Original Article
pISSN 2233-9019 · eISSN 2233-9116
Korean J Fam Pract. 2015;5(3, suppl. 2):912-916
KJFP
Korean Journal of Family Practice서 론
2014 년 발표된 통계청 자료에 따르면 심혈관 질환은 2013 년 우리 나라 남녀 사망원인 순위의 3 대 사인(암, 심장 질환, 뇌혈관 질환) 중 하나로 주요 사망원인 중 하나이며,
1)급성기 회복 후 사회로의 복귀 나 회복 후에도 지속적 관리 대상이 되어 의료 자원 소요를 요하며, 가정이나 사회적으로 중요한 역할을 담당하는 연령에서 발병이 많 아 사회·경제적 측면에서의 손실 역시 간과할 수 없다. 심혈관 질환 진단에서 침습적 관상동맥 조영술이 표준 검사법이나, 최근 급속히 발달한 전 산화 단층 촬영 기술로 인해 관상동맥 전산화 단층 촬영 혈관 조영술( coronary computed tomogr - aphy angiography , 이하 CCTA 로 지칭)로 심혈관 상태를 평가할 수 있다. CCTA 로 관상동
맥 협착을 평가에 하는데 있어 민감도와 음성 예측도가 90 % 이상으 로 매우 높고, 과거 16 -절편 다중 절편 나선식 CT ( Multi detector - row spiral CT , 이하 MDCT 로 약함)를 이용한 연구 결과의 기술적 인 한계 때문에 평가가 불가능하였던 사례가 있었으나, 최근 도입된 64 -절편 MDCT 를 이용 한 연구에서는 높은 심박동수를 가진 환자 와 1 . 5mm 이하의 작은 관상동맥을 분석대상에 포함하고도 90 % 이 상의 민감도, 특이도, 음성 예측도를 보고하고 있다.
2-7)심혈관 질환의 위험인자로는 연령, 흡연, 고혈압, 당뇨, 가족력, 이상지질혈증, 비만 등이 있다.
8)비만과 심혈관 질환과의 관련성 은 과거 비만 환자들에 대한 임상적 관찰과 심혈관계 질환 발생 환 자, 혹은 이로 인한 사망자를 포함한 인구 집단을 대상으로 한 역학 적 연구들에 의해서 밝혀졌으며, 아울러 비만 교정을 통해 심혈관
심혈관 관상동맥 이상과 비만지표 최적 변별점
유명진, 김상혁
*, 장영근, 신원영, 한정완, 이우택
효성병원 가정의학과
Optimal cut off points for obesity indices to predict coronary vascular abnormality.
Myoung-Jin Yoo, Sang Hyuck Kim
*, Young-Keun Jang, Won-Young Shin, Jeong-Wan Han, Woo-Taek Lee
Department of Family Medicine, Hyosung Hospital, Cheong-ju, KoreaBackground: Coronary computed tomography angiography is a useful tool for evaluation of coronary vasculature. This study was designed in order to estimate optimal obesity indices to predict coronary vascular abnormality by receiver-operating characteristic curves.
Methods: We selected people who visited Hyosung hospital and received coronary computed tomography angiography between 2012 and 2013 and identified cardiovascular abnormality according to the results. We estimated the optimal anthropometrical cut-off points of body mass index, waist circumference, and waist-to-height ratio using receiver operating characteristic curves and Area Under the Curves.
Results: The Area Under the Curves of waist-to-height ratio was highest, followed by waist circumferencence and body mass index in turn. Anthropometric cut-off points in males and females were identified as a body mass index of 23.0kg/m
2, 20.2kg/m², respectively, and waist circumference of 80cm and 82cm, respectively. In terms of waist-to-height ratio, the value was 0.46, 0.50 in males and females, respectively.
Conclusion: As in previous studies that predicted risk of cardiovascular disease, this study also shows thaat waist-to-height ratio is more associated with cardiovascular abnormalities than other obesity indices, such as BMI or waist circumference. Thus, more extensive trials of clinical diagnostic tools for obese people using waist-to-height ratio should be performed. In addition, lower optimal values of obesity indices should be considered for use.
