1
REVIEW ARTICLE
소아에서 예방적 항생제 사용의 적응증과 효과 및 전망
The Use of Prophylactic Antibiotics in Pediatric Urinary Tract Infection: Indication, Effect and Future
Perspective
Jae Shin Park
From the Departm ent of U rology, Daegu Catholic U niversity M edical Center, Daegu, Korea
박재신
대구가톨릭대학교 의과대학 비뇨기과학교실
Many children with urinary tract infection (UTI) and urinary tract abnor- mality such as vesicoureteral reflux (VUR) are given prophylactic anti- biotic to prevent recurrence of UTI and permanent kidney damage.
Occasionally, children with normal urinary tract receive prophylactic an- tibiotic to alleviate the patient suffering and family inconvenience asso- ciated with recurrent symptomatic UTI. These recommendations are mostly opinion based and are derived from studies that were not random- ized and were done before the current renal imaging modalities became available. Recent studies have raised serious doubts about the role of an- tibiotic prophylaxis after UTI by demonstrating the presence of preexist- ing renal scars without UTI in some patients, systematic reviews of pub- lished literature on UTI and VUR, and by comparing randomized pa- tients with VUR who received antibiotic prophylaxis with those who did not receive any prophylaxis. However, the new knowledge has also high- lighted that, apart from skilful management of individual patients, well designed studies are needed to answer the questions on antibiotic prophy- laxis across the spectrum of UTI in different clinical situations. One such study currently underway is the Randomized Intervention for Children With Vesicoureteral Reflux study, which will evaluate the role of anti- biotic prophylaxis in preventing recurrent UTI and renal scarring in young children with VUR. So, it is advisable that until the results of more appropriately designed studies become available, UTI in young chil- dren is considered as a risk factor for renal scarring and each patient is treated with prudence. Regarding antibiotic prophylaxis for antenatal hydronephrosis, routine use is not recommended, but families should re- ceive education on signs and symptoms of UTIs to allow prompt diagnosis and treatment should s UTI occur.
Key Words: Prophylactic antibiotic, Urinary tract infection, Vesicoureteral re- flux, Antenatal hydronephrosis
교신저자 박재신
대구가톨릭대학교 의과대학 비뇨기과학교실
대구시 남구 대명4동 3056-6,
705-718
Tel: 053-650-4662 Fax: 053-623-4660 E-mail: jspark@cu.ac.kr
서 론
소아에서 요로감염 발생 후 요로감염의 재발을 방 지하기 위하여 사용하는 예방적 항생제는 여러 가지
인자에 의하여 그 사용이 결정된다. 즉 환자의 나이 및 요로감염의 발생 횟수를 위시하여 방광요관역류, 신경성방광 및 배뇨습관이상과 같은 동반된 비뇨기 과적인 문제 등이 예방적 항생제 사용의 중요한 변수 가 된다. 이러한 임상적으로 발생 가능한 모든 경우에
서 예방적 항생제의 사용에 대하여 기술하는 것은 내 용이 너무 방대하여 여기에서 모두 기술하는 것은 적 절하지가 않다. 여기에서는 선천성 방광요관역류를 중심으로 이와 관련된 요로감염의 재발과 이로 인하 여 발생하는 신손상의 예방에 있어서 예방적 항생제 사용의 최신 지견과 임신 중에 발견된 산전 수신증과 생후 뒤따르는 수신증에서 예방적 항생제의 사용에 관하여 기술 하고자 한다.
본 론
일반적으로 여아의 7%, 남아의 2%는 생후부터 6세 까지 증상을 가진, 균 배양 검사에서 양성인 요로감염 이 있다.1 영아에서는 첫 번째 요로 감염 후 75%에서 요로감염이 재발하며 1세 이후에는 여아의 40%, 남아 의 30%에서 요로감염이 재발한다.2 이러한 이유로 예 방적 항생제는 방광요관역류를 가진 소아에서 요로 감염의 재발과 이로 인해 추후에 발생하는 신실질의 손상을 예방하기 위하여 많이 사용되어 왔다. 경우에 따라서는 방광요관역류와 같은 비뇨기과적인 이상이 없어도 재발하는 요로감염에서 그 빈도를 줄이기 위 하여 예방적 항생제를 사용하였다. 즉 과거에는 요로 감염 후 예방적 항생제의 사용을 강조하는 수많은 보 고들이 있었다. 그러나 최근에 발표된 보고들은 이러 한 예방적 항생제의 사용에 대하여 의문을 제기하고 있다.
