접수일: 2017년 7월 21일, 게재승인일: 2017년 11월 6일 책임저자: 김상준, 서울시 강남구 일원로 81
06351, 성균관대학교 의과대학 삼성서울병원 재활의학과
Tel: 02-3410-6069, Fax: 02-3410-0057 E-mail: [email protected]
척추관 협착증 환자에서 유치 경막외 도관을 이용한 생리식염수와 스테로이드의 지속적 투여 효과
성균관대학교 의과대학 삼성서울병원 재활의학교실1, 신경외과학교실2, 성균관대학교 의과대학 강북삼성병원 재활의학교실3
이한나1ㆍ김은상2ㆍ도종걸3ㆍ김경아1ㆍ문창원1ㆍ김상준1
Continuous Infusion of Saline with Dexa- methasone by Indwelling Epidural Catheter in Patients with Spinal Stenosis
Hannah Lee, M.D.1, Eun Sang Kim, M.D.2, Jong Geol Do, M.D.3, Kyung Ah Kim, M.D.1, Chang Won Moon, M.D.1 and Sang Jun Kim, M.D.1
Departments of 1Physical and Rehabilitation Medicine,
2Neurosurgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, 3Department of Physical and Rehabilitation Medicine, Kangbuk Samsung Hospital, Sungkyunkwan University School of Medicine, Seoul, Korea Objective: To find the therapeutic effect of continuous in- fusion of normal saline mixed with corticosteroid on spinal stenosis patients with poor outcome to conventional epi- dural steroid injection. Method: Forty-two spinal stenosis patients who had failed to improve after epidural steroid injection were enrolled. A bolus of 10 mg of dexamethasone and 1,500 I.U hyaluronidase mixed with 1 ml of ropivacaine was injected and a total of 96 ml dexamethasone solution was infused over 48 hours at flow rate of 2 ml/hour by indwelling epidural catheter. The Oswestry Disability Index (ODI) was evaluated before and 1 month after procedure and the improvement of pain was evaluated 3 months after the procedure. Results: Average ODI showed a significant change from 50.8 ± 18.2 to 45.7 ± 17.6 (p=0.025).
Fourteen patients showed ‘much improvement’, 12 patients showed ‘slight improvement’ and 16 patients showed ‘no improvement’ at 3 months. There was no overlap in con- fidence intervals of change in ODI between responders and non-responders. Conclusion: Continuous infusion of normal saline mixed with corticosteroid on spinal stenosis by indwelling epidural catheter was effective at 3 months for clinical improvement in about 61.9% of patients who had failed with conventional epidural steroid injection therapy. (Clinical Pain 2017;16:88-94)
Key Words: Spinal stenosis, Indwelling catheter, Epidural, Pain
INTRODUCTION
Spinal stenosis is a degenerative spine disease which narrows the spinal canal by herniated intervertebral disc, ligamentum flavum thickening, and facet joint hyper- trophy.1 There have been many conservative treatments for spinal stenosis including oral medication, physical therapy, and epidural steroid injection but no conservative treatment provides a positive long-term benefit and rarely, a short-term pain relief.2 Spinal decompression surgery can relieve the symptoms in long-term follow up.3 However, there is little evidence for improving walking ability,4 and it can cause spinal instability later on.5
Many articles have evaluated epidural steroid injection in the spinal stenosis, and recent meta-analysis revealed that it had limited evidence in providing long-term efficacy.
Also, it did not show better outcome than epidural lido- caine injection alone.6-9 Recently, epidural adhesiolysis has been put to practice and been used in chronic lumbosacral radiculopathy,10,11 the failed back syndrome,12 and spinal stenosis,13 in cases which were not responsive to the epi- dural steroid injection. Epidural adhesiolysis has been per- formed by a navigable catheter to mechanically disrupt scar tissue14 or by the indwelling catheter to infuse steroid and saline into the epidural space over a 3-day course.10 The possible mechanisms of epidural adhesiolysis are washout of inflammatory cytokines, relieved adhesion by the ap- plied water pressure with high volume, and the hyper- osmolar hyper-depolarization by the hypertonic saline.15
We hypothesized that continuous infusion of normal sal- ine into the epidural space would show better outcome compared to the intermittent epidural injection if the mech- anisms are washout of inflammatory cytokines and relieved
adhesion due to water pressure and high volume. One pilot study was conducted to infuse the normal saline mixed with corticosteroid through the indwelling catheter and in- fusion pump in patients with lumbar radiculopathy over a 72-hour period and suggested treatment with indwelling catheter as safe and effective method.16 The aim of this study was to find the therapeutic effect of continuous in- fusion of normal saline mixed with corticosteroid on the spinal stenosis patients with poor response to conventional epidural steroid injection.