Keywords: Coronary computed tomography angiography, obesity indices, receiver operating characteristic curves
Received February 27, 2015 Revised July 27, 2015 Accepted September 23, 2015 Corresponding Author Sang Hyuck Kim
Tel: +82-43-221-5000 E-mail: [email protected]
Copyright © 2015 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
유명진 외. 심혈관 관상동맥 이상과 비만지표 최적 변별점 Korean Journal of Family Practice
KJFP
Original Article
Korean Journal of Family Practice
질환 발생을 줄일 수 있다.
9, 10)비만의 진단과 평가는 체중( kg )을 신 장( m
2)의 제곱으로 나눈 값인 체질량지수( Body mass index , kg / m
2), 체성분 분석을 이용한 체지방량( Body fat mass , %)등이 있으 며, 복부비만 정도를 측정하는 신체 계측 지표로 허리둘레( Waist circumference ), 허리둘레-키 비( Waist - to - height ratio )등이 있 다.
11)본 연구에서는 진단된 심혈관 질환 이환자가 아닌 정상인을 대 상으로 신체 계측 시행 후 얻은 비만 관련 지표와 검진 시 촬영한 CCTA 결과를 분석해 적정 체질량지수, 허리둘레 수치, 허리둘레- 키 비를 추정 하고자 한다.
연구방법
1. 자료 출처 및 변수
2012 년 01 월 01 일 부터 2013 년 12 월 31 일 기간 동안 청주 지 역 일개 종합병원에 내원해 건강 검진을 받았던 수검자 총 63652 명 중 CCTA 검사를 받았던 자 762 명을 연구대상으로 선정했으 며, 대상자의 의무기록 확인을 통해 본 연구에 필요한 정보를 조사 하였다. CCTA 는 128 - Slice - MDCT ( optima 660 mode , General Electronics . USA )로 행해졌다. 이렇게 획득한 영상정보는 임상 정 보 없이 영상의학과 전문의에게 배정, 분석되어 판독된 자료를 사 용했다.
대상자의 기본적 특성으로 연령, 신장, 체중, 허리둘레, 고혈압, 당뇨, 흡연, 공복 혈당수치, 총 콜레스테롤 수치, 중성지방 수치, 고 밀도 지단백 수치, 저밀도 지단백 수치를 조사하였다. 고혈압은 기 존에 고혈압 진단을 받았거나, 측정 당시 수축기 혈압이 140mmHg 이상 또는 이완기 혈압이 90mmHg 이상인 경우로 분류했다. 당뇨 환자는 기존 당뇨 진단 기왕력이 있거나, 검진에서 시행한 공복혈 당 수치가 126mg / dL 이상인 사람으로 했다. 흡연유무는 설문 조사 를 대상으로 비흡연자, 과거 흡연자, 현재 흡연자로 구분하여 현재 흡연자만을 흡연군으로 분류하였다. 연구대상으로 선정한 762 명 중 의무기록 상 키, 체중, 허리둘레 등이 명시되지 않아 이를 알 수 없 었던 25 명을 제외했고, 기존 심장질환으로 심혈관 관상동맥 시술 기왕력자 4 명을(의무기록 상에는 심장질환이 표기되어 있지 않으 나, CCTA 상 심혈관 관상동맥 스텐트 삽입이 확인된 1 명 포함) 제 외했다. 아울러, CCTA 상 관상동맥 평가 시 움직임 등에 의한 인공 물( motion artifact ) 발생으로 인해 정확한 협착 정도 평가가 이루어 지지 못했던 57 명( CCTA 촬영은 하였으나, 자료가 누락되어 결과 를 알 수 없었던 2 명 포함) 역시 본 연구에서 제외해, 상기 기간 조 사대상자 762 명 중 676 명만을 선별하여 연구하였다.
2. 통계 분석 및 방법
분석을 위해 통계 프로그램 Stata 12 . 0 ( STATA corp . LP )을 통해 본 연구를 시행했고, 유의수준은 P value
<0 . 05 로 정하였다. CCTA 결과에 따른 체질량지수, 허리둘레, 허리둘레-키 비의 ROC 곡선 ( recei - ver operating characteristic curve , 이하 ROC )을 통해 구한 후 각 신체 계측치의 최적 변별점 추정을 위해 Youden index 를 이 용했다. Youden index 는 민감도와 특이도의 합에서 1 을 차감한 값 이고, 최적 변별점은 Youden index 값이 최대가 되는 지점으로 정
하였다.