먼저 방광요관역류가 없는 요로감염에 관하여 최 근에 발표된 논문들을 살펴보자. 한 논문에서는 해부 학적 이상이 없는 소아에서 요로 감염 후 예방적 항생 제를 사용한 군을 사용하지 않은 군과 무작위로 비교 하였는데 요로감염의 재발이 치료를 한 군에서는 0-4%, 치료를 하지 않은 군에서는 4.0-16.7%로 보고하 면서 정상요로를 가진 소아에서 요로감염을 예방하 기 위하여 사용하는 예방적 항생제는 그 효용성이 낮 다고 하였다.3
2006년에 Williams는 이미 발표된 5개의 논문을 체 계적으로 다시 조사하였다.4 406명에서 항생제를 10 주에서 12개월 동안 사용하였는데 항생제를 사용한 군은 대조군과 비교하였을 때 항생제가 균배양 검사 에서 양성률은 감소시켰지만 증상을 가진 요로감염 의 예방에는 그 이점은 매우 적었다고 보고하였다. 영 국에서는 의사들의 의견을 기초로 하여 Natiotional Institute for Health and Clinical Excellence (NICE)에서 권
고안을 제시하였는데 영아 및 소아에서 첫 요로감염 후 항생제의 예방적 사용을 추천하지 않는다고 하였 다.2,5
2007년 JAMA에 발표된 한 후향적 보고는 6세 이하 의 74,974명의 병력지를 조사하였다.5 5년 동안 일차 진료의가 환자를 보았을 때 첫 요로감염을 가진 666 명 중 83명에서 요로감염이 재발하였으며 이 중 20명 은 방광요관역류가 없었다. 재발하는 요로감염의 원 인을 분석하였을 때 백인, 3-5세의 나이 및 4-5급 방광 요관역류는 위험인자였으나 성별, 저급의 방광요관역 류 및 항생제 사용은 위험인자가 아니었다. 이 때 예 방적 항생제는 첫 요로감염과 요로감염의 재발 사이 의 기간을 연장시키는 효과가 없었다. 오히려 요로감 염 재발의 원인이 되는 항생제 내성균이 7.5배 높게 출현하였다. 즉 항생제의 예방적 사용은 요로감염의 재발을 감소시키지 못하고 오히려 내성균의 출현을 조장했다.
방광요관역류를 가진 요로감염
방광요관역류는 대부분의 환자에서 시간이 지나면 개선되거나 소멸된다. 전통적인 치료법은 요로감염을 즉각적으로 치료하고 방광요관역류가 소실될 때까지 혹은 수술로 방광요관역류를 교정 할 때까지 장기간 예방적 항생제를 사용하는 것이다. 수술의 적응증은 지속적인 고도의 방광요관역류가 있는 경우, 예방적 항생제 사용에도 불구하고 요로감염이 재발하는 경 우, 항생제 부작용이 있는 경우 및 환자나 부모가 약물 치료에 잘 순응하지 않는 경우였다. American Academy of Pediatrics (AAP),6 Swedish Medical Research Council,7 American Urological Association (AUA)8에서는 방광요관 역류가 있는 소아에서 신손상을 방지하기 위하여 예 방적 항생제의 사용을 권고하였다.6-8 이러한 권고안 은 방광요관역류의 정도, 단측 혹은 양측성, 첫 진단 혹은 추적 관찰 중 신반흔의 유무 및 방광요관역류의 임상 경과 등에 기초하였다. 어떤 내용은 서로 상충하 기도 하는데 AUA는 저등급 방광요관역류에 예방적 항생제 사용을 권고하였고 Swedish Medical Research Council에서는 반대하고 있다. 공통된 점은 항생제 사 용을 결정 할 때 신반흔의 중요성을 강조한 점이다.