MATERIALS AND METHODS
This study was approved by our Institutional Review Board (IRB approval number: 2016-05-052). Patients who were recruited for this study from January 2014 to October 2016 had been diagnosed with spinal stenosis and had re- ceived the epidural steroid injection before but had shown poor improvement.
Diagnosis of spinal stenosis was done by clinical symp- toms including neurogenic claudication and the lumbo- sacral magnetic resonance images (MRI). Neurogenic clau- dication was defined as increasing pain radiating to legs during walking or taking an extended lumbar posture and reliving of pain after resting or taking a flexed lumbar posture.17 Lumbosacral MRI showed central canal or fora- minal narrowing caused by the herniated disc, ligamentum flavum hypertrophy, and bony spur. The previous epidural steroid injection was restricted to interlaminar, caudal, or transforaminal approaches between one and three months prior to the participation of our study. With regard to pa- tient-reported pain outcome, the ‘poor improvement’ was defined as being less than 30% improvement of subjective symptom after the injection and ‘slight improvement’ was defined as 30∼50% improvement, and ‘much improve- ment’ was defined as more than 50% improvement of sub- jective symptom. These criteria were based on a previous study.18 Also, the changes of medication were grouped into the following 4 grades: increase, maintain, decrease, stop medication. Based on the medication that the patients had taken before the intervention, ‘increase medication’ was de- fined as increasing the quantity of same drugs or number of drugs and ‘decrease medication’ was defined as decreas- ing the quantity or number of drugs.
Patients underwent blood examination including com-
plete blood cell count, blood chemistry, and coagulation battery and were included in our study if there were no ab- normalities in the results. The Oswestry Disability Index (ODI) was checked for the evaluation of the pain and disability. We selected ODI for the evaluation because the change in ODI correlates strongly with patient satisfaction after treatment compared to other parameters.19
After acquiring the written consent of the procedure from the patients, they were admitted and received the in- dwelling catheter procedure during hospitalization. The procedure was performed in the air-clean room, which con- tained the fluoroscopy (Model: Artis Zee Ceiling, Siemens Medical Solutions, Erlangen, Germany). Patients lay on the table in the prone position. The skin of the coccyx area was sterilized with 1% chlorhexidine. After checking the sacral hiatus through the angiographic image, 1% lidocaine sol- ution was injected into the sacral hiatus for skin anesthesia.
A 16-gauge Tuohy needle with stylet was inserted into the sacral hiatus and progressed to the S3 vertebral body. After removing the stylet, a curved epidural catheter (EpistimⓇ, Sewoon Medical Corp., Seoul, Korea) was inserted. By controlling the curved part, the catheter tip was made to locate at the most stenotic area, which was confirmed by the contrast dye (IobrixⓇ, Taejoon Pharm Co. Ltd., Seoul, Korea) (Fig. 1A). Three-dimensional computed tomo- graphic images via the angiography were acquired from 2 patients to check the accurate position of catheter tip, and several directional views of two-dimensional images via the same device were acquired from other patients to check the accurate position of catheter tip (Fig. 1B). A bolus of 10 mg of dexamethasone sodium phosphate (5 mg/ml;
Yuhan Corp., Seoul, Korea) and 1,500 I.U hyaluronidase (H-laseⓇ, LNH Pharm, Seoul, Korea) mixed with 1 ml of ropivacaine HCl (RopivaⓇ, Huons Co. LTD, Seongnam, Korea) was injected. After the injection, the epidural cathe- ter was fixed with an adhesive patch and connected to an infusion pump. A total of 96 ml dexamethasone solution (20.0 mg of dexamethasone mixed with 92 ml of normal saline) was slowly infused over 48 hours at flow rate of 2 ml/hour. After the procedure, the epidural catheter was removed and the patients were discharged to home. The ODI was evaluated one month after the discharge and the improvement of pain was evaluated three months after the discharge.
Statistical analysis was performed using SPSS for
Fig. 1. The most stenotic area (arrow) was determined by magnetic resonance images (1A and 1E). The epidural catheter tip (arrow) was made to locate at the most stenotic area (1B and 1F), which was confirmed by the contrast dye (1C and 1G). Three-dimensional computed tomographic images via the angiography were acquired to check the accurate position of catheter tip (arrow, 1D and 1H).
