JKSPEN Vol. 5, No. 2, 2013
42
Received April 20, 2013 Revised May 31, 2013 Accepted July 5, 2013
Correspondence to Hyun Wook Baik
DMC Bundang Jesaeng Hospital, 20, Seohyeon-ro 180beon-gil, Bundang- gu, Seongnam 463-774, Korea
Tel: +82-31-779-0202, Fax: +82-31-779-0897, E-mail: [email protected] Copyright ⓒ 2013. The Korean Society for Parenteral and Enteral Nutrition. All Rights Reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/ by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
노화와 영양
분당제생병원 소화기내과 박지은ㆍ백현욱
Aging and Nutrition
Ji Eun Park, M.D., Hyun Wook Baik, M.D., Ph.D.
Division of Gastroenterology, Department of Internal Medicine, DMC Bundang Jesaeng Hospital, Seongnam, Korea
Malnutrition is a common health problem in people older than 65 years. In older individuals, malnutrition is asso- ciated with poor clinical outcomes and even death. These individuals particularly are characterized by inadequate nutritional intake due to various factors such as medical disease, physical impairment, age-related physiological changes, and psychological and psychosocial issues.
Furthermore, as the immune system ages, its function is compromised, and the aged person becomes more vul- nerable to harm and disease. Nutrition plays an important role in maintaining the vigor of the immune system, be- cause nutritional deficits and malnutrition can aggravate a diseased condition because of the weakened immune system. It is important to assess older individuals for mal- nutrition, particularly when weight loss or anorexia is observed. Nutritional status in older individuals is gen- erally assessed with the revised mini-nutritional asse- ssment short form, the malnutrition universal screening tool, and the nutritional risk screening 2002. A structured approach is essential for the management of unintended weight loss or malnutrition in older individuals. Studies have shown that oral nutritional supplementation, a well- established approach, can improve nutritional status and quality of life in older individuals. Pharmacological treat- ments, such as administration of megestrol acetate, dro- nabinol, testosterone, oxandrolone, and rh-growth hor- mone, require further investigation to assess whether they are fit for clinical application. (JKSPEN 2013;5(2):42-49)
Key Words: Elder nutritional physiological phenomena, Malnutrition, Immunity, Nutrition assessment, Nutritional support
중심 단어: 노인영양생리학, 영양결핍, 면역성, 영양평가, 영 양지원
INTRODUCTION
Malnutrition commonly occurs in individuals over 65 years old. Malnutrition should be understood both in terms of changes in body composition and in terms of its functional consequences.1 The pathophysiology of malnutrition includes inflammatory activity, changes in body composition and bio- logical function, deficient energy, deficient protein, and reduced fat-free mass.2
The consequences of malnutrition are well known. They in- clude delayed wound healing, diminished muscle strength, sup- pressed immune function, and increases in the number of ill- ness-related complications. The results can be prolonged lengths of stay in the hospital, reduced quality of life, and even death. In geriatric patients, malnutrition is associated with a two-fold higher risk of mortality. Malnutrition in older in- dividuals also incurs a cost to society.3,4
This article will review the prevalence and causes of malnu- trition in older individuals. We will describe the changes in the immune system associated with aging, and the assessments and nutritional support available for improving the health status of malnourished older individuals.
PREVALENCE AND CAUSES OF MALNUTRITION IN OLDER INDIVIDUALS
Many older individuals experience a decrease in total energy intake that exceeds the age-related decrease in total energy
Fig. 1. In one Korean study on the nutritional status at hospital admission, 108 elderly patients values are presented as percentage.
Hospital malnutrition is present in 22.3% of the elderly patient over 65 years old and 40.7% of the patients are at the risk of mal- nutrition and only 37% of patients were well nourished. Adapted from the article of Chung and Sohn (Korean J Community Nutr 2005;10:645-53).14
expenditure. In general, specific nutritional requirements also change with increasing age. Importantly, reduced energy intake is typically associated with insufficient intake of other nutrients, like vitamins and minerals. Specific recommendations for older individuals should emphasize the necessity of each micro- nutrient to prevent nutritional imbalance.