AAP에서는 급성기 요로감염을 치료한 후 방사선학적 검사를 시행하고 추후 치료방법이 결정될 때까지 예 방적 항생제의 사용을 권고하였다.
Table 2. Rate of renal scars after acute pyelonephritis in the different groups
Patients with VUR Patients without VUR Prophylaxis No prophylaxis Prophylaxis No prophylaxis Renal scars, n (%) 5/55 (9.0) 2/58 (3.4) 2/45 (4.5) 4/60 (6.6) Table 1. Rate and type of UTI recurrence in the different groups
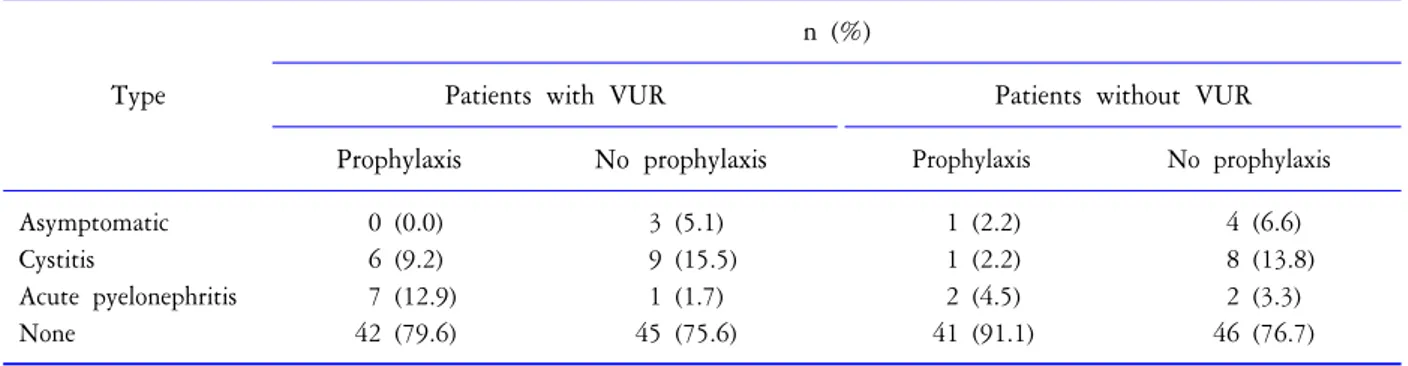
Type
n (%)
Patients with VUR Patients without VUR Prophylaxis No prophylaxis Prophylaxis No prophylaxis
Asymptomatic 0 (0.0) 3 (5.1) 1 (2.2) 4 (6.6)
Cystitis 6 (9.2) 9 (15.5) 1 (2.2) 8 (13.8)
Acute pyelonephritis 7 (12.9) 1 (1.7) 2 (4.5) 2 (3.3)
None 42 (79.6) 45 (75.6) 41 (91.1) 46 (76.7)
방광요관역류에서 예방적 항생제 사용에 관하여 발표된 논문을 살펴보면 1983년 Shindo 등9은 방광요 관역류를 교정하고 요로감염을 예방하여도 신반흔은 계속 진행한다고 하였고, 1992년 Arant10는 방광요관 역류에서 약물 치료를 잘 하여도 중등도 이하의 방광 요관역류에서도 신 손상이 동반된다고 하였다. 2000 년 Cooper 등11은 1-4등급 방광요관역류에서 항생제를 사용하지 않아도 새로운 신반흔은 없었다고 보고하 였다. Dwoskin12의 보고에서는 심한 방광요관역류를 가진 환자의 반수에서 신손상의 증거가 없었고 신손 상의 빈도는 방광요관역류의 정도와 비례하지 않았 다고 하였다.13 또한 신우신염의 빈도는 방광요관역류 소실유무에 관계없이 비슷하다고 하면서 장기간의 항생제 사용에 대하여 의문을 제기하였다.14
그러면 여기서 2000년 이후 비교적 체계적으로 발 표된 논문들을 살펴보자. 2001년 Williams 등15은 그의 논문에서 방광요관역류와 예방적 항생제 사용에 관 하여 지금까지 발표된 논문들을 체계적으로 분석해 보면 대부분의 연구들이 실제 치료효과를 너무 과장 하거나 디자인이 제대로 되지 않았다고 하였다. 2003 년 Wheeler 등16은 증상을 가진 첫 요로감염 후 방광요 관역류의 진단, 여러 가지 치료 방법의 효과 및 뒤 따 르는 신실질 손상을 체계적으로 분석하였다. 즉 방광 요관역류를 찾아내고 이를 치료한 것이 임상적으로 환자에게 중요한 이득을 주었는지를 조사하였다. 결
론으로 예방적 항생제를 사용하거나 방광요관역류를 교정하는 것이 치료를 하지 않았을 때와 비교했을 때 이점이 있었는지는 확실하지 않다고 하였다. 2003년 Gorden 등17의 보고에서도 열성요로감염으로 입원한 소아에서 방광요관역류를 찾아내어 진단하고 이후 일어날 수 있는 신실질 손상의 위험성을 분석 하였을 때 방광요관역류를 찾아내는 것이 신실질 손상의 예 측인자로서의 역할이 크지 않다고 하였다.
