Received: April 24, 2013, Revised: June 5, 2013, Accepted: June 6, 2013 ISSN 1598-4478 (Print) / ISSN 2233-7679 (Online)
†Correspondence to: Ki Seok Hong
Department of Periodontology, Dankook University School of Dentistry, 119, Dandae-ro, Dongnam-gu, Cheonan 330-714, Korea Tel: +82-41-550-1987, Fax: +82-41-555-0222, E-mail: [email protected]
*Hae-Su Jung and Hyun-Sook Bae contributed equally to this work.
Copyright © 2013 by the Korean Society of Dental Hygiene Science
The Effects of Platelet-Rich Fibrin on Osteoblast Proliferation and Differentiation: Effects of
Platelet-Rich Fibrin on Osteoblasts
Hae-Su Jung*, Hyun-Sook Bae
1* and Ki Seok Hong
†Department of Periodontology, Dankook University School of Dentistry, Cheonan 330-714, 1Department of Dental Hygiene, Namseoul University, Cheonan 331-307, Korea
혈소판 농축 섬유소가 골모세포 증식과 분화에 미치는 영향
정해수*ㆍ배현숙1*ㆍ홍기석†
단국대학교 치과대학 치주과학교실, 1남서울대학교 치위생학과
The most frequently encountered problems at fixture-implantation sites are lack of adequate bone and proximity to anatomic structures. It is generally accepted that growth factors play an essential role in the healing process and tissue formation, and they have become the focus of grafting materials research. The granules in platelets contain high concentrations of various growth factors. In particular, platelet-rich fibrin (PRF) is a second-generation platelet concentrate that allows the production of fibrin membranes enriched with platelets and growth factors from an anticoagulant-free blood harvest. This study investigated the in vitro effects of PRF on osteoblasts, in terms of the key cellular functions, and especially the effects on two growth factors, the homodimer of platelet-derived growth factor subunit B (BPDGF-BB) and transforming growth factor (TGF)-βββ1, which are associated with wound healing and regeneration (i.e., proliferation and differentiation). The following parameters were investigated: PDGF-BB and TGF-β1 levels in PRF, cell viability, alkaline phosphatase (ALP) activity, type 1 collagen synthesis, and the expressions of osteoblast differentiation markers (ALP and runt-related transcription factor 2) and bone matrix proteins (type 1 collagen). The release of autologous growth factors from PRF was maintained for a reasonable period of time, and exerted positive effects on the proliferation and differentiation of osteoblasts. The use of PRF thus appears to be a promising method for enhancing bone healing and remodeling.
Key Words: Blood platelet, Cell differentiation, Cell proliferation, Osteoblast
Introduction
Studies of platelet-rich plasma (PRP), the first practical factor in tissue engineering, have produced a respectable database of research findings and clinical outcomes in various settings1). PRP, which is a concentrated source of autologous platelets, contains and releases (through degra- nulation) at least seven different growth factors (cyto-
kines) that stimulate bone and soft-tissue healing. PRP is obtained by collecting blood from the patient and cen- trifuging it at varying speeds until it separates into three layers: platelet poor plasma (PPP), PRP, and red blood cells (RBCs). This usually requires two spins: the first (hard) spin separates the PPP from the red fraction and PRP, while the second (soft) spin separates the red fraction from the PRP. The material with the highest specific
gravity (i.e., PRP) is deposited at the bottom of the tube.
Immediately prior to its application, a platelet activa- tor/agonist (topical bovine thrombin and 10% calcium chloride) is added to activate the clotting cascade, pro- ducing a platelet gel. The whole process takes appro- ximately 12minutes and produces a platelet concentration that is 35 times that of native plasma. The clinical applications of PRP in dentistry include cosmetic peri- odontal surgery, esthetic dental implant reconstruction, and the immediate restoration of dental implants. Pio- neering use of PRP in dentistry includes the work of Marx and Garg2).
