Clinical crown lengthening procedure with forced eruption and fi berotomy
6
0
0
전체 글
(2) Clinical crown lengthening procedure with forced eruption and fiberotomy. 치관연장술에 대한 대안으로 사용되거나 일벽성 또는 이벽성. 값으로 표현하였으며, 잔존치질의 양은 치은변연을 기준으로. 골내낭을 가진 치아의 골결손부 감소 및 제거를 위해 사용될. 하여 치은연상에 있을 경우 양의 값, 치은연하에 있을 경우 음. 수 있다. Ingber (1976)는 맹출에 필요한 힘과 시간, 유지 후 외. 의 값으로 표현하였다. 측정값은 치료대상 치아의 협측과 설. 과적 치관연장술 등의 방법을 보고하였으며, Simon 등(1978). 측 근심, 중앙, 원심 3부위에서 측정하였으며 근심부터 원심으. 은 근관치료의 목적으로 강제 맹출술을 보고하였다.. 로의 순서로 기록하였다. 환자의 치주낭 깊이는 협설측에서. 또한 Pontoriero 등(1987)은 강제 맹출술에 치은섬유절단술. 각각 2/2/2 mm, 2/2/2 mm로 측정되었으며, 잔존치질의 양은. (fiberotomy)의 필요성에 대하여 보고하였다. 이 술식은 치아. 협설측에서 각각 0/−1/−1 mm, 1/1/0 mm로 측정되었다. 치아. 주변의 치은섬유를 수술도를 이용하여 절단시켜주는 술식으. 의 동요는 관찰되지 않았다. 상악 좌측 중절치의 치관-치근 파. 로, 치아를 강제적으로 맹출시키면 치은섬유와 치주인대섬유. 절 진단 하에 강제 맹출술을 동반한 임상치관연장술을 계획. 가 장력을 받게 되는데 치아의 정출을 억제하는 치은섬유를. 하였다.. 절단시킴으로써 치아의 이동을 빠르게 하고 정출된 치아가 제 자리로 돌아가려는 것을 억제시키는 효과가 있다.. 모형 상에서 장치를 제작하였으며, 와이어는 충분히 강성 (rigidity)이 있고, 조작이 용이하며, 정출과정 중 두드러지는. 이번 증례에서 소개한 강제 맹출술은 적절한 수복물을 위치. 휨 현상이 없게 하기 위하여 0.036 inch round orthodontic wire. 시키기 위해 상피부착부 상방으로 파절선을 노출시키기 위한. 나 다가닥 와이어(multi stranded wire)가 주로 사용되는데, 이. 술식이며, 비교적 덜 침습적이고, 두드러지는 골개조 현상 없. 번 증례에서는 다가닥 와이어를 사용하였다. 와이어는 근관. 이 치주인대 섬유의 신장에 의해 정출이 이루어지는 급속교. 위를 통과하게 하여 협설측으로의 경사이동(tilting)이 발생. 정적 치료방법 중 하나이다. 임상치관연장이 필요한 경우, 치. 하지 않도록 하였다. 또한 와이어를 절단연 방향에 최대한 가. 아와 함께 치은 및 치조골이 이동함에 따라 외형적인 치관길. 깝게 제작하고 hook를 가능한 치근 방향으로 가깝게 부착하. 이의 증가가 없는 경우도 있으며, 이런 경우에만 2차적인 수술. 