Korean Circulation Journal
Introduction
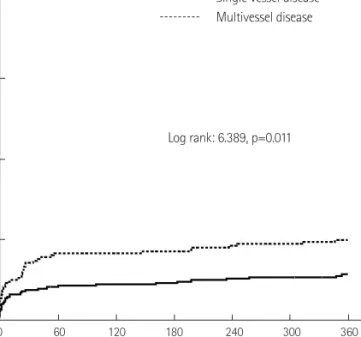
The incidence of multivessel disease (MVD) in patients with acute myocardial infarction (AMI) is reported to be 40-50%. The morbid- ity and mortality are higher in patients with MVD versus single ves- sel disease (SVD).
1-6)Chronic total occlusion (CTO) is commonly fo-
Print ISSN 1738-5520 • On-line ISSN 1738-5555
Impact of Multivessel Coronary Disease With Chronic Total Occlusion on One-Year Mortality in Patients With Acute Myocardial Infarction
Ju Hwan Lee, MD 1,2 , Hun Sik Park, MD 1 , Hyeon Min Ryu, MD 2 , Hyunsang Lee, MD 2 , Myung Hwan Bae, MD 1 , Jang Hoon Lee, MD 1 , Dong Heon Yang, MD 1 , Yongkeun Cho, MD 1 , Shung Chull Chae, MD 1 , and Jae-Eun Jun, MD 1
1
Department of Internal Medicine, Kyungpook National University School of Medicine, Daegu,
2