12, 13)연구결과
1. 대상자의 일반적 특성
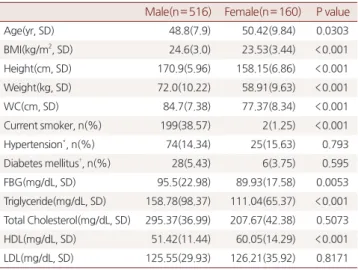
남자 516 명, 여자 160 명으로 총 676 명이 본 연구의 대상이었 고, 평균연령은 남자 48 . 8 세, 여자 50 . 4 세로 차이가 있었으며,( P value 0 . 030 ) 체질량지수는 남자 24 . 6kg / m
2, 여자 23 . 5kg / m
2, 평균 키는 남자 170 . 9cm , 여자 158 . 2cm , 평균체중은 남자 72 . 0kg , 여 자 58 . 9kg , 허리둘레의 경우 남자 84 . 7cm , 여자 77 . 4cm 로 남자에 서 더 높았다. ( P
<0 . 001 ) 현재 흡연 인구는 남자 38 . 6 %, 여자 2 % 로 남자 흡연자 비율이 훨씬 높았다. ( P
<0 . 001 ) 고혈압 환자는 남 자에서 14 . 3 %, 여자 15 . 6 %로 차이가 없었으며( P value 0 . 793 ), 당뇨의 경우 역시 남자에서 5 . 4 %, 여자 3 . 8 %로 차이를 보이지 않 았다. ( P value 0 . 595 ) 혈액 검사의 경우 남녀 각각 공복 혈당수치 95 . 5mg / dL , 89 . 9mg / dL 로 남자에서 더 높았고, ( P value 0 . 005 ), 중성 지방 수치는 남자 158 . 8mg / dL , 여자 111 . 0mg / dL 로 남자에 서 더 높았고, ( P
<0 . 001 ) 고밀도 지단백 수치는 남자 51 . 4mg / dL ,
Table 1. Baseline characteristics by study groups
Male(n= 516) Female(n= 160) P value
Age(yr, SD) 48.8(7.9) 50.42(9.84) 0.0303
BMI(kg/m2, SD) 24.6(3.0) 23.53(3.44) <0.001 Height(cm, SD) 170.9(5.96) 158.15(6.86) <0.001 Weight(kg, SD) 72.0(10.22) 58.91(9.63) <0.001
WC(cm, SD) 84.7(7.38) 77.37(8.34) <0.001
Current smoker, n(%) 199(38.57) 2(1.25) <0.001
Hypertension*, n(%) 74(14.34) 25(15.63) 0.793
Diabetes mellitus†, n(%) 28(5.43) 6(3.75) 0.595
FBG(mg/dL, SD) 95.5(22.98) 89.93(17.58) 0.0053
Triglyceride(mg/dL, SD) 158.78(98.37) 111.04(65.37) <0.001 Total Cholesterol(mg/dL, SD) 295.37(36.99) 207.67(42.38) 0.5073 HDL(mg/dL, SD) 51.42(11.44) 60.05(14.29) <0.001 LDL(mg/dL, SD) 125.55(29.93) 126.21(35.92) 0.8171
* Taking antihypertensive drugs or Blood pressure is above 140/90 mmHg
† Taking drugs for diabetes or fasting blood sugar(FBS)≥126mg/dL
Myoung-Jin Yoo, et al. Optimal cut off points for obesity indices to predict coronary vascular abnormality.
Korean Journal of Family Practice
KJFP
여자 60 . 1mg / dL 로 여자에서 더 높았다. ( P
<0 . 001 ) total cholesterol 및 저밀도 지단백 수치는 남녀 각각 295 . 4mg / dL , 207 . 7mg / dL , 125 . 6mg / dL , 126 . 2mg / dL 로 차이가 없었다. (각각 P value 0 . 507 , 0 . 817 ) ( Table 1 )
2. 관상동맥 조영 전산화 단층 촬영결과에 따른 신체 계측치의 분포 JACC ( Journal of The American College of Cardiology ) 발행된 자료를 참고 관상동맥 협착 정도를 CCTA 결과에 따라 6 단계로
14)나눈 후 심혈관 이상 유무에 따라 참고하여 두 군으로 분류하였다.