There are numerous reports of the favorable effects of PRP on wound healing after bone augmentation. How- ever, some of those studies did not control the quan- tification of platelet yield in both whole blood and PRP, use commercial assays to quantify growth factor con- centration (e.g., PRP may or may not also contain increa- sed concentrations of white blood cells), use contralateral control groups, and performed histomorphometric analysis of the specimens3). Furthermore, the safety of PRP re- mains an issue. As reported by Sánchez et al.4), who ela- borated on the potential risks associated with the use of PRP, the process of accelerating PRP gel formation using calcium chloride and bovine thrombin may be associated with the development of antibodies to factors V and XI, and thrombin, thus increasing the risk of life-threatening coagulopathies. It has also been shown that preparations of thrombin containing factor V could stimulate the immune system when challenged with a foreign protein5).
In contrast, platelet-rich fibrin (PRF) is a second- generation platelet concentrate that allows the production of fibrin membranes enriched with platelets and growth factors from an anticoagulant-free blood harvest6). By definition, fibrin is the activated form of a plasmatic mole- cule called fibrinogen. This soluble fibrillary molecule is abundant in both plasma and the platelet -granules, and plays a determining role in platelet aggregation during hemostasis. It is transformed into a kind of biologic glue that is capable of consolidating the initial platelet cluster, thus constituting a protective wall along vascular breaches during coagulation. Fibrinogen is actually the final sub- strate of all coagulation reactions. Being a soluble protein,
fibrinogen is transformed into an insoluble fibrin by th- rombin, and the polymerized fibrin gel constitutes the first cicatricial matrix of the injured site.
The PRF protocol was described for the first time in 2001 by Dohan et al.7). It is a general protocol involving a simplified technique that is not linked to either a medical device or a specific machine, and is free and openly acce- ssible to all clinicians. The required quantity of blood is drawn into 10-ml test tubes without an anticoagulant and is immediately centrifuged using a tabletop centrifuge for 12 minutes at 2,700 r/min. The resultant product compri- ses three layers: PPP, PRF, and RBCs. PRF is not a blood- derived product, in contrast to the PRPs and fibrin glues.
The production of PRF does not require modification of the blood composition using, for example, bovine throm- bin, anticoagulants, or calcium chloride. PRF is polyme- rized according to a completely natural process without any modifiers. Therefore, it is a totally autologous mate- rial that is prepared extemporaneously, in the same way as a bone harvest (chin, retromandibular line, iliac, or parie- tal) or a palatal connective tissue harvest.
Researches into clinical applications of PRF have yield- ed very promising results. However, there have been insu- fficient basic studies to support its efficacy. The aim of this study was therefore to determine the in vitro effects of PRF on osteoblasts, in terms of the key cellular functions, and especially on the release of two growth factors, the homodimer of platelet-derived growth factor (PDGF) subunit B (PDGF-BB) and transforming growth factor (TGF-) type 1 (TGF-1), which are associated with wound healing and regeneration (i.e., proliferation and differen- tiation).
Materials and Methods
1. Reagents
α−Minimum essential medium (α−MEM), Dulbecco's modi- fied Eagle's medium (DMEM), and fetal bovine serum (FBS) were purchased from Invitrogen (Carlsbad, CA, USA). Except where stated otherwise, all other reagents were obtained from Sigma-Aldrich (St. Louis, MO, USA).
2. Collection and preparation of platelet-rich fibrin Blood was collected from a 27-year-old male volunteer at the Department of Periodontology, Dankook Dental Hospital, Korea. The volunteer received clear and honest information regarding the nature and the objectives of our study before testing. The 10 ml blood sample was collec- ted without anticoagulant into a 10 ml glass-coated plastic tube and immediately centrifuged using a tabletop centri- fuge (Medifuge, Silfradent, Italy). After centrifugation the PRF clot was apparent in the middle of the tube between a jelly-like RBC layer at the bottom and a supernatant of serum at the top. The PRF clots were retrieved from the tube and the RBC gel was detached and discarded. The upper layer, comprising PPP, was also taken and used as a control factor.