예방적항생제 사용을 추적관찰만 한 경우와 비교한 최근의 논문
방광요관역류가 있는 소아에서 예방적 항생제를 사용한 군을 추적관찰만 한 경우와 비교한 논문을 살 펴보자. 2006년 Garin 등18은 급성신우신염을 가진 3개 월에서 18세 사이의 소아 263명을 조사하였다. 이 중 3개월에서 12세 사이, 1-3등급 방광요관역류를 가진 113명과 3개월에서 17세 사이, 방광요관역류가 없는 105명이 포함된 218명을 1년 동안 관찰 하였다. 항생 제를 사용한 군과 사용하지 않은 군을 무작위로 나누 었으며 Dimercaptosuccinic acid (DMSA) 신주사를 신반 흔을 보기 위하여 시행하였다. 1년 뒤 218명 중 13명 (5.9%)에서 신반흔이 발생하였고, 요로감염, 신우신염 및 신반흔의 발생에서 두 군 간의 차이는 없었다 (Table 1, 2). 즉 이 논문은 저등급 방광요관역류는 예
Fig. 1. Kaplan-Meier IFS curves considering the absence of recurrence of UTI (A) or febrile UTI (B). There was no significant difference between group treated with antibiotic prophylaxis and control group, regardless of whether UTI or febrile UTI was considered.
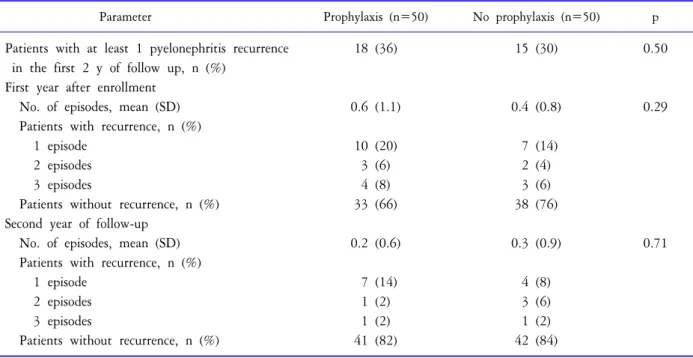
Table 3. Rate of pyelonephritis recurrence during the first 2 years of follow-up
Parameter Prophylaxis (n=50) No prophylaxis (n=50) p
Patients with at least 1 pyelonephritis recurrence 18 (36) 15 (30) 0.50 in the first 2 y of follow up, n (%)
First year after enrollment
No. of episodes, mean (SD) 0.6 (1.1) 0.4 (0.8) 0.29 Patients with recurrence, n (%)
1 episode 10 (20) 7 (14)
2 episodes 3 (6) 2 (4)
3 episodes 4 (8) 3 (6)
Patients without recurrence, n (%) 33 (66) 38 (76) Second year of follow-up
No. of episodes, mean (SD) 0.2 (0.6) 0.3 (0.9) 0.71 Patients with recurrence, n (%)
1 episode 7 (14) 4 (8)
2 episodes 1 (2) 3 (6)
3 episodes 1 (2) 1 (2)
Patients without recurrence, n (%) 41 (82) 42 (84) 방적 항생제 사용이 필요하지 않다고 강조하였다.