( Table 2 , Table 3 )
3. 신체 계측치별 위험도 예측 및 최적 변별점
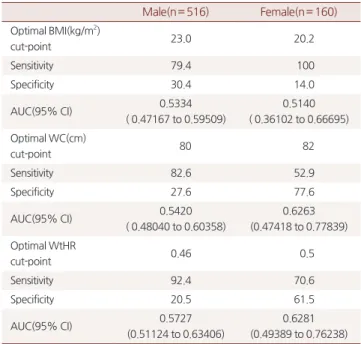
ROC 곡선을 이용하여 심장 관상동맥 이상 유무 예측 목적으로 체질량지수, 허리둘레, 허리둘레-키 비의 예측 정도를 평가하였고, 최적 변별점을 추정하였다. 남녀 모두에서 예측 정도는 AUC ( area under the curve , 이하 AUC 지칭)가 허리둘레-키 비, 허리둘레, 체질량지수 순으로 각각의 수치는 남자 0 . 5727 , 0 . 5420 , 0 . 5334 , 여 자 0 . 6281 , 0 . 6263 , 0 . 5140 로 관찰되었다. ( Figure 1 , 2 )
체질량지수의 최적 변별점은 남자에서 23 . 0kg / m
2(민감도 79 . 4 %, 특이도 30 . 4 %), 여자에서 20 . 2kg / m
2(민감도 100 %, 특이도 14 . 0 %)였고, 허리둘레의 경우 남자에서 80cm (민감도 82 . 6 %, 특이 도 27 . 6 %), 여자에서 82cm (민감도 52 . 9 %, 특이도 77 . 6 %)였으며, 허리둘레-키 비의 경우에는 남자에서 0 . 46 (민감도 92 . 4 %, 특이도 20 . 5 %), 여자에서 0 . 5 (민감도 70 . 6 %, 특이도 61 . 5 %)였다. ( Table 4 ) 고 찰
아시아인이 백인에 비해 같은 체질량지수에서도 더 높은 체지방 률을 갖거나,
15-17)더 낮은 체질량 지수에서 비만 관련 질환 위험성 이 높다는 연구가 발표되었다.
15, 18-21)허리둘레-키 비는 심혈관 질 환 위험인자들을 예측할 수 있는 복부비만의 지표로서 권 등
22)은 성인 남자에서 허리둘레-키 비가 0 . 5 이상인 군에서 고혈당, 이상 지질혈증 등의 발병이 더 높게 나타남을 보고하였고, Park 등
23)은 2005 년 국민건강영양조사 자료를 이용하여 한국성인에서 심혈관
Table 2. Distribution of participants by CCTA scoreCCTA Male
(n= 516) % Female
(n= 160) % total (n= 676) %
0(normal)* 424 82.2 143 89.4 567 83.9
1(minimal)† 26 5 6 3.8 32 4.7
2(mild)‡ 48 9.3 10 6.3 58 8.6
3(moderate)§ 10 1.9 1 0.6 11 1.6
4(severe)|| 6 1.2 0 0 6 0.9
5(occluded) 2 0.4 0 0 2 0.3
Normal*: Absence of plaque and no luminal stenosis Miniaml†: Plaque with<25% stenosis
Mild‡: 25%~49% stenosis Moderate§: 50%~69% stenosis, Severe||: 70%~99% stenosis
Table 3. Distribution of participants by coronary vascular abnomality*, sex
coronary vasculature
male (n= 516)
female (n= 160)
total (n= 676)
normal 424 143 567
abnormal 92 17 109
* We distributed participants two groups as normal group that have no coronary abnomality & abnormal group have any obstructive lesion by CCTA result.
Figure 1. ROC curve of anthropometric indices and their area under the curve(AUC) for male
predicting coronary vascular abnormality.
BMI*: Body Mass Index.
WC†: Waist Circumference.
WtHR‡: Waist-to- Height Ratio.
Figure 2. ROC curve of anthropometric indices and their area under the curve(AUC) for fema
-le predicting coronary vascular abnormality.
BMI*: Body Mass Index.
WC†: Waist Circumference.
WtHR‡: Waist-to- Height Ratio.
유명진 외. 심혈관 관상동맥 이상과 비만지표 최적 변별점 Korean Journal of Family Practice
KJFP
질환 위험인자인 당뇨병, 고혈압 및 이상지질혈증의 위험성을 예 측하기 위한 허리둘레-키 비 최적 변별점을 분석한 결과, 남자는 0 . 50 , 여자는 0 . 51 임을 보고한 바 있다.