Windows version 20.0 statistical software (SPSS, Inc, Chicago, Illinois, USA) and p-value<0.05 was considered to be statistically significant. Wilcoxon signed rank test was conducted for comparison of ODI before and one month after the procedure and Fisher's exact test was used for statistical analysis of patient-reported pain outcome.
The differences between responder and non-responder groups were assessed using Mann-Whitney U test.
The possible complications from the indwelling catheter technique including dural puncture, motor weakness, in- fection, and bleeding were investigated during the study period.
RESULTS
A total 42 patients (32 women and 10 men) were in- cluded in our study and underwent the indwelling epidural catheter procedure. Average age was 65.2 ± 12.8 years.
Average duration of symptom was 17.2 ± 22.2 months and
initial average ODI was 50.8 ± 18.2. All participants had undergone epidural injection at least once in the past.
Average number of previous epidural injections was 2.6 ± 1.6 and maximal number of previous epidural injections was 7. In detail, route of administration were trans- foraminal approach in 18 patients, interlaminar approach in 9 patients, caudal approach in 6 patients, and mixed ap- proach in 9 patients. Indwelling catheter was fixed at the level of L3-4 in 4 patients, L4-5 in 30 patients, and L5-S1 in 8 patients.
Two patients complained of bilateral lower extremity weakness and urinary incontinence several hours after the indwelling catheter procedure, and the indwelling catheter was removed immediately. The symptoms disappeared af- ter removal of the indwelling catheter and these patients were discharged to home with oral medication.
One month after the procedure, average ODI signifi- cantly improved from 50.8 ± 18.2 to 45.7 ± 17.6 (95%
confidence interval 0.31∼9.83, p-value in Wilcoxon sign-
Table 1. Correlation between the Changes of Medication and the Improvement of Pain at 3 Months after Indwelling Catheter Procedure
Poor improvement
Slight improvement
Much improvement
Increase medication 12 0 0
Maintain medication 4 8 0
Decrease medication 0 4 2
Stop medication 0 0 12
Fisher's exact test showed significant correlation between the change of medication and the improvement of pain (p-value<
0.001).
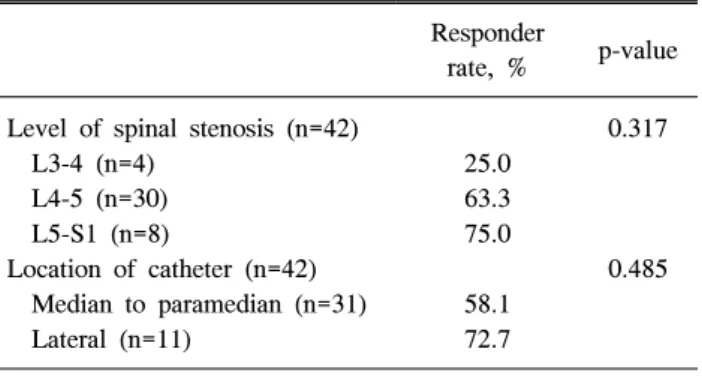
Table 2. Responder Rate According to the Level of Spinal Stenosis and Location of Catheter
Responder
rate, % p-value Level of spinal stenosis (n=42) 0.317
L3-4 (n=4) 25.0
L4-5 (n=30) 63.3
L5-S1 (n=8) 75.0
Location of catheter (n=42) 0.485
Median to paramedian (n=31) 58.1
Lateral (n=11) 72.7
Fig. 2. Square and bar mean average and 95% confidence inter- vals of change in ODI, respectively. Confidence intervals of change in ODI between responder (n=26) and non-responder (n=16) groups were not overlapped (p-value in Mann-Whitney U test=0.05).
ed rank test=0.025).
Three months after the procedure, 12 patients increased their oral medication for pain control, 12 patients did not change their medication, 6 patients decreased oral medi- cation in dosage or frequency, and 12 patients stopped the medication. Oral medication consisted of nonsteroidal an- ti-inflammatory drugs and anticonvulsants with or without prostaglandin E1. According to patient-reported pain out- come, 14 patients showed ‘much improvement’, 12 patients showed ‘slight improvement’ and 16 patients showed ‘no improvement’. There was statistically significant correla- tion between the change of medication and the improve- ment of pain (p-value in Fisher's exact test<0.001) as pre- sented in the Table 1.