The PRF was incubated with 10 ml of fresh α−MEM at 37oC under 5% CO2 in air. Samples of exudate were colle- cted on days 1, 7, 14, and 21 and stored at 80C before use.
These α−MEM-enriched exudate samples represent 100%
exudate, while experiments were performed using 20%
exudate solutions (diluted with α−MEM).
3. Cell culture
The MC3T3-E1 cells and MG63 cells, derived from mouse calvaria and human osteosarcoma, respectively, were used in this study. These cell lines were maintained with α−MEM or DMEM containing 10% FBS. All of the cells were cultured in 10 mm culture dishes at 37oC under 5% CO2 in air.
4. Measurements of transforming growth factor type 1 and platelet-derived growth factor subunit B levels in platelet-rich fibrin
The TGF-1 and PDGF-BB levels in the supernatant of activated PRF were determined using a commercially available sandwich enzyme-linked immunosorbent assay (ELISA) kit from R&D Systems (Quantikine, R&D Sys- tems, Minneapolis, MN, USA) according to the manu- facturer's instructions. All assays were performed in du- plicate.
5. Cell viability
Cell viability was determined using the 3-(4, 5-dime-
thylthiazol-2-yl)-2, 5-diphenyltetrazolium bromide (MTT) assay. MC3T3-E1 cells were seeded at 8×103 cells/well into 96-well plates. The cells were treated with 20% PRF.
After culture, the cells were incubated with 20 μl of MTT (5 mg/ml; added to each well) for another 34 hours at 37oC under 5% CO2 in air. The supernatants were discarded, and 100 μl of isopropyl alcohol was added to each well to dissolve the formazan crystals produced. The optical density of formazan was measured at 540 nm by spec- trophotometry. The mean values of triplicate experiments were determined.
6. Measurement of alkaline phosphatase activity The MC3T3-E1 cells were seeded on 96-well plates in α−MEM with 10% FBS. The cells were treated with 20%
PRF-supplemented 2% FBS for 72 hours. After lysing in 0.05% Triton X-100 buffer, the cell lysates were analyzed for alkaline phosphatase (ALP) activity. The enzyme activity was measured at 405 nm by spectrophotometry using p-nitrophenylphosphate (100 mM) as a substrate.
ALP activity was determined using a p-nitrophenol stan- dard curve and normalized to total cellular protein.
7. Measurement of type I collagen synthesis
The MG63 cells were seeded onto six-well plates in DMEM with 10% FBS. The cells were treated with 20%
PRF-supplemented 2% FBS for 24 hours. After lysing in 100 μl of PBS with 0.5% Triton X-100, 1 mM EDTA, and 1 mM phenylmethylsulfonyl fluoride, cell lysates were analyzed for type I collagen production. The amount of type I collagen was determined using commercially avail- able sandwich ELISA kits (Takara Bio, Otsu, Shiga, Japan) according to the manufacturer's instructions. All type I collagen assays were performed in duplicate.
8. Statistical analysis
Mean values and standard deviations were calculated.
Differences between the control (PPP) and test groups (PRF) over time were compared using Student's t-test.
The probability cutoff for statistical significance was set at p<0.05.
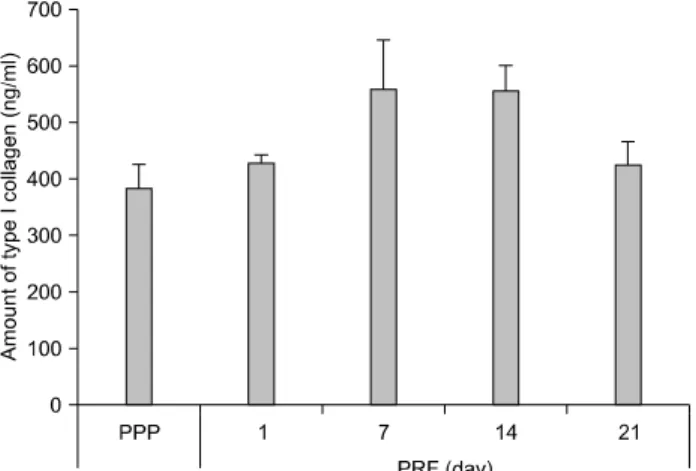
Fig. 4. Amount of type I collagen. The amount of type I collagen produced by cells treated with exudates of PRF collected on days 1, 7, 14, and 21 did not differ significantly. However, the amounts produced by cells treated with PRF exudate collected on days 7 and 14 were higher than those of cells treated with PPP. PRF:
platelet-rich fibrin, PPP: platelet poor plasma.