본 연구에서도 심혈관 관상동맥 동맥 이상 유무를 예측함에 있어 체질량지수나 허리둘레보다 허리둘레-키 비가 유용하게 나타났다.
이는 아시아인이 백인에 비해 같은 체질량지수에서도 더 높은 체지 방률을 갖거나 더 낮은 체질량지수에서 비만 관련 질환 위험성이 높 다는 과거 연구결과를 고려하면
15-21)한국인에 있어서 체질량 지수 가 복부 비만 정도를 반영하는데 있어 미흡한 점 있다고 사료하며, 한국인 역시 서양인에 비해 복부 비만 위험이 높을 것이라고 여겨진 다. 선행 연구들에서 허리둘레-키 비가 심혈관 질환 및 대사성 질 환에 있어 높은 상관관계를 가짐
23-25)을 볼 때 허리둘레-키 비를 이 용한 비만 지표의 임상 적용 확대 역시 고려할 여지가 있다.
비만 진단기준(체질량지수:남녀 모두 25 . 0kg / m
2이상, 허리둘레 남자 90cm 이상, 여자 85cm 이상) 및 기존의 최적 변별점에 비교 시 본 연구에서 체질량지수, 허리둘레, 허리둘레-키 비의 최적 변별점 은 남녀 각각 23 . 0kg / m
2, 20 . 2kg / m
2, 80cm , 82cm , 0 . 46 , 0 . 5 로 다 소 낮게 산출되었다. 최근 비만 기준의 보다 엄격한 적용에 대한 의 견이 대두되고 있는 상황에 비추어 볼 때 본 연구 결과가 최적 변별 점 설정에 참고가 될 수 있을 것이다.
본 연구의 제한점은 첫째, 일개 지역사회 2 차병원 한 곳에만 내 원한 수검자만을 선별하여 연구대상으로 했기 때문에 일반적 특성 을 반영하기에는 미흡한 점이 존재할 수 있다는 점, 둘째, 의무기록 확인만으로 가족력, 신체 활동 여부 등을 알 수 없는 점 등이라 하겠
다. 아울러, 흡연력, 기저 질환 같은 변수 중 일부는 수검자 응답에 만 의지하여 얻어져 비뚤림( bias )이 발생할 수 있다는 점이다. 이러 한 제한점에도 불구하고 내원한 수검자 특성이 환자가 아닌 검진 목 적으로 병원을 방문한 상대적으로 건강한 사람들이라는 점에 있어 신체 활동 상의 급격한 차이가 크지 않을 것이라 여겨지며, 회상에 의한 비뚤림 발생 역시 상대적으로 낮을 것으로 판단된다.
기존 연구들이 대사 증후군 진단 기준 등을 이용해 비만 지표의 변별점을 추정한 것에 비해 본 연구는 CCTA 라는 개관적 검사결과 에 의거하여 심혈관 이상 유무와 비만지표간의 관계를 제시하고자 하는 데에 의의가 있다고 하겠다. 향후 한국인에 맞는 적합한 신체 계측치의 기준 개발을 기대한다.
요 약
연구배경: 심혈관 평가에 있어 전산화 단층 촬영 기술의 발달로 관 상동맥 전산화 단층 촬영 혈관 조영술는 유용한 도구이다. 비만은 심혈관 질환의 위험 인자이다. 심혈관 질환자가 아닌 정상인에, 체 질량 지수, 허리둘레, 허리둘레-키 비등의 비만지표와 관상동맥 촬 영 결과를 분석하여 ROC 곡선을 이용 하여 각 신체 계측치의 최적 변별점을 추정 목적으로 본 연구를 기획하였다
방법: 2012 년 01 월 01 일부터 2012 년 12 월 31 일 기간 청주 효성병 원에 내원해 건강 검진을 받았던 수검자 중 관상동맥 전산화 단층 촬영 혈관 조영술 검사를 받았던 자를 연구대상으로 선정한 후 체질 량 지수, 허리둘레, 허리둘레-키 비에 따른 심혈관 이상 여부 예측 정도와 최적변별점을 ROC 곡선을 이용해 추정했다.
