122 CASE REPORT
Korean Circ J 2008;38:122-127
Print ISSN 1738-5520 / On-line ISSN 1738-5555 Copyright ⓒ 2008 The Korean Society of Cardiology
A Case Report of Recurrent Subacute Stent Thrombosis After Repetitive Percutaneous Coronary Interventions
Myung Soo Kang, MD, Ki Ju Jeung, MD, Ji Hyeong Kim, MD, Hye-Sun Seo, MD, Duk Won Bang, MD, Yoon Haeng Cho, MD, Nae Hee Lee, MD, Min Su Hyon, MD, Sung Koo Kim, MD and Young Joo Kwan, MD Division of Cardiology, Department of Internal Medicine, Soonchunhyang University College of Medicine, Bucheon, Korea ABSTRACT
Stent thrombosis (ST) is one of the major complications that occur in percutaneous coronary interventions (PCIs) with stents. Various factors have been attributed to the development of ST, and several strategies have been recommended for its management. We report the case of a patient suffering from recurrent subacute STs after recurrent PCIs. The patient was treated by coronary artery bypass graft (CABG). (Korean Circ J 2008;38:122-127) KEY WORDS: Stents; Thrombosis.
Introduction
Percutaneous coronary intervention (PCI) with stents is the most popular method for treating coronary artery disease (CAD). However, stent thrombosis (ST), one of the major complications in PCIs with stents, is highly lethal, and several methods for treating STs have been suggested. We report the case of a patient suffering from recurrent subacute STs after recurrent PCIs.
Case
A 50-year-old woman presented with syncope and chest tightness that had occurred 4 hours ago. She had no history of hypertension, diabetes mellitus, and chron- ic renal failure. Further, she did not taking any drugs that could deteriorate the platelet function. Her blood pressure was 140/80 mmHg, and her pulse rate was 80 beats per minute. Electrocardiography (ECG) re- vealed a third degree atrioventricular block (Fig. 1).
Her plasma creatinine kinase, CK-myocardial band iso- enzyme, and Troponin T levels were 143 IU/L, 6.5 ng/
mL, and 0.31 ng/mL, respectively. On admission, she received 300 mg aspirin and 600 mg clopidogrel; sub- sequently, she continued to receive aspirin and 100 mg/
day clopidogrel. Two days after admission, coronary
angiography (CAG) revealed the culprit lesion of the subtotally occluded proximal portion of the left anterior descending artery (LAD) with thrombolysis in myocar- dial infarction (TIMI) grade 3 flow [quantitative coro- nary analysis (QCA), diameter stenosis (DS); 71.5%] and 70% stenosis (QCA, 78.73%) in the middle segment of the right coronary artery (RCA) (Fig. 2). Two Cypher® stents (2.5/23 mm and 3.0/28 mm; Cordis/Johnson &
Johnson, USA) were implanted in each lesion (Fig. 3) at 16 and 18 mmHg (post-PCI QCA: RCA, 8.3%;
LAD, 6.5%), respectively, and cilostazole was applied.
Two days after the PCI, the patient complained of chest pain. ECG revealed ST segment elevation in leads V2- V4 (Fig. 4). The second angiography revealed total oc- clusion in the previous stent-implanted area of the LAD (Fig. 5A), and PCI using a Quantum® balloon (3.0/12 mm; Boston Scientific, USA) at 16 mmHg was performed successfully with ReoPro(abciximab) infu- sion (Fig. 5B). Platelet function analysis (Platelet Aggre- gometer, ChronoLog Corporation, USA) showed that the transillumination rates of collagen (C), adenosine diphos-phate (ADP), and arachidonic acid (AA) were below the normal values (C 10%, control value 80%;
ADP 5 μM:20 μM 16%:19%, control value 43%:74%;
AA 22%, control value 71%); this finding was inter- preted as a normal response to aspirin and clopidogrel.
The levels of protein C, protein S, factor assay, and lupus anticoagulant antibody were also within the normal range. Chest pain recurred 5 days after the first ST event.