여, 와이어와 hook 사이에 수직적으로 충분한 공간이 형성되. 을 통해 치은과 치조골을 필요한 만큼만 제거하여 인접치와. 도록 하였다. 정출에 사용하는 견인장치로는 chain elastic이. 조화되는 치은, 치조골의 높이를 얻을 수 있게 된다. 그러므로. 나 elastic thread가 주로 사용되는데, 이번 증례에서는 elastic. 이 방법은 강제 맹출술을 동반하지 않은 임상치관연장술에. thread를 사용하였다(Fig. 1B).. 비하여 삭제하는 골의 양이 적고 치간유두를 보존할 수 있기. 구강 내 장치를 장착하고 장치장착기간동안 심미적 불편감 을 방지하기 위해 순면에 레진 의치를 부착하였다(Fig. 1C). 2. 때문에 더 심미적이다. 이는 임플란트와 비교하였을 때에도 마찬가지로, 심미적 치. 주 간격으로 elastic thread를 교체하고 치은섬유절단술을 시. 료가 어려운 전치부 임플란트에 비해 비교적 쉽게 심미적인. 행하면서 2개월 동안 견인을 시행하였다. 장치를 장착하고 2. 결과를 얻을 수 있을 뿐만 아니라 자연치아가 갖는 치주인대. 개월 경과 후의 모습에서 치아의 정출과 함께 치은이 치관 쪽. 의 완충능력과 고유수용성 감각기능을 유지할 수 있기 때문. 으로 이동된 모습을 관찰할 수 있으며 방사선사진을 통해서. 에 부가적인 장점을 갖는다.. 도 치아의 정출을 확인할 수 있었다(Fig. 1D, E). 약 8주의 유지. 이에 저자들은 조선대학교 치과병원 치주과에서 치관 파절 또는 치관-치근 파절로 진단된 3명의 환자에서 각각의 진단 및 치료과정에 대한 고찰과 함께 술 후 경과에 대한 증례들을 보고하고자 하는 바이다.. 기간 후 골 삭제술을 동반하지 않은 치은절제술을 통하여 임 상치관연장술을 시행하였다(Fig. 1F). 임상치관연장술 시행 후 치주낭 깊이는 협설측에서 각각 2/2/2 mm, 2/2/2 mm로 치료 전과 비교하여 큰 변화가 없었으 며, 잔존치질의 양은 협설측에서 각각 2/1/1 mm, 2/2/2 mm로. 증례보고 증례 1 21세 여성 환자로 상악 좌측 중절치의 파절을 주소로 내원 하였으며 임상검사 및 방사선사진을 통하여 파절선이 치은연 하로 연장되어 있는 치관-치근 파절임을 확인하였다(Fig. 1A).. 치료 전과 비교하여 보철수복에 적절한 양의 잔존치질을 확 보하였다(Fig. 1G). 이후 임시보철물과 최종보철물을 제작 및 장착하였으며, 최종보철 장착 후 심미적으로 큰 문제없이 양 호한 결과를 얻을 수 있었다(Fig. 1H).. 증례 2. 치료의 평가를 위해 치료대상 치아의 치주낭의 깊이 및 임상. 54세 여성 환자로 상악 좌측 견치의 동요를 주소로 내원하. 치관의 길이를 치료 전후에 측정하였다. 치주낭 깊이는 잔존. 였으며 임상검사 및 방사선사진을 통하여 상부 보철물의 변. 치질의 변연을 기준으로 치주낭 기저부까지의 거리를 측정한. 연 부적합을 확인하였다(Fig. 2A). 치주낭 깊이는 협설측에서. 64.