Various conditions can cause reduced food intake. For exam- ple, appetite can be affected by disease, physical impairment, age-related physiologic changes, and psychological and psycho- social issues. The term ‘anorexia of aging’ refers to the physio- logic reduction in appetite and food intake that accompanies normal aging.5 Average daily energy intake has been reported to decrease by up to 30% between ages 20 and 80 years old.6 Factors that contribute to anorexia of aging are a marked de- cline in the ability to taste and smell with aging, age-related changes in gut function, and changes in hormone levels, like endogenous opioids, cholecystokinin, gastric inhibitory poly- peptide, peptide YY, amylin, and glucagon like peptide-1.7 Poverty is a major social cause of malnutrition in older individuals. Also, an increasing number of older individuals live alone; older individuals may not be comfortable shopping, cooking, or eating by themselves. Psychological factors that contribute to malnutrition in older individuals include alcohol- ism, depression, dementia, or Alzheimer’s disease.8
How common is malnutrition in older individuals, actually?
The risk and prevalence of malnutrition increase with age. The prevalence of malnutrition in individuals above 60 years old was greater than in individuals under 60 years old.9 In one
study, 15% of community-dwelling, ambulatory, older indivi- duals were malnourished.10 The prevalence increased to be- tween 20% and 65% in hospitalized patients.11,12 Another study estimated that 85% of patients in nursing homes were either malnourished or at risk for malnutrition.13 One Korean study report that, among hospital patients over 65 years old, malnu- trition was present in 63%, and only 37% were well nourished (Fig. 1).14
NUTRITION AND IMMUNITY
Age-related changes in the immune system are directly or in- directly related to increases in the incidence of infectious dis- eases, cancer, and age-related diseases, like cardiovascular dis- ease, neurodegenerative diseases, diabetes, and osteoporosis.15 Aging induces dysregulation of the immune system, mainly as a result of changes in cell-mediated immunity. It is well known that older patients do not manifest as vigorous an immune re- sponse as their younger counterparts, especially in the setting of infections and sepsis. The capacity of the immune system to mount an adequate response decreases with age, starting at around 60 years old. This is primarily due to oxidative stress, because production of free radicals and proinflammatory cyto- kines increases with age. In addition, several life style factors and underlying diseases can significantly affect the immune system in each individual.16 Immunologic changes occur early in the course of nutritional depletion. Thus, malnutrition is the most common cause of secondary immune deficiency in older individuals.17 In malnourished older individuals, the changes in T cell subsets (CD3+, CD8+, and CD4+) and function (decreased interleukin [IL]-2, IL-6 release) were marked com- pared with healthy older individuals. Protein energy malnu- trition leads to severe immunodeficiency in older individuals, affection not only specific immunity (B and T lymphocytes) but also nonspecific immunity (monocytes and polymorphonuclear cells).18 Malnutrition has adverse, sometimes devastating effects on the antigen-specific arms of the immune system and on many general mechanisms of host defense.19
The immune system comprises two functional branches known as the innate and the acquired immune systems. Both branches involve a diversity of blood-borne factors (complement, antibodies, and cytokines) and cells (macrophages, poly- morphonuclear cells, and lymphocytes). Gut immunity is a part of the innate immune system. It is characterized by a non-spe-
cific, rapid response compared to adaptive immunity. Gut im- munity consists of natural barriers, phagocytes and secreted molecules, and pattern-recognition molecules, like endotoxin.
The intestinal barrier is the first line of gut immunity; it com- prises the largest interface between inner and outer environ- ments and between healthy and disease status. The intestine consists of an immunologic barrier and a non immunologic barrier. The primary purpose of the mucosal immune response is to protect the mucosa by blocking entry to microbes, toxins, and antigens by secreting and transporting IgA into the lumen of the gut; this process is mediated by a special type of memory T-cell that is capable of recruiting B cells. These cell types can be found in the lamina propia of the intestinal barrier; therefore, they can interact and receive signals from the endogenous mi- crobiota of the gut. Commensal bacteria may exert a dual func- tion; they stimulate mucosal defense mechanisms (for instance, by lactobacilli) and they maintain homeostasis of the immune response.20 Disruption of the mucosa increases intestinal permeability. This condition can result in bacterial trans- location, which can lead to systemic endotoxemia. However, gut immunity can be restored by rebuilding the intestinal muco- sa with supportive nutrients, including glutamine, probiotics, lactoferrin, IgA, and mucosal growth factor. Bovine colostrum can be a source of mucosal growth factor, IgA, and lactoferrin.
