 1:16 ratio is inferior to that of a 1:8 ratio. *Indicates significant statistical difference between the CD34+ only group and a cotransplanted group.
% of engraftment
14 12 10 8 6 4 2
0 1:0 1:1 1:2 1:4 1:8 1:16 Ratio of HSC and MSC
% of engraftment
14 12 10 8 6 4 2
0 1:0 1:1 1:2 1:4 1:8 1:16 Ratio of HSC and MSC
% of engraftment
10 8 6 4 2
0 1:0 1:1 1:2 1:4 1:8 1:16 Ratio of HSC and MSC
Exp. 3 Exp. 2
Exp. 1
*
Ratio (HSCs:MSCs)
% of engraftment in bone marrow
No. of mouse/ratio
group 1:0 1:1 1:2 1:4 1:8 1:16
CD34+ dose 1 1 1 1 1 1
(×105)
MSCs dose 0 1 2 4 8 16
(×105)
Exp. 1 2.66 3.62 6.57 10.62 NA NA 1
Exp. 2 0.6 1.26 1.08 3.61 6.62 NA 2
* 3.1 8.28 5.04 5.25
Exp. 3 0.59 0.64 NA 1.29 4.55 1.67 3
1.25 0.26 1.68 5.64 2.35 1.73 2.56 1.35 11.34 3.43 Table 2.Summary of bone marrow engraftment
NA, not applicable. *, expired at 2 weeks later after transplantation.
also derived from different donors; however, it is unlikely that the quality of MSCs is the sole determinant of engraftment efficiency. It is clear that the CD34+ cell dose has been shown to be strongly associated with engraftment kinetics regard- less of individual differences (21, 22).
In addition, the proliferation rate and morphology of the 3 MSCs experiments differed when observed during cell ex- pansion before cotransplantation (data not shown). There- fore, our findings suggest that the engraftment enhancing ability of MSCs might have considerable difference accord- ing to the MSC donor.
Our study demonstrated that MSCs could enhance engraft- ment in a dose-dependent manner up to a certain level in NOD/SCID mice. Future studies should help elucidate fur- ther mechanisms associated with engraftment such as secre- tion of specific MSC-cytokines that help enhance engraft- ment. For clinical application to human patients character- istics of MSCs including immunosuppression and HLA res- triction require further explanation.
REFERENCES
1. Majumdar MK, Thiede MA, Mosca JD, Moorman M, Gerson SL.
Phenotypic and functional comparison of cultures of marrow-derived mesenchymal stem cells (MSCs) and stromal cells. J Cell Physiol 1998; 176: 57-66.
2. Pittenger MF, Mackay AM, Beck SC, Jaiswal RK, Douglas R, Mosca JD, Moorman MA, Simonetti DW, Craig S, Marshak DR. Multilin- eage potential of adult human mesenchymal stem cells. Science 1999;
284: 143-7.
3. Johnstone B, Hering TM, Caplan AI, Goldberg VM, Yoo JU. In vitro chondrogenesis of bone marrow-derived mesenchymal progenitor cells. Exp Cell Res 1998; 10: 265-72.
4. Bruder SP, Fink DJ, Caplan AI. Mesenchymal stem cells in bone development, bone repair, and skeletal regeneration therapy. J Cell Biochem 1994; 56: 283-94.
5. Gimble J, Guilak F. Adipose-derived adult stem cells: isolation, charac- terization, and differentiation potential. Cytotherapy 2003; 5: 362-9.
6. Dexter TM. Stromal cell associated haemopoiesis. J Cell Physiol Suppl 1982; 1: 87-94.
7. Caplan AI. Osteogenesis imperfecta, rehabilitation medicine, funda- mental research and mesenchymal stem cells. Connect Tissue Res 1995; 31: 9-14.
8. Noort WA, Kruisselbrink AB, in’t Anker PS, Kruger M, van Bezooi- jen RL, de Paus RA, Heemskerk MH, Lowik CW, Falkenburg JH, Willemze R, Fibbe WE. Mesenchymal stem cells promote engraft- ment of human umbilical cord blood-derived CD34(+) cells in NOD/
SCID mice. Exp Hematol 2002; 30: 870-8.