2008년 Roussey-Kesler 등19은 1개월에서 3년 사이의 1-3등급 방광요관역류환자 환아 225명에서 항생제를 사용한 군을 사용하지 않은 군과 무작위로 나누어 비 교하였다. 18개월 후에 조사하였을 때 요로감염의 발 생은 항생제군 17%, 대조군 26%로 (p=0.2) 두 군 간에 유의한 차이가 없었다 (Fig. 1). 방광요관역류의 정도 에 따른 차이도 없었으나 3등급 방광요관역류를 가진 남아에서는 요로감염의 발생이 치료한 군에서 의미
있게 낮았다 (p=0.017). 즉 이 논문에서는 3등급 남아 이외의 저등급 방광요관역류는 예방적 항생제 사용 이 필요하지 않다고 강조하였다.
2008년 Pennesi 등20은 급성신우신염 후 2-4등급 방 광요관역류 100명 환아에서 항생제를 사용한 군과 사 용하지 않은 군을 무작위로 나누어 비교하였다. 평균 환아 나이는 항생제군은 9개월, 항생제를 사용하지 않은 군은 8.3개월이었다. 항생제를 사용한 군은 2년 동안 예방적 항생제를 사용하고 이후 2년 동안 관찰
Fig. 2. Algorithm for postnatal evaluation of antenatal hydronephrosis. APD: anterior-posterior diameter, UTI: urinary tract infection, VCVG: voiding cystourethrogram, VUR: vesicoureteral reflux.
Table 4. Patients with persistent VUR at the end of the second and fourth years of follow-up
Parameter Prophylaxis
(n=50), n (%)
No prophylaxis (n=50), n (%)
Persistent VUR 31 (62) 40 (80)
at the end second year Grade of VUR
I 3 (6) 4 (8)
II 10 (20) 12 (24)
III 15 (30) 20 (40)
IV 3 (6) 4 (8)
Persistent VUR 26 (52) 25 (50)
at the end fourth year Grade of VUR
I 3 (6) 3 (6)
II 7 (14) 5 (10)
III 13 (26) 14 (28)
IV 3 (6) 3 (6)
만 하였고, 양군에서 4년 간 추적관찰 하였다. DMSA 신주사를 신반흔을 보기 위하여 시행하였다. 급성신 우신염의 재발은 2년 뒤 (항생제 사용군: 36%, 사용하 지 않은 군: 30%) 및 4년 뒤에 차이가 없었다. DMSA
신주사는 2, 3, 4급 방광요관역류에서 0, 30, 67%가 비 정상이었는데 2년 뒤 신반흔의 차이는 없었고 4년 동 안 새로운 신반흔의 발생은 없었다 (Table 3, 4). 이 논 문에서도 2-4등급 방광요관역류에서 예방적 항생제 의 이점이 없다고 하였다.
최근에 발표된 이러한 연구들은 급성신우신염을 치료한 후에 요로감염의 재발 및 신반흔을 예방하기 위하여 사용하는 예방적 항생제는 방광요관역류의 유무에 관계없이 일부 소아에서는 그 역할이 없다는 것을 말한다. 그러나 모든 방광요관역류 환아에서 예 방적 항생제의 역할이 없다는 것은 아니라고 하겠다.
최근에 발표된 이러한 연구들도 엄밀한 의미에서 그 조사의 한계점이 있는데 그것은 이러한 연구들이 이 중 맹검 검사가 아니고, 환아의 수 및 추적기간이 충분하지 않으며, 대상군의 나이 간격이 넓으며 소변 을 가리지 못하는 영아에서 있을 수밖에 없는 소변 집뇨 방법의 문제 등이라고 하겠다. 또한 DMSA 신주 사의 판독에 있어서 판독자 간의 차이 등도 짚고 넘어 가야 할 점이라고 하겠다.