Older individuals are commonly deficient in more than one micronutrient. Several studies have examined the effects of combinations of vitamins and trace elements on immune re- sponses and the incidence of infection.21 When older hospi- talized patients were given a supplement of vitamins A, C, and E for 4 weeks, they showed a high number of CD4+ and CD8+
T-cells and an increased lymphocyte proliferative response to mitogen compared to the placebo group.22 In one study, older patients were given a low-dose, multi-micronutrient supplement that contained increased amounts of vitamin C, vitamin E, and beta-carotene. This treatment was associated with an increase in the number of T-cell subsets, enhanced lymphocyte re- sponses to mitogen, increased IL-2 production, greater natural killer cell activity, and increased response to influenza virus vaccine compared to the placebo group.23
Zinc is an important trace element for maintaining the im- mune system of older individuals. Zinc deficiency can result immune system hypoplasia, impaired immune response, poor wound healing, diminished T-cell dependent reactions, and atte- nuated chemotaxis in neutrophils and monocytes.24 Despite
these important functions, the body has only limited zinc stores, which are easily depleted; thus, the body cannot compensate for long periods of zinc deficiency. Oral zinc supplementation has demonstrated the potential for improving immunity and ef- ficiently down-regulating chronic inflammatory responses in older individuals.25
Antioxidants that act as free radical scavengers are able to protect cells and perhaps assist in repairing cells damaged by free radicals. Nutrient antioxidants, including vitamins A, C, E, and Zinc, play a pivotal role in maintaining the antioxidant/ ox- idant balance in immune cells, protecting them from oxidative stress, and preserving their function.16 These antioxidants can be provided in vitamins and mineral-rich foods, rather than in drugs.
ASSESSMENT OF MALNUTRITION
It is important to identify ‘at risk’ older individuals with screening. Weight loss is the most reliable sign of malnutri- tion.26 For example, nutritional risk and morbidity are strongly indicated when 10% or more of the usual body weight is lost over 6 months, or when 5% or more of the usual body weight is lost over 1 month.
Screening should be followed up with an assessment by an experienced professional to confirm the diagnosis and start nu- tritional treatment. No single biomarker is a strong indicator of malnutrition in older individuals. A detailed assessment typi- cally involves a combined analysis of anthropometric data, bio- chemical data, clinical data, and dietary data. Biochemical and anthropometric measurements provide an objective dimension when considered in conjunction with routine dietary nutrient in- take data.9 And nutritional assessment is complex and requires multidimensional approach in the older individuals. Many med- ical conditions affect diet and nutrition. It is important that find- ing other medical conditions, such as infection, malignancy and cardiopulmonary disease, affect to decrease appetite.
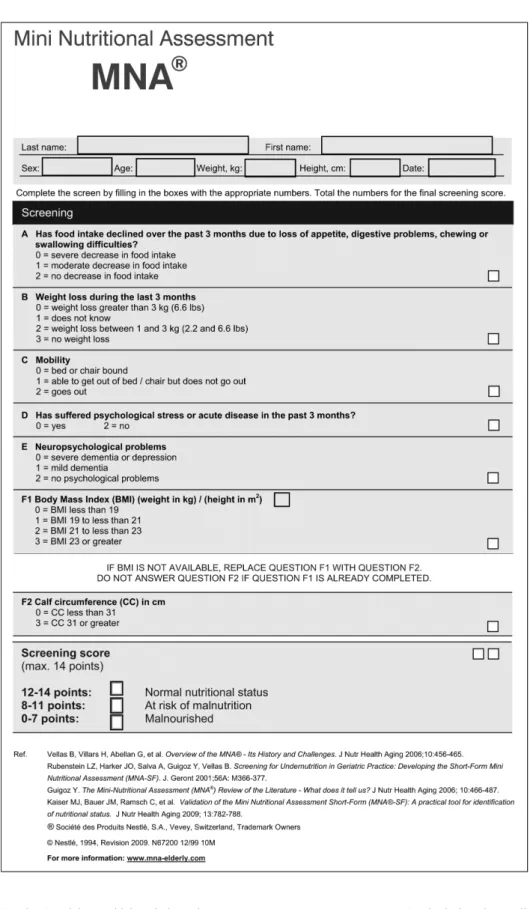
The revised mini-nutritional assessment short-form (MNA- SF, Fig. 2) retains the validity and accuracy of the original MNA for identifying older individuals that are malnourished or at risk of malnutrition. The MNA-SF consists of six items, in- cluding food intake, weight loss, mobility, psychological stress, neuropsychological problems, and body mass index (BMI).27-30 It is a rapid method that can be readily used in the clinic. It is available in Japanese, Chinese, English, French, German,
Fig. 2. The revised mini-nutritional assessment short-form.26-29
Greek, Spanish, Turkish, Thai, and Korean.