Fig. 1. TGF-1 and PDGF-BB levels. PRF TGF-1 levels at days 1 and 7 were significantly higher than those of PPP. PRF PDGF-BB levels at days 1, 7, 14, and 21 were significantly higher than those of PPP. However, PDGF-BB levels at days 7, 14, and 21 did not differ significantly from those at day 1. TGF-1: trans- forming growth factor type 1, PDGF-BB: platelet-derived growth factor subunit B, PRF: platelet-rich fibrin, PPP: platelet poor plasma.
Fig. 2. Osteoblast viability. There was a significant increase in osteoblast proliferation when the culture medium contained exu- dates of PRF collected on days 7, 14, and 21 compared to culture medium containing PPP (**p<0.01 compared to PPP). PRF: pla- telet-rich fibrin, PPP: platelet poor plasma.
Fig. 3. ALP activity. The ALP activity of osteoblasts treated with exudates of PRF collected on days 7 and 14 was significantly higher than that of osteoblasts treated with PPP. However, the ALP activity of osteoblasts was reduced when treated with PRF collected on day 21 (*p<0.05 compared to PPP). ALP: alkaline phosphatase, PRF: platelet-rich fibrin, PPP: platelet poor plasma.
Results
1. Measurements of transforming growth factor type 1 and platelet-derived growth factor subunit B levels Levels of TGF-1 in PRF harvested at days 1 and 7 were significantly higher than those found in PPP. At day 1, PRF released a maximum level of TGF-1, which was maintained to day 7 (no significant difference). The levels of PDGF-BB in PRF on days 1, 7, 14, and 21 were
significantly higher than those in PPP. The maximum amount of PDGF-BB was released on day 1, which was maintained up to day 21 (no significant difference; Fig. 1).
2. Cell viability
MTT assay was used to determine the effects of PRF on osteoblast viability. There was a significant increase in the proliferation of osteoblasts when the culture medium contained exudates of PRF harvested on days 7, 14, and 21 compared to the culture medium containing PPP (Fig. 2).
3. ALP activity
The ALP activity was measured to observe the effects on osteoblast differentiation over 72 hours. The ALP activity of cells treated with exudates of PRF collected at days 7 and 14 were significantly higher than those of PPP (Fig. 3).
4. Measurement of type I collagen synthesis
The synthesis of type I collagen by osteoblasts was detected using ELISA. The amounts of type I collagen synthesized by osteoblasts treated with exudates of PRF collected at days 7 and 14 were higher than that of osteoblasts treated with PPP (Fig. 4).
Discussion
The granules in platelets contain high concentrations of various growth factors. Growth factors PDGF and TGF- are both important in the process of connective tissue repair and bone regeneration, triggering adjacent cells (e.g., preosteoblasts), and inducing their differentiation into mature osteoblasts favoring the initiation of bone remodeling, tissue healing, and bone mineralization8,9). In particular, PDGF-BB exerts strong mitogenic effects on stem cells and osteoblasts, and promotes angiogenesis and collagen synthesis, thus enhancing the process of wound healing, while TGF-1 is the most abundant TGF- isoform detected in bone and is an important functional modulator of osteoclasts. TGF-1 can induce osteoclast apoptosis.
PDGF and TGF- have been identified in PRF. It is hypothesized that these soluble molecules are trapped in the fibrin mesh of PRF and can be released in a con- trollable, and relatively long-term way. Su et al.10) found that the content of PDGF-AB and TGF-1 in PRF releasate increased over time. However, these reports are not consistent with that of Gassling et al.11), who examined the growth factor release from PRF and reported that PRF did not contain either TGF-1 or PDGF-BB. A possible explan- ation for the different cytokine contents of these PRFs could be the lack of standardization of the PRF preparation procedure, as has been reported for PRP.