산전 수신증에서 예방적 항생제 사용
전통적으로 산전 수신증 (anterior posterior diameter (APD) >5 mm)이 있으면 모든 신생아에서 예방적 항 생제를 사용하고 영상의학적 검사로 초음파와 배뇨 중방광요도조영술을 시행하였다.21-24 심지어 출생 후 초음파검사가 정상인 경우도 방광요관역류를 찾기 위해 배뇨중방광요도조영술을 시행하였다.21-24 그러 나 최근의 연구결과는 출생 후 초음파검사가 정상이 면 방광요관역류는 경미하며 대부분 자연 소실된다 고 보고하고 있다.25-27 즉 경미한 방광요관역류는 놓 치더라도 임상적인 경과는 별 문제가 없으며 이러한 이유로 예방적 항생제를 사용할 필요는 없다고 하였 다.20 다만 요로감염이 발생하면 바로 진단하고 치료 할 수 있도록 부모를 교육하는 것이 중요하다고 하였 다. 물론 심한 수신증이 있는 경우는 아직까지 예방적 항생제를 사용하여야 한다.28 Fig. 2는 산전 수신증을 가진 신생아의 산후 검사를 보여준다.29
예방적 항생제 사용의 제한점
예방적 항생제를 장기간 사용하면 여러 가지 문제 가 발생할 수 있다. 먼저 예방적 항생제를 사용함에도 불구하고 방광요관역류를 가진 소아의 25-38%에서는 돌파감염이 발생한다.14,30 또 다른 문제는 항생제를 장기간 사용하였을 때 발생하는 내성균의 출현이다.
한 조사에 의하면 6개월 동안 조사하였을 때 항생제 를 4주 이상 사용하면 사용하지 않았을 때와 비교하 여 더 많은 Escherichia coli 내성균이 발생한다고 하였다 [odds ratio (OR) 13.9, 95% confidence interval (CI) 8.2-23.5].31 한편 1991년과 비교하였을 때 1999년은 소 아요로감염에서 자주 사용하는 항생제에 대한 항생 제 감수성이 전체적으로 감소하였다는 연구보고도 있다.30 또한 소아의 약 10%에서는 장기적 예방적 항 생제 사용의 부작용이 있는데 대부분은 첫 6개월에 나타난다고 한다. 즉 sulfamethoxazole/trimethoprim은 소 화기계 증상, 피부 발진, 간독성 및 혈액학적 부작용 이 있고 nitrofurantoin은 소화기계 증상을 나타낸다.
Sulfamethoxazole/trimethoprim은 골수 억제 같은 좀 더 심 한 부작용이 있을 수 있으며 드물기는 하지만 Stevens- Johnson syndrome도 일어날 수 있다.32,33 또한 장기간에 걸쳐서 매일 약물을 복용하는데 대한 환자의 순응도
도 문제가 된다. 한 연구에 의하면 97%의 부모가 매일 예방적 항생제를 복용시켰다고 하지만 환아의 소변 에서는 31%에서만 약물이 검출 된다고 한다.34 또한 방광요관역류소실을 증명하기 위하여 어린 소아에서 반복적으로 시행하는 배뇨중방광요도조영술의 불편 함도 환아에게 큰 문제가 된다.
결 론
예방적 항생제는 지난 수 십 년 동안 방광요관역류 를 가진 소아에서 요로감염 후에 요로감염을 예방하 기 위하여 많이 사용되었다. 이러한 예방적 항생제의 사용 행태는 대부분 체계적으로 조사되지 않은 연구 결과에 근거하였다. 최근의 연구결과들은 예방적 항 생제의 역할에 많은 의문점을 제기하고 있다. 이의 근 거로는 잘 디자인 된 체계적인 최근의 연구결과들이 며 또한 일부 신생아에서 요로감염 없이 발견되는 신 반흔 및 요로감염에서 변비 및 배뇨장애의 역할 등이 다. 그러나 이러한 최근의 연구결과들도 그 한계가 있 는 만큼 다양한 임상적인 상황에서 예방적 항생제 사 용의 해법을 제시하기 위해서는 향후 좀 더 잘 디자인 된 연구들이 필요하다. 이러한 노력 중의 하나로 현재 Randomized Intervention for Children With Vesicoureteral Reflux study가 진행 중인데35 이것은 다기관, 전향적, 무작위, 위약 대조군 연구이며 향후 방광요관역류를 가진 소아에서 요로감염의 재발과 신반흔을 예방하 는데 있어서 예방적 항생제의 역할에 대하여 답을 내 놓을 수 있을 것으로 생각한다. 요로감염 후 발생하는 신반흔은 아직까지 중요한 문제이기 때문에 적절히 조사된 연구결과들이 나오기까지는 요로감염과 방광 요관역류를 가진 환아는 그 치료에 있어서 신중하게 판단하여야 할 것으로 생각한다.