When we divided the patients into responders (‘much improvement’ and ‘slight improvement’ without increasing the medication) and non-responders (‘no improvement’ or increasing the medication), 26 patients (61.9%) showed clinical improvement after indwelling catheter procedure among the total 42 patients who had not responded to the conventional epidural injection. Confidence intervals of change in ODI between these two groups were not over- lapped either (95% confidence interval 2.11∼16.46 in res- ponder and −4.76∼1.23 in non-responder, p-value in Mann-Whitney U test=0.05, Fig. 2). However, there were no significant differencesin age and sex between res- ponders and non-responders. Also, the route of admin- istration and number of previous epidural injections was not significantly different between groups (2.5 ± 1.6 in res- ponders and 2.8 ± 1.6 in non-responders, p-value in Mann-Whitney U test=0.522).
There was no significant correlation between the im- provement of symptom and the level of spinal stenosis or the location of the catheter (p-value in Fisher's exact test=0.317 and 0.485, respectively, Table 2).
DISCUSSION
We found that continuous infusion of normal saline mixed with dexamethasone by indwelling epidural catheter over 48 hours produced a significant improvement of pain during 3 months after the injection in about 61.9% patients who had poor response to conventional epidural steroid injection. There were 2 cases of bilateral lower extremity weakness and urinary incontinence after the procedure but these complications disappeared after removal of the catheter.
This is the first study on the effects of continuous in- fusion by an indwelling epidural catheter targeting the spi- nal stenosis patients without benefit from conventional epi- dural steroid injections. Change in ODI and patient-re- ported pain outcome showed significant improvement of pain at one and three months after procedure, respectively.
Although we did not compare the outcome of indwelling epidural catheter with that of conventional epidural in- jection in this study, it is presumed that the indwelling epi- dural catheter has a stronger effect in pain reduction than conventional epidural injection as about 61.9% of patients had clinical improvement for whom conventional epidural injection was not effective.
Average change of ODI was 5.1 which was less than the minimal clinically important difference for ODI,20 but the average change of ODI in responder group was 9.3 which was similar to the minimal clinically important difference for ODI. In fact, there was less change in ODI compared to other studies using same outcome measure after epidural steroid injection.21,22 One possible explanation for our find- ings is that the target of this study was spinal stenosis that conventional epidural injections was ineffective.
We did not investigate the inflammatory cytokines in this study as inflammatory cytokines related to the herni- ated lumbar disc or spinal stenosis are not detected in the usual enzyme-linked immunosorbent assay (ELISA).23 Although the inflammatory effect of epidural catheter on the epidural tissues outweighs anti-inflammatory effect of the infusion of the drugs via the epidural catheter,24 we speculate that possible therapeutic mechanism of epidural saline infusion by indwelling epidural catheter might be the washout of inflammatory cytokines and the expansion ef- fect of high volume (96 ml) of saline.
In an animal study,25 continuous epidural infusion led to a more localized distribution of medications than a single bolus injection, therefore our protocol of continuous in- fusion into the most stenotic area might be better than other protocols of epidural neurolysis.10,13
In our study, there were no complications except tempo- rary bilateral lower extremity weakness and urinary incontinence. We postulate that these side effects might be due to the leakage of ropivacaine into the intrathecal space as they disappeared after removal of the catheter. According to Goeller et al.26 continuous infusion into the epidural space does not increase pressure at the epidural space The
side effect demonstrated in this study is less likely due to increased epidural space pressure and we can suspect that the leakage of ropivacaine into the intrathecal space might have been due to dural puncture by the indwelling catheter.
The epidural catheter resided in the epidural space for 48 hours, and there is no guideline on how long the epi- dural catheter can stay at the epidural space. One mortality has been reported of bupivacaine crystal deposits after a long-term epidural infusion27 and epidural breakages have been described in several studies.28 For our protocol, the optimal and maximal possible duration of indwelling cathe- ter must be specified for better and safer protocol of this indwelling epidural technique.
No patient in ‘much improvement’ or ‘slight improve- ment’ group increased their medication at 3 months. But, 8 patients in ‘slight improvement’ group maintained oral medication after intervention. The reason why they wanted to keep their oral medication was that pain occurred in oth- er sites, such as knee joint.
There was no significant difference in age, sex, and ini- tial ODI between ‘much improvement’, ‘slight improve- ment’, and ‘no improvement’ groups. However, a trend was found that responder rate in improvement of pain in- creased as the level of spinal stenosis was lowered.