The present study found that high levels of released PDGF-BB in activated PRF were maintained from day 1
to day 21 (the slight decrease from day 7 onward was not statistically significant). Meanwhile, levels of TGF-1 released from activated PRF were highest at day 1, decreasing slightly to day 7, and then rapidly thereafter (Fig. 1). Statistical analysis of the levels of TGF-1 and PDGF-BB released from PRF at different time points confirmed the hypothesis proposed by Dohan and Choukroun12), which states that PRF slowly releases large amounts of growth factors for at least 7days. He et al.13) also showed that the growth factors PDGF and TGF reach peak levels at day 14.
Our finding indicated that PRF continued to release PDGF-BB and TGF-1 up to day 14. This is very important because it has been reported that bone graft healing is a sequential process involving inflammation, revasculari- zation, osteogenesis, remodeling, and incorporation into the host skeleton to form a mechanically efficient struc- ture, and the ingrowth and proliferation and differentiation of osteoblasts occurs during the initial 14 days of this process14,15). It therefore appears that PRF could enhance bone regeneration and as such be useful in clinical applications.
In terms of osteoblastic proliferation, the results obta- ined with PRF herein are very similar to those of previous studies13). In particular, we noted a growth peak for osteo- blasts at day 14 (Fig. 2). This finding is consistent with that of He et al.13), who showed a statistically significant increase in the proliferation of osteoblasts when the culture medium contained exudates of PRF collected at 14 days.
In comparison to the observation of osteoblastic proli- feration by PRP, several studies have demonstrated an absence of stimulation of proliferation by osteoblasts cultured with PRP; indeed, a negative effect on their proli- feration has even been observed16,17). Platelet concentrates contain a large number of different factors that exert highly variable effects. For example, the platelet granules contain equivalent ratios of angiostimulating factors (e.g., vascular endothelial growth factor and basic fibroblast growth factor) and angiostatic factors (e.g., endostatin and thrombospondin-1), which implies quite contrasting results18). In the same way, the effects of two key platelet cytokines, TGF-1 and PDGF-BB, vary according to the initial state of cells, with TGF-1 acting on differentiation
and PDGF-BB acting on proliferation19,20). Other research on PRP has generally demonstrated that while there is a significant stimulation of osteoblast proliferation by the PRP-type platelet concentrates, the reported effects never reach the level of intensity that Ehrenfest et al.observed in their study with PRF21-23).
ALP activity can usually be considered to reflect osteo- blast activity. Therefore, ALP activity was measured to study the effect of PRF on osteoblastic differentiation over a 72-hour period in the present study. The addition of PRF to the proliferating cultures seemed to stimulate simul- taneously the proliferation and a type of differentiation characterized by strong ALP activity. As shown in Fig. 3, the ALP activity of the cells treated with exudates of PRF increased significantly from day 1 to day 14 (p<0.05).
The ALP activity decreased from day 14 to day 21, but it was still slightly higher for the cells treated with exudates of PRF than for those treated with PPP. This finding of the present study is similar to those of other studies13), in which it was concluded that ALP activity was significantly higher during osteoblastic proliferation than in nonprolife- rating osteoblasts.
The present study found that PRF increased type 1 collagen as a bone matrix protein in the osteoblastic MG63 cells to a peak level at day 7, and that this high level was maintained until day 14 (Fig. 4). According to published data, PDGF stimulates type 1 collagen synthesis in fibro- blasts and up-regulates integrin 1, which enhances the mi- gratory response of fibroblasts to type 1 collagen and to several other extracellular matrix proteins24). Likewise, TGF- also activates fibroblasts to produce collagen.
Together these results indicate that it is likely that some growth factors in PRF could also stimulate collagen synthesis in MG63 cells. Centrella et al.25) reported that type 1 collagen synthesis in osteoblasts increases with the use of TGF-1.