REFERENCES
1. Marild S, Jodal U. Incidence rate of first-time symptomatic urinary tract infection in children under 6 years of age.
Acta Paediatr 1998;87:549-52
2. National Institute for Health and Clinical Excellence.
Urinary tract infection: diagnosis, treatment, and long- term management of urinary tract infection in children.
National Institute of Health and Clinical Excellence London, England. A very controversial report that is not evidence based. 2007;1-136
3. Le Saux N, Pham B, Moher D. Evaluating the benefits of
antimicrobial prophylaxis to prevent urinary tract infections in children: a systematic review. CMAJ 2000;163:523-9 4. Williams GJ, Lee A, Craig JC. Long-term antibiotics for
preventing recurrent urinary tract infection in children.
Cochrane Database Syst Rev 2006CD001534
5. Conway PH, Cnaan A, Zaoutis T, Henry BV, Grundmeier RW, Keren R. Recurrent urinary tract infections in children: risk factors and association with prophylactic anti- microbials. JAMA 2007;298:179-86
6. American Academy of Pediatrics, Committee on Quality Improvement, Subcommittee on Urinary Tract Infection.
Practice parameter:. the diagnosis, treatment, and evalua- tion of the initial urinary tract infection in febrile infants and young children. Pediatrics 1999;103(4 Pt1):843-52 7. Jodal U, Lindberg U. Guidelines for management of
children with urinary tract infection and vesicoureteric reflux. Recommendations from a Swedish state-of-the-art conference. Swedish Medical Research Council. Acta Pae- diatr Suppl 1999;88:87-9
8. Elder JS, Peters CA, Arant BS Jr. Pediatric vesicoureteral reflux guidelines panel summary report on the manage- ment of primary vesicoureteral reflux in children. J Urol 1997;157:1846-51
9. Shindo S, Bernstein J, Arant BSJ Jr. Evolution of renal segmental atrophy (Ask-Upmark kidney) in children with vesicoureteric reflux: radiographic and morphologic studies.
J Pediatr 1983;102:847-54
10. Arant BSJ Jr. Medical management of mild and moderate vesicoureteral reflux: followup studies of infants and young children. A preliminary report of the Southwest Pediatric Nephrology Study Group. J Urol 1992;148(5 Pt 2):1683-7 11. Cooper CS, Chung BI, Kirsch AJ, Canning DA, Snyder
HM 3rd. The outcome of stopping prophylactic antibiotics in older children with vesicoureteral reflux. J Urol 2000;
163:269, 72; discussion 272-3
12. Dwoskin JY, Perlmutter AD. Vesicoureteral reflux in chil- dren: a computerized review. J Urol 1973;109:888-90 13. Hannerz L, Wikstad I, Johansson L, Broberger O, Aperia
A. Distribution of renal scars and intrarenal reflux in children with a past history of urinary tract infection. Acta Radiol 1987;28:443-6
14. Tamminen-Mobius T, Brunier E, Ebel KD. Cessation of vesicoureteral reflux for 5 years in infants and children allocated to medical treatment. The International Reflux Study in Children. J Urol 1992;148:1662-6
15. Williams G, Lee A, Craig J. Antibiotics for the prevention of urinary tract infection in children: a systematic review of randomized controlled trials. J Pediatr 2001;138:868-74 16. Wheeler D, Vimalachandra D, Hodson EM, Roy LP, Smith
G, Craig JC. Antibiotics and surgery for vesicoureteric reflux: a meta-analysis of randomised controlled trials. Arch Dis Child 2003;88:688-94