The third CAG showed total occlusion of the proximal LAD (Fig. 6A). PCI using a Cypher® stent (2.5/33 mm; Cordis/Johnson&Johnson) at 18 mmHg was form- ed successfully (Fig. 6B). Two days after the second ST
Received: June 4, 2007
Revision Received: August 16, 2007 Accepted: August 31, 2007
Correspondence: Yoon Haeng Cho, MD,Division of Cardiology, Department of Internal Medicine, Soonchunhyang University College of Medicine, 1174 Jung-dong, Wonmi-gu, Bucheon 420-767, Korea
Tel: 82-32-621-5132, Fax: 82-32-621-5016 E-mail: [email protected]
Myung Soo Kang, et al.·123
episode, the patient complained of neck pain. ECG revealed ST segment elevation in leads V2-V6 (Fig. 7).
However, emergency rescue PCI could not be performed at that time. Therefore, thrombolytic therapy with tissue plasminogen activator (t-PA) was performed successfully, and the fourth CAG showed no residual stenosis or thrombosis. However, right-side weakness, dysarthria, and disorientation occurred on the next day. Her brain CT scan revealed intracranial hemorrhage (ICH) in the
thalamus near the left third ventricle. Despite this find- ing, we decided to continue administration of aspirin and clopidogrel to prevent additional ST episodes. After 4 days, her mental status improved but chest pain re- curred. ECG revealed ST elevation in leads II, III, and aVF (Fig. 8). The fifth CAG showed total occlusion in the earlier stent-implanted lesion of the RCA (Fig. 9A).
Emergency PCI using a Kongou® balloon (3.5/15 mm;
Terumo Corp., Japan) at 16 mmHg was performed suc-
Fig. 1. ECG showed third degree atrioventricular block (data obtained from another hospital). ECG: electrocardiography.
I
II
III
aVR
aVL
aVF
V1
V2 ½
V3 ½
V4
V5
V6
Fig. 2. Initial finding of coronary angiogram. CAG showed the culprit lesion (dark arrow) of the subtotally occluded proximal portion of the LAD with TIMI grade 3 flow (A) and 70% stenosis (dotted arrow) in the middle segment of the RCA (B). CAG: coronary angiography, LAD: left anterior descending artery, TIMI: thrombolysis in myocardial infarction, RCA: right coronary artery.
A B
124·Recurrent Stent Thrombosis Treated With CABG
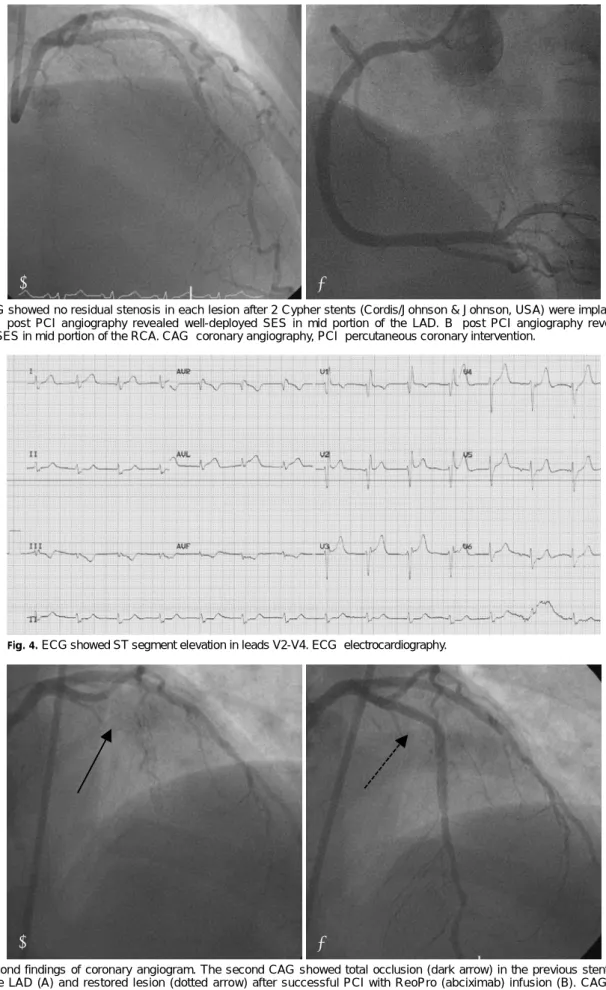
Fig. 3. CAG showed no residual stenosis in each lesion after 2 Cypher stents (Cordis/Johnson & Johnson, USA) were implanted in the lesions. A: post PCI angiography revealed well-deployed SES in mid portion of the LAD. B: post PCI angiography revealed well- deployed SES in mid portion of the RCA. CAG: coronary angiography, PCI: percutaneous coronary intervention.