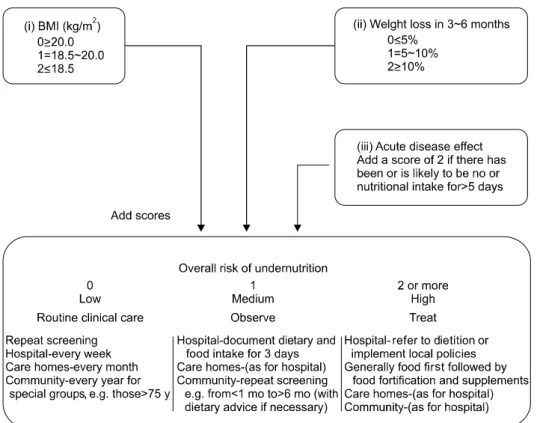
In Europe, the malnutrition universal screening tool (MUST, Fig. 3) and the nutritional risk screening 2002 (NRS 2002, Fig.
4) are established tools for assessing older individuals. The
MUST includes three clinical parameters, BMI, weight loss, and presence of acute illness; each parameter is rated as 0, 1, or 2. The MUST is regarded easy to use, and it takes approx- imately 3 to 5 minutes to complete for each individual.31 The
Fig. 3. The malnutrition universal screening tool. BMI = body mass index. Modified from the article of Stratton et al. (Br J Nutr 2004;92:
799-808).31
NRS 2002 was based on the concept that nutritional support is indicated for patients that are undernourished, or for patients with increased energy requirements, due to acute or chronic disease. It comprises an initial screening that consists of four items (BMI, weight loss, oral intake, and stress).32 When one of the screening items indicates a malnourished condition, the patient must proceed to the final screening, which consists of two components: impaired nutritional status and severity of disease. These tools for nutritional assessment can be highly subjective in evaluating older individuals; they rely on the knowledge, interpretative ability, and experience of the evaluator.
MANAGEMENT OF MALNUTRITION IN OLDER INDIVIDUALS
For older individuals with malnutrition, initial efforts should focus on increasing oral intake. A non pharmacologic strategy for improving voluntary intake is to provide frequent, small meals and oral nutritional supplementation (ONS). Guidelines from the European Society for Clinical Nutrition and Metabolism recommend intensive dietary advice and oral nutritional supple- ments to increase dietary intake. Many studies have established
the benefits of ONS. For example, after 1 month of ONS, pa- tients in the hospital with a fractured femur had fewer compli- cations and deaths than the control group.33 In a nursing-home, over a 2-month period, ONS was associated with increased body weight and nutritional status in most patients that were malnourished or at risk of malnutrition.34 Another study showed that a 3-month intervention of high protein oral supplements improved the outcome in malnourished patients with digestive diseases, both in functional status and quality of life.35 ONS intake between meals may be effective for increasing energy intake. It was found that giving ONS between meals or at least 1 hour before a meal was less likely to spoil the appetite.36 Older individuals with impaired oral intake due to neuro- muscular disease or ventilator use may be unable to meet their nutritional requirements. In these cases, a feeding tube can pro- vide access to the gut. Enteral nutrition is preferable to paren- teral nutrition. The only contraindication to enteral feeding is a mechanical obstruction to the gut. Access to the gut can be achieved with nasogastric, nasointestinal, percutaneous gastric (PEG), or percutaneous jejunal routes. Each route is associated with benefits and risks, but PEG is the most common and pre- ferred route, when enteral feeding is expected to last more than 30 days, because it provides higher safety, cost-efficiency, and
Fig. 4. The nutritional risk screening 2002. BMI = body mass index; COPD = chronic obstructive pulmonary disease; APACHE = acute physiology and chronic health evaluation. Modified from the article of Kondrup et al. (Clin Nutr 2003;22;321-36).32
comfort than the other routes. The enteral formula selection is patient-specific. All formulas contain carbohydrates, fats, and proteins. The formula should contain proteins that comprise 7%∼16% of the total calories. The recommended daily re- quirement for proteins is 0.8 g/kg/day, but in older individuals, the requirement may go up to 1.2∼1.5 g/kg/day.37
Pharmacological approaches for stimulating appetite and for treating weight loss include the administration of megesterol acetate, dronabinol, testosterone, oxandrolone, or rh-growth
hormone. Megesterol acetate is a synthetic derivative of a natu- rally occurring progestational agent that is similar to proge- sterone. It increases appetite and non fluid weight gain in a dose-dependent manner. Anabolic hormones (e.g., growth hor- mone, testosterone, oxandrolone, and nandrolone) were sug- gested as possible supplemental agents to help preserve or in- crease lean body mass in patients with malnutrition and weight loss. Further research is needed to define clinical applications for giving anabolic hormones as a pharmacologic intervention
in combination with nutrition therapy in older individuals.