Although this was not statistically significant, it is assumed that the lesion with the higher level is more likely to be involved with multilevel nerve roots.
Unfortunately, because of small sample size, we did not find why some patients showed ‘much improvement’ while others did not after the same indwelling catheter. Further study must be conducted to elucidate the prognostic factors of indwelling catheter procedure. There were several limi- tations in our study. First, previous epidural steroid in- jections to patients in this study were performed by multi- ple physicians at various hospitals. The effect of procedure may vary depending on the practitioner. However, we could not estimate the quality of procedures or physicians’
competence in this study. The other was the study design, which was not a randomized controlled double blind study.
Indwelling catheter procedure necessitated admission at the hospital, which made conduction of a double blind study difficult as a comparator arm with transforaminal epidural injection which would not necessitate admission to the hos- pital, also, it would have been difficult to match the two experimental arms. To make our results more compelling,
a prospective randomized controlled study is necessary. In addition, there was the absence of a long-term follow up.
The last follow up period was at 3 month, which might be insufficient to evaluate the long-term effect of indwelling catheter procedure on spinal stenosis. Therefore, a long- term follow up study must be conducted to fully evaluate the long-term effect of the indwelling catheter procedure on spinal stenosis.
CONCLUSION
In summary, the present study demonstrates that con- tinuous infusion of normal saline mixed with corticosteroid on the spinal stenosis by indwelling epidural catheter was effective at 3 months for clinical improvement in about 61.9% of patients with spinal stenosis that conventional epidural steroid injection had failed to have clinical effectiveness. Further randomized controlled study with long-term follow up will be required to consolidate this ef- fect of indwelling epidural catheter procedure.
ACKNOWLEDGEMENT
This work was supported by the ICT R&D program of IITP/MSIP (B0101-17-1081, Development of ICT based software platform and service technologies for medical 3D printing applications) and by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI16C1104).
REFERENCES
1. Lee JY, Whang PG, Lee JY, Phillips FM, Patel AA.
Lumbar spinal stenosis. Instr Course Lect 2013; 62:
383-396
2. Issack PS, Cunningham ME, Pumberger M, Hughes AP, Cammisa FP, Jr. Degenerative lumbar spinal stenosis: eval- uation and management. J Am Acad Orthop Surg 2012; 20:
527-535
3. Kovacs FM, Urrutia G, Alarcon JD. Surgery versus con- servative treatment for symptomatic lumbar spinal stenosis:
a systematic review of randomized controlled trials. Spine (Phila Pa 1976) 2011; 36: E1335-1351
4. Ammendolia C, Stuber K, Tomkins-Lane C, Schneider M,
Rampersaud YR, Furlan AD, et al. What interventions im- prove walking ability in neurogenic claudication with lum- bar spinal stenosis? A systematic review. Eur Spine J 2014;
23: 1282-1301
5. Sengupta DK, Herkowitz HN. Lumbar spinal stenosis.
Treatment strategies and indications for surgery. Orthop Clin North Am 2003; 34: 281-295
6. Meng H, Fei Q, Wang B, Yang Y, Li D, Li J, et al.
Epidural injections with or without steroids in managing chronic low back pain secondary to lumbar spinal stenosis:
a meta-analysis of 13 randomized controlled trials. Drug Des Devel Ther 2015; 9: 4657-4667
7. Friedly JL, Comstock BA, Turner JA, Heagerty PJ, Deyo RA, Sullivan SD, et al. A randomized trial of epidural glu- cocorticoid injections for spinal stenosis. N Engl J Med 2014; 371: 11-21
8. Manchikanti L, Kaye AD, Manchikanti K, Boswell M, Pampati V, Hirsch J. Efficacy of epidural injections in the treatment of lumbar central spinal stenosis: a systematic review. Anesth Pain Med 2015; 5: e23139
9. Manchikanti L, Cash KA, McManus CD, Damron KS, Pampati V, Falco FJ. A randomized, double-blind con- trolled trial of lumbar interlaminar epidural injections in central spinal stenosis: 2-year follow-up. Pain Physician 2015; 18: 79-92
10. Gerdesmeyer L, Wagenpfeil S, Birkenmaier C, Veihelmann A, Hauschild M, Wagner K, et al. Percutaneous epidural lysis of adhesions in chronic lumbar radicular pain: a randomized, double-blind, placebo-controlled trial. Pain Physician 2013; 16: 185-196
11. Gerdesmeyer L, Lampe R, Veihelmann A, Burgkart R, Gobel M, Gollwitzer H, et al. Chronic radiculopathy. Use of minimally invasive percutaneous epidural neurolysis ac- cording to Racz. Schmerz 2005; 19: 285-295