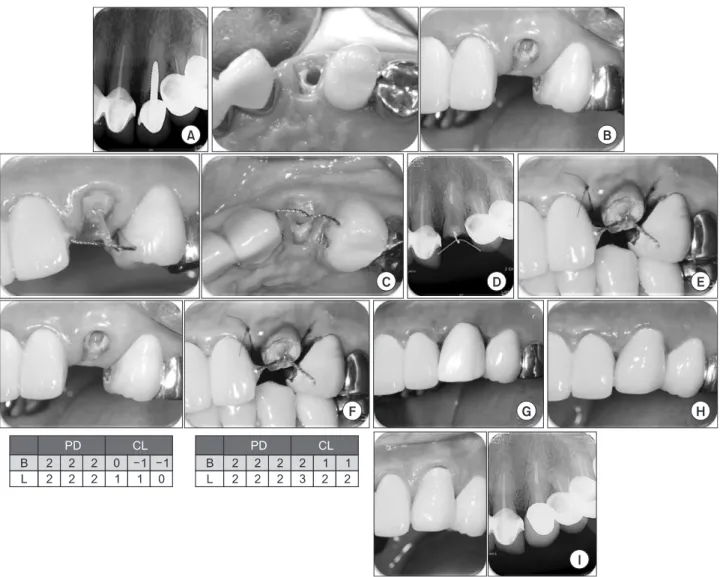
(3) Keon-Il Yang et al.. Fig. 1. (A) Showing crown-root fracture of #21 on radiograph at the first visit. (B) Intra-oral appliance delivery. (C) Resin denture was attached on buccal side to prevent esthetic inconvenience during the setting time. (D) Radiograph taken 2 months after forced eruption showing extrusion of the tooth. (E) Clinical photo 2 months after forced eruption. (F) Clinical photo after clinical crown lengthening. Proper amount of tooth was obtained through gingivectomy without bone removal. (G) Comparison of the appearance before and after the treatment. Compared to the appearance before the treatment, about 2 mm of tooth was extruded and the amount of tooth enough for prosthodontic restoration was obtained in supra-gingival area after the treatment. PD: pocket depth, CL: crown length. (H) The final prosthodontics after the treatment.. 각각 2/2/2 mm, 2/2/2 mm로 측정되었으며, 잔존치질의 양은. 2/2/2 mm, 2/2/2 mm로 치료 전과 비교하여 큰 변화가 없었으. 협설측에서 각각 −1/−1/−1mm, 0/0/−1 mm로 측정되었다. 치. 며, 잔존치질의 양은 협설측에서 각각 2/2/2 mm, 3/3/2 mm 로. 아의 동요는 관찰되지 않았다(Fig. 2B). 상악 좌측 견치의 상부. 치료 전과 비교하여 보철수복에 적절한 양의 잔존치질을 확. 보철물의 변연 부적합 진단 하에 근관치료와 함께 강제 맹출. 보하였다(Fig. 2F). 임시보철물을 통하여 치은조직의 치유를. 술을 동반한 임상치관연장술을 계획하였다. 위 증례와 동일한 방법으로 모형상에서 장치를 제작하였으 며 구강 내 장치를 장착하였다(Fig. 2C). 2주 간격으로 elastic thread를 교체하고 치은섬유절단술을 시행하면서 2개월 동 안 견인을 시행하였다. 2개월 경과 후의 모습에서 치아의 정출. 도모하였으며 이후 최종보철물을 장착하였다(Fig. 2G, H). 약 1년 후의 임상검사에서 약간의 치은퇴축을 제외하고 특별한 이상소견은 관찰되지 않았다(Fig. 2I).. 증례 3. 과 함께 치은이 치관 쪽으로 이동된 모습을 관찰할 수 있으며. 40세 여성 환자로 상악 우측 중절치의 파절을 주소로 내원. 방사선사진을 통해서도 치아의 정출을 확인할 수 있었다(Fig.. 하였으며 임상검사 및 방사선사진을 통하여 상악 우측 중절. 2D, E). 약 8주의 유지기간 후 골삭제를 동반하지 않은 치은절. 치 치관파절을 확인하였다(Fig. 3A). 치주낭 깊이는 협설측에. 제술을 통하여 임상치관연장술을 시행하였다. 임상치관연장술 시행 후 치주낭 깊이는 협설측에서 각각. 서 각각 2/2/2 mm, 2/2/2 mm로 측정되었으며, 잔존치질의 양 은 협설측에서 각각 1/2/1 mm, 0/0/0 mm로 측정되었다. 치아. 65.