CONCLUSION
Malnutrition is common in older individuals, which ag- gravate a weakened immune system in older individuals. The physician should be aware of the high prevalence and the con- sequences of malnutrition. Early screening and assessment of nutritional status should be followed by providing appropriate nutritional supplementation to reverse the deterioration of health in malnourished older individuals.
REFERENCES
1. Allison SP. Malnutrition, disease, and outcome. Nutrition 2000;16(7-8):590-3.
2. Meijers JM, van Bokhorst-de van der Schueren MA, Schols JM, Soeters PB, Halfens RJ. Defining malnutrition: mission or mission impossible? Nutrition 2010;26(4):432-40.
3. Chin A Paw MJ, Dekker JM, Feskens EJ, Schouten EG, Kromhout D. How to select a frail elderly population? A com- parison of three working definitions. J Clin Epidemiol 1999;52(11):1015-21.
4. Morley JE, Silver AJ. Nutritional issues in nursing home care.
Ann Intern Med 1995;123(11):850-9.
5. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al; Cardiovascular Health Study Collaborative Research Group. Frailty in older adults: evidence for a phe- notype. J Gerontol A Biol Sci Med Sci 2001;56(3):M146-56.
6. Omran ML, Morley JE. Assessment of protein energy malnu- trition in older persons, Part II: Laboratory evaluation. Nutrition 2000;16(2):131-40.
7. MacIntosh C, Morley JE, Chapman IM. The anorexia of aging. Nutrition 2000;16(10):983-95.
8. Morley JE, Morley PMK. Psychological and social factors in the pathogenesis of weight loss. Ann Rev Gerontal Geriatr 1995;15(1):83-109.
9. Kyle UG, Unger P, Mensi N, Genton L, Pichard C. Nutrition status in patients younger and older than 60 y at hospital ad- mission: a controlled population study in 995 subjects. Nutri- tion 2002;18(6):463-9.
10. Sullivan DH. Undernutrition in older adults. Ann Long Term Care 2000;8:41-6.
11. Bienia R, Ratcliff S, Barbour GL, Kummer M. Malnutrition in the hospitalized geriatric patient. J Am Geriatr Soc 1982;
30(7):433-6.
12. Willard MD, Gilsdorf RB, Price RA. Protein-calorie malnu- trition in a community hospital. JAMA 1980;243(17):1720-2.
13. Mion LC, McDowell JA, Heaney LK. Nutritional assessment of the elderly in the ambulatory care setting. Nurse Pract Forum 1994;5(1):46-51.
14. Chung SH, Sohn CM. Nutritional status of hospitalized geri- atric patients using by the mini nutritional assessment. Korean J Community Nutr 2005;10(5):645-53.
15. Vasto S, Candore G, Balistreri CR, Caruso M, Colonna- Romano G, Grimaldi MP, et al. Inflammatory networks in ageing, age-related diseases and longevity. Mech Ageing Dev 2007;128(1):83-91.
16. Victor VM, De la Fuente M. N-acetylcysteine improves in vi- tro the function of macrophages from mice with endotoxin-in- duced oxidative stress. Free Radic Res 2002;36(1):33-45.
17. Bistrian BR, Blackburn GL, Scrimshaw NS, Flatt JP. Cellular immunity in semistarved states in hospitalized adults. Am J Clin Nutr 1975;28(10):1148-55.