12. Hwang BY, Ko HS, Suh JH, Shin JW, Leem JG, Lee JD.
Clinical experiences of performing transforaminal balloon adhesiolysis in patients with failed back surgery syndrome:
two cases report. Korean J Anesthesiol 2014; 66: 169-172 13. Lee JH, Lee SH. Clinical effectiveness of percutaneous ad- hesiolysis and predictive factors of treatment efficacy in pa- tients with lumbosacral spinal stenosis. Pain Med 2013; 14:
1497-1504
14. Jamison DE, Hsu E, Cohen SP. Epidural adhesiolysis: an evidence-based review. J Neurosurg Sci 2014; 58: 65-76 15. Shin JW. A new approach to neuroplasty. Korean J Pain
2013; 26: 323-326
16. Pauza K, Shapiro M, Calodney A, Bae S, Singh KP.
Treating radiculopathy with an indwelling epidural catheter and infusion pump. Pain Physician 2005; 8: 271-276 17. Nadeau M, Rosas-Arellano MP, Gurr KR, Bailey SI,
Taylor DC, Grewal R, et al. The reliability of differ- entiating neurogenic claudication from vascular claudica- tion based on symptomatic presentation. Can J Surg 2013;
56: 372-377
18. Cappelleri JC, Bushmakin AG, Zlateva G, Sadosky A. Pain responder analysis: use of area under the curve to enhance interpretation of clinical trial results. Pain Pract 2009; 9:
348-353
19. Pratt RK, Fairbank JC, Virr A. The reliability of the Shuttle Walking Test, the Swiss Spinal Stenosis Questionnaire, the Oxford Spinal Stenosis Score, and the Oswestry Disability Index in the assessment of patients with lumbar spinal stenosis. Spine (Phila Pa 1976) 2002; 27: 84-91
20. Copay AG, Glassman SD, Subach BR, Berven S, Schuler TC, Carreon LY. Minimum clinically important difference in lumbar spine surgery patients: a choice of methods using the Oswestry Disability Index, Medical Outcomes Study questionnaire Short Form 36, and pain scales. Spine J 2008;
8: 968-974
21. Hong J, Jung S. Clinical Effectiveness and Prognostic Indicators of Parasagittal Interlaminar Epidural Injection.
Pain Physician 2016; 19: E877-884
22. Park Y, Lee WY, Ahn JK, Nam HS, Lee KH. Percutaneous Adhesiolysis Versus Transforaminal Epidural Steroid Injection for the Treatment of Chronic Radicular Pain Caused by Lumbar Foraminal Spinal Stenosis: A
Retrospective Comparative Study. Ann Rehabil Med 2015;
39: 941-949
23. Scuderi GJ, Brusovanik GV, Anderson DG, Dunham CJ, Vaccaro AR, Demeo RF, et al. Cytokine assay of the epi- dural space lavage in patients with lumbar intervertebral disk herniation and radiculopathy. J Spinal Disord Tech 2006; 19: 266-269
24. Ture H, Eti Z, Gogus FY, Duzgun O, Mutlu Z, Karabagli P. Histopathological effects on epidural tissue of bolus or continuous infusions through an epidural catheter in ewes.
Anaesthesia 2010; 65: 473-477
25. Mowat I, Tang R, Vaghadia H, Krebs C, Henderson WR, Sawka A. Epidural distribution of dye administered via an epidural catheter in a porcine model. Br J Anaesth 2016;
116: 277-281
26. Goeller JK, Joselyn A, Martin DP, Bhalla T, Dairo O, Herz DB, et al. Epidural pressure changes following caudal blockade: a prospective, observational study. J Anesth 2016; 30: 578-582
27. Balga I, Gerber H, Schorno XH, Aebersold Keller F, Oehen HP. Bupivacaine crystal deposits after long-term epidural infusion. Anaesthesist 2013; 62: 543-548
28. Sbardelotto C, Yoshimi MM, Pereira Rda R, de Castro RA.
Breakage of a catheter in the epidural space. Rev Bras Anestesiol 2008; 58: 643-650