결과: 남녀 모두에서 예측 정도는 곡선 아래 면적( AUC )이 허리둘 레-키 비, 허리둘레, 체질량지수 순으로 나타났고, 체질량 지수의 최적 변별점은 남자에서 23 . 0kg / m
2, 여자에서 20 . 2kg / m
2였고, 허 리둘레의 경우 남자에서 80cm , 여자에서 82cm 였으며, 허리둘레- 키 비의 경우에는 남자에서 0 . 46 , 여자에서 0 . 5 였다.
결론: 심혈관 질환 및 대사성 질환에 예측에 있어 선행 연구 결과와 같이 본 연구에서도 허리둘레-키 비가 다른 비만 지표에 비해 심혈 관 이상 유무에 높은 상관 관계를 가졌다. 따라서, 허리둘레-키 비 를 이용한 비만 지표의 임상 적용 확대를 기대하며, 기존 비만 지표 에 비해 더 낮은 적정점에 논의 역시 기대한다.
중심단어: 심혈관 질환 , 관상동맥 전산화 단층 촬영 혈관 조영술, 비만 지표, ROC 곡선, 최적 변별
Table 4. Optimal anthropometric cut-points to predict CCTA result
Male(n= 516) Female(n= 160) Optimal BMI(kg/m2)
cut-point 23.0 20.2
Sensitivity 79.4 100
Specificity 30.4 14.0
AUC(95% CI) 0.5334
( 0.47167 to 0.59509)
0.5140 ( 0.36102 to 0.66695) Optimal WC(cm)
cut-point 80 82
Sensitivity 82.6 52.9
Specificity 27.6 77.6
AUC(95% CI) 0.5420
( 0.48040 to 0.60358)
0.6263 (0.47418 to 0.77839) Optimal WtHR
cut-point 0.46 0.5
Sensitivity 92.4 70.6
Specificity 20.5 61.5
AUC(95% CI) 0.5727
(0.51124 to 0.63406)
0.6281 (0.49389 to 0.76238)
* CI; Confidence Interval
† WC; Waist Circumference
‡ WtHR; Waist-to-Height Ratio
Myoung-Jin Yoo, et al. Optimal cut off points for obesity indices to predict coronary vascular abnormality.
Korean Journal of Family Practice
KJFP
REFERENCES
1. Fact sheet: Causes of death Statistics 2013 [Internet]. Daejeon:
Statistics Korea. Available from: http://www.kostat.go.kr.
2. Kim DH, Choi SI, Jeung EJ, Chang SA, Choi EK, Chang HJ et all. Coronary CT Angiography: Focus on a New Algorithm as Diagnostic Tool in Routine Clinical Practice. Journal of the Korean Societ -y of Radiology. 2007; 56: 461-4721.
3. Leschka S, Alkadhi H, Plass A, Desbiolles L, Grunenfelder J, Marincek B, et al. Accuracy of MSCT coronary angiography with 64-slice technology: first experience. Eur Heart J 2005; 26: 1482- 1487.
4. Cho IJ and Chang HJ, Division of Cardiology, Department of internal medicine, Yonsei University College of Medicine, Seoul, Korea, Current Uptodata and Clinical Application of Cardiac CT, The Korean journal of Medicine. 2013.
5. Maurovich-Horvat P, Ferencik M, Voros S, Merkely B, Hoffmann U, Comprehensive plaque asses -sent by coronary CT angiography, Nat Rev Cardiol. 2014 Jul; 11(7): 390-402.
6. Eue-Keun Choi, MD, Sang Il Choi, MD, Juan J.Rivera, MD, Khurram Nasir, MD, Suing-A Chang, MD, Eun Ju Chun, MD, et al, Seongnam-si, Gyeonggi-do, South Korea ; Baltimore, Maryland;
and Boston, Massachusetts, coronary computed tomography angiography as a screening tool for the detection of occult coronary artery disease in asymptomatic individuals, Journal of the American College of Cardiology. 2008; 52(5): 357-365.