B A
Fig. 4. ECG showed ST segment elevation in leads V2-V4. ECG: electrocardiography.
Fig. 5. Second findings of coronary angiogram. The second CAG showed total occlusion (dark arrow) in the previous stent-implanted area of the LAD (A) and restored lesion (dotted arrow) after successful PCI with ReoPro (abciximab) infusion (B). CAG: coronary angiography, LAD: left anterior descending artery, PCI: percutaneous coronary intervention.
B A
Myung Soo Kang, et al.·125
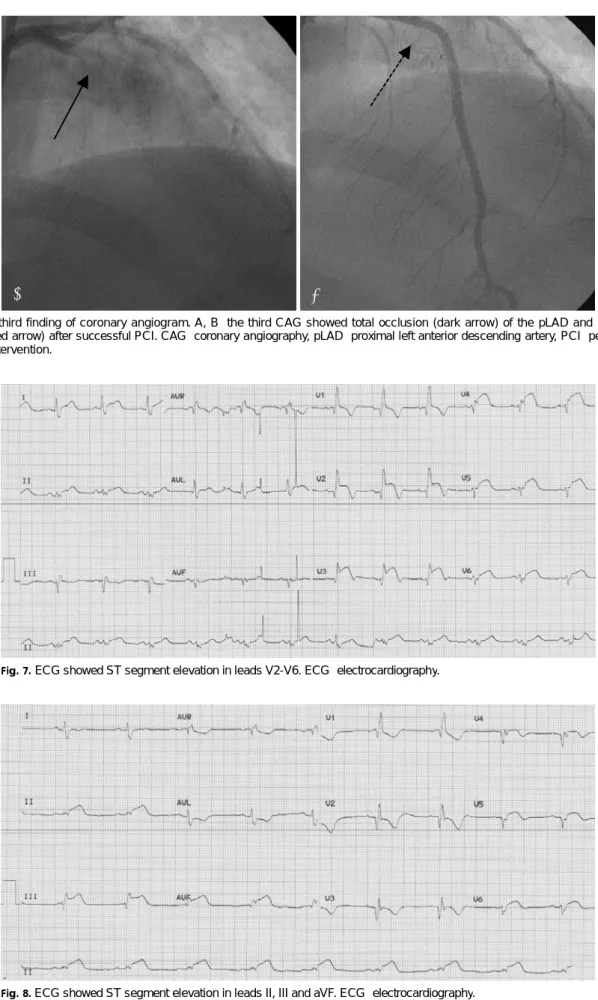
Fig. 6. The third finding of coronary angiogram. A, B: the third CAG showed total occlusion (dark arrow) of the pLAD and recanalized lesion (dotted arrow) after successful PCI. CAG: coronary angiography, pLAD: proximal left anterior descending artery, PCI: percutaneous coronary intervention.
A B
Fig. 7. ECG showed ST segment elevation in leads V2-V6. ECG: electrocardiography.
Fig. 8. ECG showed ST segment elevation in leads II, III and aVF. ECG: electrocardiography.
126·Recurrent Stent Thrombosis Treated With CABG
cessfully (Fig. 9B). Chest pain recurred 10 h after the PCI. Since CAG revealed a lesion in the RCA again (Fig. 10), we decided to perform coronary artery bypass graft (CABG). A few days after the emergency CABG, the patient recovered and was discharged without any complications. Thus far, the patient has shown good progress at follow-ups.
Discussion
Although the efficacy and safety of drug-eluting co- ronary stents (DESs) are well known, there are many
concerns regarding ST after DES deployment. ST may occur acutely, subacutely (<30 days), lately (<1 year), or very lately (>1 year) and may result in serious com- plications associated with myocardial infarction (MI) and death.