(4) Clinical crown lengthening procedure with forced eruption and fiberotomy. Fig. 2. (A) Radiograph at the first visit showing radiolucent gap between the upper prosthodontics and root rest of #22 tooth. (B) Clinical photo after the removal of the upper prosthodontics. The margin of the residual tooth is observed at infra-gingival area. (C) Intra-oral appliance delivery. (D) Radiograph showing extrusion 2 months after the forced eruption. (E) Clinical photo taken 2 months after the forced erupiton. (F) Comparison of the appearance before and after the treatment. Compared to the appearance before the treatment, about 2 mm of tooth was extruded and the proper amount of tooth enough for prosthodontic restoration was obtained at supra-gingival area. PD: pocket depth, CL: crown length. (G) Temporary prosthodontics set for healing of gingiva. (H) Appearance showing the final prosthodontics after the treatment. (I) Clinical photo and radiograph one year after the final prosthodontics. Gingival recession on labial side is observed.. 의 동요는 관찰되지 않았다(Fig. 3B). 상악 우측 중절치의 치관 파절 진단 하에 근관치료와 함께 강제 맹출술을 동반한 임상 치관연장술을 계획하였다.. 여 임상치관연장술을 시행하였다(Fig. 3F). 임상치관연장술 시행 후 치주낭 깊이는 협설측에서 각각 2/2/2 mm, 2/2/2 mm로 치료 전과 비교하여 큰 변화가 없었으. 위 두 증례와 동일한 방법으로 모형 상에서 장치를 제작하. 며, 잔존치질의 양은 협설측에서 각각 3/4/3 mm, 2/2/2 mm로. 고 구강 내 장치를 장착하였다(Fig. 3C). 2주 간격으로 elastic. 치료 전과 비교하여 보철수복에 적절한 양의 잔존치질을 확. thread를 교체하고 치은섬유절단술을 시행하면서 2개월 동안. 보하였다(Fig. 3G). 이후 최종보철물을 제작 및 장착하였으며. 견인을 시행하였다. 1개월 경과 후의 임상검사 및 방사선사진. 보철수복 후 심미적으로 만족스러운 결과를 얻을 수 있었다. 에서 정출된 양상을 확인할 수 있었으며 2개월 경과 후 보철수. (Fig. 3H).. 복을 위한 충분한 양의 치질이 확보되었다(Fig. 3D, E). 8주 간 의 유지기간 후 골삭제를 동반하지 않은 치은절제술을 통하. 66.
(5) Keon-Il Yang et al.. Fig. 3. (A) Radiograph at the first visit. Crown fracture of #11 is observed. (B) Clinical photo after the completion of endodontic treatment. About 0-1 mm of residual tooth is observed. (C) Intra-oral appliance delivery. (D) Radiograph and clinical photo taken one month after the forced eruption. Extrusion of tooth is observed. (E) Clinical photo 2 months after the forced eruption. (F) After the clinical crown lengthening. Enough tooth was obtained through gingivectomy without bone removal. (G) Comparison of the appearance before and after the treatment. Compared to the appearance before the treatment, about 2 mm of tooth was extruded and proper amount of tooth enough for prosthodontic restoration was obtained at supra-gingival area. PD: pocket depth, CL: crown length. (H) The final prosthodontics after the treatment.. 고. 찰. 강제 맹출술은 교정적 치료방법으로서 힘, 시간, 치은섬유 절단술, 심미적 문제, 유지기간 등을 고려해야 한다. 정출에 필. 치은하방으로 파절선이 연장된 경우에 심미적, 생물학적,. 요한 적절한 힘을 Cooke과 Scheer (1980)는 70-150 g이라 하. 수복적 문제를 고려해야 하며 치료방법을 선택하는 데 있어. 였고 Wang과 Wang (1992)은 20-30 g, Bondemark 등(1997). 서 남아있는 치관의 양, 파절선에서 치조정까지의 거리, 환자. 은 30-60 g이라고 보고하였다. 정출에 필요한 시간은 Ingber. 의 심미적인 요구조건 등을 고려해야 하는데, 강제 맹출술은. (1976)는 2주에 1 mm, Wang 등(1992)은 2주에 3-4 mm, Proffit. 심미적인 외형을 수복하는 데 있어 위험성이 낮은 적절한 치. 등(2000)은 1주에 1 mm 정도가 적당하다고 하였다.. 료방법이라 할 수 있다(Koyuturk & Malkoc, 2005).. Simon (1984)은 정출과정에 있어 골과 연조직의 상방이동. 67.