Summary
Based on the data obtained in this study, we conclude that PRF induces the maintained release of autologous growth factors over a period of time that would be reasonable for clinical application, and that these released
growth factors exert positive effects on the proliferation and differentiation of osteoblasts in vitro, as characterized by cell viability, ALP activity, and type 1 collagen synthesis. Therefore, the use of PRF may be a promising method of enhancing bone healing and remodeling.
요 약
임플란트 식립 시 가장 빈번하게 맞게 되는 문제점으로 임플란트 식립 부위에서의 불충분한 골량과 해부학적 구조 에 의한 접근성의 문제를 들 수 있다. 일반적으로 성장 인자 들은 치유 과정이나 조직 형성에 있어서 가장 기본적인 필 수 요소로 인정되고 있다. 이러한 이유로 골 이식 재료의 효 과를 증진시키기 위한 성장 인자들이 최근에 주목을 받고 있다. 혈소판 내 granules에는 높은 농도의 다양한 성장 인 자들이 포함되어 있다. 특히, platelet-rich fibrin (PRF)는 2 세대 혈소판 농축 인자로 항응고제가 들어있지 않은 상태로 얻을 수가 있고, 혈소판과 많은 성장 인자들이 풍부한 섬유 소 막을 포함하고 있다. 이번 연구의 목적은 in vitro 상에서 골아 세포에 대한 PRF의 영향을 알아보고자 하였다. 특히 치유와 재생에 연관된 주요 기능으로써 증식과 분화에 대한 영향을 조사하고자 하였다. 이를 위해서, PRF 내에서 방출 되는 성장 인자(platelet-derived growth factor subunit B와 transforming growth factor-β1)의 농도, 세포의 생존능력, alkaline phosphatase (ALP) activity, type 1 collagen 합성, 골아 세포의 분화 지표로써 ALP와 Runx2의 발현 정도와 골 기질 단백질로써 type 1 collagen의 발현 정도에 대해서 조사하였다. 이 실험을 통하여 PRF는 치유 시 필요한 타당 한 기간 동안에 충분히 자가 성장 인자의 방출을 유지하고 있음을 알 수 있었고, 골아 세포의 증식과 분화에 대해서 긍 정적인 효과가 있음을 보여 주였다. 제한적인 실험이지만, 골재생을 위한 PRF의 사용은 골 치유와 골 개조에 있어서 증진 효과를 가져다줄 수 있는 촉망되는 방법 중 하나가 될 수 있을 것이다.
References
1. Gonshor A: Technique for producing platelet-rich plasma and platelet concentrate: background and process. Int J Periodo- ntics Restorative Dent 22: 547-557, 2002.
2. Marx RE, Garg AK. The sinus bone graft. Quintessence, Illinois, USA. pp. 183-189, 1999.
3. Wang HL, Avila G: Platelet rich plasma: myth or reality? Eur
J Dent 1: 192-194, 2007.
4. Sánchez AR, Sheridan PJ, Kupp LI: Is platelet-rich plasma the perfect enhancement factor? A current review. Int J Oral Maxillofac Implants 18: 93-103, 2003.
5. Landesberg R, Moses M, Karpatkin M: Risks of using platelet rich plasma gel. J Oral Maxillofac Surg 56: 1116- 1117, 1998.
6. Choukroun J, Adda F, Schoeffler C, Vervelle A: Une oppo- rtunité en paro-implantologie. Implantodontie 42: 55-62, 2001.
7. Dohan DM, Choukroun J, Diss A, et al.: Platelet-rich fibrin (PRF): a second-generation platelet concentrate. Part II:
platelet-related biologic features. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 101: e45-e50, 2006.
8. Kiuru J, Viinikka L, Myllylä G, Pesonen K, Perheentupa J:
Cytoskeleton-dependent release of human platelet epidermal growth factor. Life Sci 49: 1997-2003, 1991.