18. Lesourd BM. Nutrition and immunity in the elderly: mod- ification of immune responses with nutritional treatments. Am J Clin Nutr 1997;66(2):478S-84S.
19. Beisel WR. Nutrition in pediatric HIV infection: setting the research agenda. Nutrition and immune function: overview. J Nutr 1996;126(10 Suppl):2611S-5S.
20. Schiffrin EJ, Blum S. Interactions between the microbiota and the intestinal mucosa. Eur J Clin Nutr 2002;56(Suppl 3):S60-4.
21. Chandra RK. Graying of the immune system. Can nutrient supplements improve immunity in the elderly? JAMA 1997;
277(17):1398-9.
22. Penn ND, Purkins L, Kelleher J, Heatley RV, Mascie-Taylor BH, Belfield PW. The effect of dietary supplementation with vitamins A, C and E on cell-mediated immune function in eld- erly long-stay patients: a randomized controlled trial. Age Ageing 1991;20(3):169-74.
23. Chandra RK. Effect of vitamin and trace-element supple- mentation on immune responses and infection in elderly subjects. Lancet 1992;340(8828):1124-7.
24. Ibs KH, Rink L. Zinc-altered immune function. J Nutr 2003;
133(5 Suppl 1):1452S-6S.
25. Haase H, Rink L. The immune system and the impact of zinc during aging. Immun Ageing 2009;(6):9.
26. Omran ML, Morley JE. Assessment of protein energy malnu- trition in older persons, part I: History, examination, body composition, and screening tools. Nutrition 2000;16(1):50-63.
27. Vellas B, Villars H, Abellan G, Soto ME, Rolland Y, Guigoz Y, et al. Overview of the MNA--Its history and challenges.
J Nutr Health Aging 2006;10(6):456-63.
28. Rubenstein LZ, Harker JO, Salvà A, Guigoz Y, Vellas B.
Screening for undernutrition in geriatric practice: developing the short-form mini-nutritional assessment (MNA-SF). J Gerontol A Biol Sci Med Sci 2001;56(6):M366-72.
29. Guigoz Y. The Mini Nutritional Assessment (MNA) review of the literature--What does it tell us? J Nutr Health Aging 2006;10(6):466-85.
30. Kaiser MJ, Bauer JM, Ramsch C, Uter W, Guigoz Y, Cederholm T, et al; MNA-International Group. Validation of the Mini Nutritional Assessment short-form (MNA-SF): a practical tool for identification of nutritional status. J Nutr Health Aging 2009;13(9):782-8.
31. Stratton RJ, Hackston A, Longmore D, Dixon R, Price S, Stroud M, et al. Malnutrition in hospital outpatients and in- patients: prevalence, concurrent validity and ease of use of the
‘malnutrition universal screening tool’ (‘MUST’) for adults.
Br J Nutr 2004;92(5):799-808.
32. Kondrup J, Rasmussen HH, Hamberg O, Stanga Z; Ad Hoc ESPEN Working Group. Nutritional risk screening (NRS 2002): a new method based on an analysis of controlled clin- ical trials. Clin Nutr 2003;22(3):321-36.
33. Delmi M, Rapin CH, Bengoa JM, Delmas PD, Vasey H, Bonjour JP. Dietary supplementation in elderly patients with fractured neck of the femur. Lancet 1990;335(8696):1013-6.
34. Lauque S, Arnaud-Battandier F, Mansourian R, Guigoz Y, Paintin M, Nourhashemi F, et al. Protein-energy oral supple- mentation in malnourished nursing-home residents. A con-
trolled trial. Age Ageing 2000;29(1):51-6.
35. Norman K, Kirchner H, Freudenreich M, Ockenga J, Lochs H, Pirlich M. Three month intervention with protein and en- ergy rich supplements improve muscle function and quality of life in malnourished patients with non-neoplastic gastro- intestinal disease--a randomized controlled trial. Clin Nutr 2008;27(1):48-56.
36. Wilson MM, Purushothaman R, Morley JE. Effect of liquid dietary supplements on energy intake in the elderly. Am J Clin Nutr 2002;75(5):944-7.
37. Gersovitz M, Motil K, Munro HN, Scrimshaw NS, Young VR. Human protein requirements: assessment of the adequacy of the current Recommended Dietary Allowance for dietary protein in elderly men and women. Am J Clin Nutr 1982;
35(1):6-14.