17. Gordon I, Barkovics M, Pindoria S, Cole TJ, Woolf AS.
Primary vesicoureteric reflux as a predictor of renal damage in children hospitalized with urinary tract infection: a systematic review and meta-analysis. J Am Soc Nephrol 2003;14:739-44
18. Garin EH, Olavarria F, Garcia Nieto V, Valenciano B, Campos A, Young L. Clinical significance of primary vesi- coureteral reflux and urinary antibiotic prophylaxis after acute pyelonephritis: a multicenter, randomized, controlled study. Pediatrics 2006;117:626-32
19. Roussey-Kesler G, Gadjos V, Idres N, Horen B, Ichay L, Leclair MD, et al. Antibiotic Prophylaxis for the prevention of recurrent urinary tract infection in children with low grade vesicoureteral reflux: results from a prospective ran- domized study. J Urol 2008;179:674-9
20. Pennesi M, Travan L, Peratoner Ll. Is antibiotic prophy- laxis in children with vesicoureteral reflux effective in pre- venting pyelonephritis and renal scars? A randomized, con- trolled trial. Pediatrics 2008;121:e1489-94
21. Jaswon MS, Dibble L, Puri Sl. Prospective study of out- come in antenatally diagnosed renal pelvis dilatation. Arch Dis Child Fetal Neonatal Ed 1999;80:F135-8
22. Phan V, Traubici J, Hershenfield B, Stephens D, Rosen- blum ND, Geary DF. Vesicoureteral reflux in infants with isolated antenatal hydronephrosis. Pediatr Nephrol 2003;
18:1224-8
23. Alconcher L, Tombesi M. Mild antenatal hydronephrosis:
management controversies. Pediatr Nephrol 2004;19:819- 20
24. Tibballs JM, De BR. Primary vesicoureteric reflux: how useful is postnatal ultrasound? Arch Dis Child 1996;75:
444-7
25. Coelho GM, Bouzada MC, Pereira AK. Outcome of isolated antenatal hydronephrosis: a prospective cohort study. Pediatr Nephrol 2007;22:1727-34
26. Lidefelt KJ, Herthelius M. Antenatal hydronephrosis: in- fants with minor postnatal dilatation do not need pro- phylaxis. Pediatr Nephrol 2008;23:2021-4
27. Merlini L, Parvex P, Anooshiravani-Dumont M, Girardin E, Hanquinet S. Postnatal management of isolated mild pelvic dilatation detected in antenatal period. Acta Paediatr 2007;96:1131-4
28. Mallik M, Watson AR. Antenatally detected urinary tract abnormalities: more detection but less action. Pediatr Nephrol 2008;23:897-904
29. Becker AM. Postnatal evaluation of infants with an abnor- mal antenatal renal sonogram. Curr Opin Pediatr 2009;21:
207-13
30. Birmingham Reflux Study Group. Prospective trial of operative versus nonoperative treatment of severe vesicou- reteric reflux in children: five years’ observation. Br Med J (Clin Res Ed) 1987;295:237-41
31. Allen UD, MacDonald N, Fuite L, Chan F, Stephens D.
Risk factors for resistance to "first-line" antimicrobials among urinary tract isolates of Escherichia coli in children.
CMAJ 1999;160:1436-40
32. Karpman E, Kurzrock EA. Adverse reactions of nitrofu- rantoin, trimethoprim and sulfamethoxazole in children. J Urol 2004;172:448-53
33. Bollgren I. Antibacterial prophylaxis in children with uri- nary tract infection. Acta Paediatr Suppl 1999;88:48-52
34. Uhari M, Nuutinen M, Turtinen J. Adverse reactions in children during long-term antimicrobial therapy. Pediatr Infect Dis J 1996;15:404-8
35. Keren R, Carpenter MA, Hoberman A, Shaikh N, Matoo TK, Chesney RW, et al. Rationale and design issues of the Randomized Intervention for Children With Vesicoureteral Reflux (RIVUR) study. Pediatrics 2008;122(Suppl 5):S240- 50