(6) Clinical crown lengthening procedure with forced eruption and fiberotomy. 의 최소화, 치료 후 재발의 방지와 유지기간의 감소를 위해 치 은섬유절단술의 필요성을 보고하였다. Reitan (1969)은 치주 인대가 신장된 상태로 3-5개월 가량 지속되기 때문에 재발의 위험을 최소화하고 유지 기간을 단축시키기 위해 치은섬유절 단술이 필요하다고 보고하였다. 강제 맹출술은 치은절제술 등의 외과적 술식을 단일치아 로 한정할 수 있게 하므로 심미적인 면에서 유리하다고 할 수 있다(Ingber, 1989). 치료 후 유지기간은 다양하게 보고되었으 나 대략 7-14주의 유지기간이 필요하며 다른 일반적인 교정치 료에 비해 재발이 적다고 보고되었다(Andreasen et al., 1989; Heithersay, 1973; Ingber, 1976; Simon et al., 1978; Zyskind et al., 1992). 그 밖에 강제 맹출술을 시행하기 위해서는 최소 14 mm의 치아길이가 있는 것이 유리하며 이는 치근단 폐쇄를 위한 4 mm의 Gutta percha cone 길이, post를 위한 10 mm의 길이이 다. 치주조직의 지지를 유지하기 위해 최소 1 : 1의 치관 치근 비율이 필요하며 파절선에서 치근단까지 12 mm 이하인 경우 에는 그 예후가 불량하다고 할 수 있다(Lovdahl, 1995). 이 논문에서 살펴본 3개의 증례 모두 보철물을 수복하기 위 한 잔존 치질이 부족한 상태였으며 강제 맹출술을 통하여 치 아를 정출시킴으로써 골삭제술 없이 보철수복에 충분한 양의 치질을 확보하였다. 수술 후 치아동요도 증가와 같은 술 후 합 병증은 발견되지 않았으며 치관 치근비율 1 : 1로 강제 맹출술 에 적절한 적응증이었다. 술 후 추적관찰에서 증례 2의 경우 1 년 후 약간의 치은퇴축 소견이 관찰되었으나 이외의 치주적 인 문제는 발견되지 않았으며 증례 1과 3의 경우는 술 후 합병 증 없이 심미적으로 잘 유지되었다. 결론적으로, 치은 하방으로 연장된 치아의 파절을 수복하기 위한 강제 맹출술을 동반한 임상치관연장술은 좋은 치료방법 으로 이는 환자가 쉽게 받아들일 수 있는 간단하며 안전한 술 식이다.. 참고문헌 Andreasen G, Margeas R, Green K, Nowak A, Lainson P, Dembo J: A multidisciplinary approach for optimal total patient care: a case report. Quintessence Int 20:295-297, 1989. Bondemark L, Kurol J, Hallonsten AL, Andreasen JO: Attractive magnets for orthodontic extrusion of crown-root fractured teeth. Am J Orthod Dentofacial Orthop 112:187-193, 1997. Cooke MS, Scheer B: Extrusion of fractured teeth. The evolution of practical clinical techniques. Br Dent J 149:50-53, 1980. de Waal H, Castellucci G: The importance of restorative margin placement to the biologic width and periodontal health. Part. 68. II. Int J Periodontics Restorative Dent 14:70-83, 1994. Fugazzotto PA, Parma-Benfenati S: Preprosthetic periodontal considerations. Crown length and biologic width. Quintessence Int Dent Dig 15:1247-1256, 1984. Gargiulo A, Wentz F, Orban F: Dimensions and relations of the dentogingival junction in humans. J Periodontol 32:261, 1961. Heithersay GS: Combined endodontic-orthodontic treatment of transverse root fractures in the region of the alveolar crest. Oral Surg Oral Med Oral Pathol 36:404-415, 1973. Ingber JS: Forced eruption: part II. A method of treating nonrestorable teeth-Periodontal and restorative considerations. J Periodontol 47:203-216, 1976. Ingber JS: Forced eruption: alteration of soft tissue cosmetic deformities. Int J Periodontics Restorative Dent 9:416-425, 1989. Koyuturk AE, Malkoc S: Orthodontic extrusion of subgingivally fractured incisor before restoration. A case report: 3-years follow-up. Dent Traumatol 21:174-178, 2005. Lovdahl PE: Periodontal management and root extrusion of traumatized teeth. Dent Clin North Am 39:169-179, 1995. Nevins M, Skurow HM: The intracrevicular restorative margin, the biologic width, and the maintenance of the gingival margin. Int J Periodontics Restorative Dent 4:30-49, 1984. Pontoriero R, Celenza F Jr, Ricci G, Carnevale G: Rapid extrusion with fiber resection: a combined orthodontic-periodontic treatment modality. Int J Periodontics Restorative Dent 7:3043, 1987. Proffit WR, Fields HW, Sarver DM: Contemporary orthodontics. 