9. Erices AA, Allers CI, Conget PA, Rojas CV, Minguell JJ. Human cord blood-derived mesenchymal stem cells home and survive in the
marrow of immunodeficient mice after systemic infusion. Cell Trans- plant 2003; 12: 555-61.
10. Devine SM, Hoffman R. Role of mesenchymal stem cells in hemato- poietic stem cell transplantation. Curr Opin Hematol 2000; 7: 358- 63.
11. Kim DH, Yoo KH, Choi KS, Choi J, Choi SY, Yang SE, Yang YS, Im HJ, Kim KH, Jung HL, Sung KW, Koo HH. Gene expression profile of cytokine and growth factor during differentiation of bone marrow-derived mesenchymal stem cell. Cytokine 2005; 31: 119-26.
12. Haynesworth SE, Baber MA, Caplan AI. Cell surface antigens on human marrow-derived mesenchymal cells are detected by mono- clonal antibodies. Bone 1992; 13: 69-80.
13. Prockop DJ. Marrow stromal cells as stem cells for nonhematopoi- etic tissues. Science 1997; 276: 71-4.
14. Bensidhoum M, Chapel A, Francois S, Demarquay C, Mazurier C, Fouillard L, Bouchet S, Bertho JM, Gourmelon P, Aigueperse J, Char- bord P, Gorin NC, Thierry D, Lopez M. Homing of in vitro expand- ed Stro-1-or Stro-1+human mesenchymal stem cells into the NOD/
SCID mouse and their role in supporting human CD34 cell engraft- ment. Blood 2004; 103: 3313-9.
15. Rafii S, Meeus S, Dias S, Hattori K, Heissig B, Shmelkov S, Rafii D, Lyden D. Contribution of marrow-derived progenitors to vascular and cardiac regeneration. Semin Cell Dev Biol 2002; 13: 61-7.
16. Shake JG, Gruder PJ, Baugartner WA, Senechal G, Meyers J, Red- mond JM, Pittenger MF, Martin BJ. Mesenchymal stem cell implan- tation in a swine myocardial infarct model: engraftment and func- tional effects. Ann Thorac Surg 2002; 73: 1919-25.
17. Ortiz LA, Gambelli F, McBride C, Gaupp D, Baddoo M, Kaminski N, Phinney DG. Mesenchymal stem cell engraftment in lung is en- hanced in response to bleomycin exposure and ameliorates its fibrotic effects. Proc Natl Acad Sci USA 2003; 100: 8407-11.
18. Hofstter CP, Schwarz EJ, Hess D, Widenfalk J, El Manira A, Prockop DJ, Olson L. Marrow stromal cells form guiding stands in the injured spinal cord and promote recovery. Proc Natl Acad Sci USA 2001;
99: 2199-204.
19. De Kok IJ, Peter SJ, Archambault M, van den Bos C, Kadiyala S, Aukhil I, Cooper LF. Investigation of allogeneic mesenchymal stem cell-based alveolar bone formation: preliminary findings. Clin Oral Implants Res 2003; 14: 481-9.
20. Orlic D. Adult bone marrow stem cells regenerate myocardium in ischemic heart disease. Ann NY Acad Sci 2003; 996: 152-7.
21. Ketterer N, Salles G, Raba M, Espinouse D, Sonet A, Tremisi P, Dumontet C, Moullet I, Eljaafari-Corbin A, Neidhardt-Berard EM, Bouafia F, Coiffier B. High CD34+ cell counts decrease hemato- logic toxicity of autologous peripheral blood progenitor cell trans- plantation. Blood 1998; 91: 3148-55.
22. Weaver CH, Hazelton B, Birch R, Palmer P, Allen C, West W. An analysis of engraftment kinetics as a function of CD34 content of peri- pheral blood progenitor cell collection in 692 patients after the admin- istration of myeloblative chemotherapy. Blood 1995; 86: 3961-9.