7. Gilbert L. Raff, Kavitha M. Chinnaiyan, R icardo C. Cury, Mario T.
Garcia, Harvey H. Hecht, Judd E. Hollander, et al, SCCT guidelines on the use of coronary computed tomographic angiography for patients presenting with acute chest pain to the emergency department, Journal of Cardiov -ascular Computed Tomography 2014: 1-18
8. PS Singh, G Singh, SK Singh, Clinical profile and risk factors in acute coronary syndrome, JIACM 2013;14(2): 130-2.
9. Hubert HB, Feinleib M, McNamara PM, Castelli WP. Obesity as an independent risk factor for cardiovascular disease: A 26-year followup of participants in the Framingham Heart Study. Circul -ation. 1983; 67: 968-977.
10. Wilson PW, D'Agostino RB, Levy D, Belanger AM, Silbershatz H, Kannel WB. Prediction of coron -ary heart disease using risk factor categories.Circulation. 1998 May 12; 97(18): 1837-47.
11. Park HS. Cut-off Values of Waist Circumference for Abdominal Obesity among Koreans. Journ -al of the Korean Medial Association. 2005; 48(12): 1165-1172.
12. Böhning D, Böhning W, Holling H. Revisiting youden’s index as a useful measure of the miscla -ssification error in meta-analysis of diagnostic studies. Statistical Methods in Medical Research 2008:17(6):543-54.
13. Nakas CT, Yiannoutsos CT. Ordered multiple-class ROC analysis
with continuous measurement-s. Stat. Med. 2004; 23(22): 3437-49.
14. Arbab-Zadeh, Armin, and John Hoe. "Quantification of coronary arterial stenoses by multidetec-tor CT angiography in comparison with conventional angiography: methods, caveats, and implications.
Journal of the American College of Cardiology: Cardiovascular Imaging 2011; 4.2: 191-202.
15. Park Jong-Heon . Measuring BMI Cutoff Points of Korean Adults Using Morbidity of BMI relate -d Diseases. 2011. Korean Society for the Study of Obesity: 2011; 20: 36-43.
16. Deurenberg P, Deurenberg-Yap M, Guricci S. Asians are different from Caucasians and from e -ach other in their body mass index/
body fat per cent relationship.Obesity Reviews. 2002; 3: 141-6 17. WHO expert consultation. Appropriate body-mass index for Asian
populations and its implicati -ons for policy and intervention strategies. Lancet 2004; 363: 157-63.
18. Shiwaku K, Anuurad E, Enkhmaa B, Nogi A, K18. Deurenberg- Yap M, Chew SK, Lin VFP, Tan BY, Staveren WA, Deurenberg P.
Relationships between indices of obesity and its comorbidities in multi-ethnic Singapore, International Journal of Obesity 2001; 25:
1554-62.
19. Lin WY, Lee LT, Chen CY, Lo H, Hsia HH, Liu IL.et al. Optimal cut-off values for obesity: using Simple anthropometric indices to predict cardiovascular risk factors in Taiwan, International Jo -urnal of Obesity. 2002;26: 1232-8.
20. Shiwaku K, Anuurad E, Enkhmaa B, Nogi A, Kitajima K, Shimono K. et al. Overweight Japanese with body mass indexes of 23.0~24.9 have higher risks for obesity-associated disorders:
acomparison of Japanese and Mongolians. Int J Obes Relat Metab Disord.2004:28(1):152-8.
21. Chien LY, Liou YM, Chen JJ. Association between indices of obesity and fasting hyperglycemia in Taiwan. International Journal of Obesity 2004:28:690-6.
22. Kwon OH, Lee KM, No YM, Kim HY, Hwang SW, Jung SP.
Cardiovascular risk factors in men with normal and overweight according to waist-to-height ratio. The Korean Academy of Family Medicine 2001; 22(12): 1757-1764.
23. Park SH, Choi SJ, Lee KS, Park HY. Waist circumference and waist-to-height ratio as predictors of cardiovascular disease risk in Korean adults. Circ J 2009; 73(9): 1643-1650.
24. Lee CM, Huxley RR, Wildman RP, Woodward M. Indices of abdominal obesity are better Discriminators of cardiovascular risk factors than BMI: a meta-analysis. J Clin Epidemiol. 2008 ;61 :646-653.
25. Jawad A Al-Lawati, Nabil M Barakat, Alya M Al-Lawati, Ali J Mohammed. Optimal cut-points f-r body mass index, waist circumference and waist-to-hip ratio using the Framingham coronary heart disease risk score in an Arab population of the Middle East. Diabetes and Vascular Disease Research November 2008;5: 304-309