In recent studies on ST, the rate of ST after DESs implantation was 1.2-1.8%; furthermore, it remains con- troversial whether DESs are more thrombogenic than bare metal stents (BMSs).1-4) According to a domestic re- search, the rate of ST after successful DES implantation was 1.8%, and except for 1 patient, ST occurred within 7 days in all patients.5) In our patient, ST occurred 5 times in multiple lesions (proximal LAD and middle RCA). To the best of our knowledge, this is the first study to report the occurrence of ST for more than 5 times in a patient without aspirin and clopidogrel re- sistance and blood abnormalities. Whenever STs oc- curred, emergency PCIs were performed. Finally, CABG was performed for ST management. It is known that most cases of ST are related to premature discontinua- tion of the antiplatelet therapy.5)6) Although dual anti- platelet therapy effectively attenuates ST, long and mul- tiple stents,7)8) stent underexpansion,9) stent malapposi- tion,9)10) residual dissection,7) impaired response to as- pirin and clopidogrel, and platelet polymorphism11-13) may also affect ST. Our patient was daily administered with the dual antiplatelet therapy, and her platelet function analysis revealed a normal response to aspirin and clopidogrel, as mentioned earlier. Since we did not perform intravascular ultrasound (IVUS) of the coronary arteries, we were unable to determine the factors as- sociated with ST, including stent malapposition. In conclusion, recurrent STs appear to occur by multiple causes. Emergency CABG is an effective method for managing recurrent STs.
Fig. 9. The fifth finding of coronary angiogram. A, B: the fifth CAG showed total occlusion (dark arrow) in the earlier stent-implanted lesion of the RCA and recanalized lesion (dotted arrow) after successful PCI. CAG: coronary angiography, RCA: right coronary artery, PCI: percutaneous coronary intervention.
A B
Fig. 10. The sixth CAG revealed exactly the same lesion (dark arrow) in the RCA 10 h after the PCI. CAG: coronary angiography, RCA: right coronary artery, PCI: percutaneous coronary inter- vention.
Myung Soo Kang, et al.·127
Limitation
Since IVUS was not performed, the lesions could not be precisely observed, and the cause of multiple episodes of ST could not be determined.
REFERENCES
1) Kuchulakanti PK, Chu WW, Torguson R, et al. Correlates and long-term outcomes of angiographically proven stent thrombosis with sirolimus- and paclitaxel-eluting stents. Circulation 2006;
113:1108-13.
2) Park DW, Park SW, Lee SW, et al. Frequency of coronary arte- rial late angiographic stent thrombosis (LAST) in the first six months: outcomes with drug-eluting stents versus bare metal stents. Am J Cardiol 2007;99:774-8.
3) Mauri L, Hsieh WH, Massaro JM, Ho KK, D’Agostino R, Cutlip DE. Stent thombosis in randomized clinical trials of drung-eluting stents. N Engl J Med 2007;356:1020-9.
4) Stone GW, Moses JW, Ellis SG, et al. Safety and efficacy of siro- limus- and paclitaxel-eluting coronary stents. N Engl J Med 2007;
356:998-1008.
5) Park SH, Hong GR, Seo HS, Tahk SJ. Stent thrombosis after successful drug-eluting stent implantation. Korean Circ J 2005;
35:163-71.
6) Iakovou I, Schmidt T, Bonizzouni E, et al. Incidence, predictors,
and outcome of thrombosis after successful implantation of drug eluting stents. JAMA 2005;293:2126-30.
7) Orford JL, Lennon R, Melby S, et al. Frequency and correlates of coronary stent thrombosis in the modern era: analysis of a single center registry. J Am Coll Cardiol 2002;40:1567-72.
8) Cutlip DE, Baim DS, Kalon K, et al. Stent thrombosis in the modern era. Circulation 2001;103:1967-71.
9) Uren NG, Schwarzacher SP, Metz JA, et al. Predictors and out- comes of stent thrombosis: an intravascular ultrasound registry.
Eur Heart J 2002;23:124-32.
10) Choi BR, Lee CW, Park SW. Late stent thrombosis associated with late stent malapposition after drug-eluting stenting: a case report. Korean Circ J 2006;36:472-5.
11) Sucker C, Scheffold N, Cyran J, Ghodsizad A, Scharf RE, Zotz RB. No evidence for involvement of prothrombotic platelet re- ceptor polymorphisms in acute coronary stent thrombosis. Int J Cardiol 2007; [Epub ahead of print].
12) Glowczynska R, Malek LA, Spiewak M, et al. Clinical, bioche- mical and genetical resistance to clopidogrel in a patient with the recurrent coronary stent thrombosis: a case report and review of the literature. Int J Cardiol 2006;111:326-8.
13) Wenaweser P, Dorffler-Melly J, Imboden K, et al. Stent thrombosis is associated with an impared response to antiplatelet therapy. J Am Coll Cardiol 2005;45:1748-52.