4th ed. Mosby Elsevier, St. Louis, pp.645, 2000. Reitan K: Principles of retention and avoidance of posttreatment relapse. Am J Orthod 55:776-790, 1969. Simon JH, Kelly WH, Gordon DG, Ericksen GW: Extrusion of endodontically treated teeth. J Am Dent Assoc 97:17-23, 1978. Simon JH: Root extrusion. Rationale and techniques. Dent Clin North Am 28:909-921, 1984. Tal H, Soldinger M, Dreiangel A, Pitaru S: Periodontal response to long-term abuse of the gingival attachment by supracrestal amalgam restorations. J Clin Periodontol 16:654-659, 1989. Vacek JS, Gher ME, Assad DA, Richardson AC, Giambarresi LI: The dimensions of the human dentogingival junction. Int J Periodontics Restorative Dent 14:154-165, 1994. Wagenberg BD: Surgical tooth lengthening: biologic variables and esthetic concerns. J Esthet Dent 10:30-36, 1998. Wang Z, Heffernan M, Vann WF Jr: Management of a complicated crown-root fracture in a young permanent incisor using intentional replantation. Dent Traumatol 24:100-103, 2008. Wang WG, Wang WN: Forced eruption: an alternative to extraction or periodontal surgery. J Clin Orthod 26:146-149, 1992. Zyskind K, Zyskind D, Soskolne WA, Harary D: Orthodontic forced eruption: case report of an alternative treatment for subgingivally fractured young permanent incisors. Quintessence Int 23:393-399, 1992..
(7)
수치
관련 문서
3. In case of gold alloy inner crown, gold alloy outer crown was better than GES outer crown in retentive force. However, retentive force of gold alloy outer
As the number of clinical cases requiring supracrestal apical-coronal positioning is increasing, we examined the utility of FEA in such cases. In this study,
:Acidulated phosphate fluoride treatment and formation of caries-like lesions in enamel: effect of application time.. Schmidt HF : The fluoride varnish
When it comes to Arbitration which is a useful way to resolve the international investment disputes, the Civil procedure for Recognition and Enforcement of Foreign Judgement
Diagrams show the spatial distribution of individual trees and stand profile(a), crown projection(b) for Group of Quercus glauca... The comparison of
The clinical outcome and complication for treating proximal femoral shaft fracture were compared and analyzed through the group treated with closed
19) Yu Y, Kang J., Clinical studies on treatment of chronic prostatitis with acupuncture
The key procedure of seismic design is consisted of decision of design earthquake, dynamic seismic response analysis, seismic design of structures and equipment,