9. Marx RE, Carlson ER, Eichstaedt RM, Schimmele SR, Strauss JE, Georgeff KR: Platelet-rich plasma: Growth factor enhancement for bone grafts. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 85: 638-646, 1998.
10. Su CY, Kuo YP, Tseng YH, Su CH, Burnouf T: In vitro release of growth factors from platelet-rich fibrin (PRF): a proposal to optimize the clinical applications of PRF. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 108: 56-61, 2009.
11. Gassling VL, Açil Y, Springer IN, Hubert N, Wiltfang J:
Platelet-rich plasma and platelet-rich fibrin in human cell culture. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 108: 48-55, 2009.
12. Dohan DM, Choukroun J: PRP, cPRP, PRF, PRG, PRGF, FC How to find your way in the jungle of platelet concentrates?
Oral Surg Oral Med Oral Pathol Oral Radiol Endod 103:
305-306, 2006.
13. He L, Lin Y, Hu X, Zhang Y, Wu H: A comparative study of platelet-rich fibrin (PRF) and platelet-rich plasma (PRP) on the effect of proliferation and differentiation of rat osteoblasts in vitro. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 108: 707-713, 2009.
14. Cypher TJ, Grossman JP: Biological principles of bone graft healing. J Foot Ankle Surg 35: 413-417, 1996.
15. Eriksson C, Ohlson K, Richter K, Billerdahl N, Johansson M, Nygren H: Callus formation and remodeling at titanium implants. J Biomed Mater Res 83: 1062-1069, 2007.
16. Cenni E, Ciapetti G, Pagani S, Perut F, Giunti A, Baldini N:
Effects of activated platelet concentrates on human primary cultures of fibroblasts and osteoblasts. J Periodontol 76:
323-328, 2005.
17. Slapnicka J, Fassmann A, Strasak L, Augustin P, Vanek J:
Effects of activated and nonactivated platelet-rich plasma on proliferation of human osteoblasts in vitro. J Oral Maxillofac Surg 66: 297-301, 2008.
18. Italino JE, Richardson JL, Patel-Hett S: Angiogenesis is regulated by a novel mechanism: pro- and antiangiogenic proteins are organized into separate platelet alpha granuales and differentially released. Blood 111: 1227-1233, 2008.
19. Celotti F, Colciago A, Negri-Cesi P, Pravettoni A, Zaninetti R, Sacchi MC: Effect of platelet-rich plasma on migration and proliferation of SaOS-2 osteoblasts: role of platelet- derived growth factor and transforming growth factor-beta.
Wound Repair Regen 14: 195-202, 2006.
20. Ogino Y, Ayukawa Y, Kukita T, Koyano K: The contribution of platelet-derived growth factor, transforming growth factor-beta1, and insulin-like growth factor-I in platelet-rich plasma to the proliferation of osteoblast-like cells. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 101: 724-729, 2006.
21. Dohan Ehrenfest DM, Diss A, Odin G, Doglioli P, Hippolyte MP, Charrier JB: In vitro effects of Choukroun's PRF (platelet-rich fibrin) on human gingival fibroblasts, dermal prekeratinocytes, preadipocytes, and maxillofacial osteo- blasts in primary cultures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 108: 341-352, 2009.
22. Ferreira CF, Carriel Gomes MC, Filho JS, Granjeiro JM, Oliveira Simões CM, Magini Rde S: Platelet-rich plasma influence on human osteoblasts growth. Clin Oral Implants Res 16: 456-460, 2005.
23. Uggeri J, Belletti S, Guizzardi S, et al.: Dose-dependent effects of platelet gel releasate on activities of human osteo- blasts. J Periodontol 78: 1985-1991, 2007.
24. Ivarsson M, McWhirter A, Borg TK, Rubin K: Type I collagen synthesis in cultured human fibroblasts: regulation by cell spreading, platelet-derived growth factor and interac- tions with collagen fibers. Matrix Biol 16: 409-425, 1998.
25. Centrella M, McCarthy TL, Canalis E: Transforming growth factor-beta and remodeling of bone. J Bone Joint Surg Am 73: 1418-1428, 1991.