관련 문서
Age-related changes in the prevalence of osteoporosis according to gender and skeletal site: The Korea National Health and Nutrition Examination Survey 2008-2010..
Objective: The purpose of this study is to investigate the relationship between depression and evening meals for adult women by using the National Health and Nutrition Survey
socioeconomic status and thyroid cancer prevalence; Based on the korean National Health and Nutrition Examination Survey2010-2011. Jung YI, Kim
Health behavior of multicultural and general family adolescents in Korea: the Korea Youth Risk.. Behavior
Prevalence of Undiagnosed Diabetes and Related Factors in Korean Postmenopausal Women:.. The 2011-2012 Korean National Health and
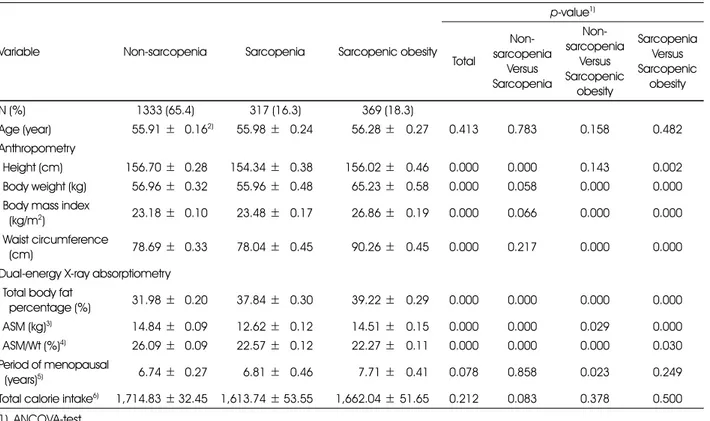
Objective: This study was conducted to identify the association between vitamin D and Sarcopenia among all adults in Korea using data from the National Health and
Objective: The purpose of this study is to use it as a basis for the health care guidelines for the muscle mass and cardiovascular disease of Korean population by
Incident major cardiovascular events (coronary artery disease, ischemic stroke, hemorrhagic stroke and cardiovascular mortality) were set as primary end points.