서 론
심혈관 질환은 2014년 통계청 자료에 의하면 사망 원인 중 2위이 며 , 그 비율은 증가 추세에 있다. 순환기계통 질환 사망률은 인구 10 만 명당 113.9명으로 심장 질환(52.4명), 뇌혈관 질환(48.2명), 고혈압 (10명) 순이었다.
1)심혈관 질환 중 대표적인 것은 허혈성 심장질환이 며, 관상동맥의 동맥경화가 허혈성 심장질환의 유발인자로서 질병 의 이환 및 사망과 높은 관련이 있는 것으로 제시되었다.
2)심혈관 질 환의 위험인자로는 흡연, 고혈압, 당뇨, 심혈관 질환의 가족력, 비만, 이상지질혈증 등이 있으며 그 중 비만은 독립적인 위험요인으로 널 리 알려져 있다.
3,4)비만 측정을 위한 신체 계측 지표로는 체질량지수(body mass in- dex, BMI), 허리둘레, 허리둘레-키 비 등이 있다. 비만지표 간의 비교 에서 허리둘레-키 비 또는 허리둘레가 심혈관 질환 예측에 있어 BMI 보다 유용하다는 여러 보고가 있다.
5-7)그러나 BMI는 임상적으로 가 장 많이 이용되는 비만지표이며 우리나라에서는 2000년 세계보건 기구 서태평양지역회의에서 제정한 기준을 사용하고 있다.
8)관상동맥의 평가에는 관상동맥 조영술(conventional coronary an- giography, CAG)이 가장 정확한 검사이나 침습적이며 비용과 시간의 문제로 건강한 성인의 진단 목적의 검사로는 이용되지 않고 있다. 이 에 관상동맥 전산화 단층촬영 혈관조영술(coronary computed to- mography angiography, CCTA)이 CAG를 대체하여 많이 이용되고 있
Original Article
관상동맥 질환의 예측을 위한 체질량지수의 최적 변별점
이우택, 장영근*, 권지은, 김성욱, 한정완, 신동렬
효성병원 가정의학과
Optimal Cutoff Points for Body Mass Index to Predict Coronary Artery Disease
Woo-Taek Lee, Young-Keun Jang*, Ji-Eun Kwon, Seong-Wook Kim, Jeong-Wan Han, Dong-Ryoul Shin
Department of Family Medicine, Hyosung Hospital, Cheongju, KoreaBackground: Obesity has been known as an independent risk factor of cardiovascular disease. We aimed to determine the optimal body mass index (BMI) for predicting coronary vascular disease. Conventional coronary angiography (CAG) and coronary computed tomography angiography (CCTA) have been used to detect significant coronary artery diseases.
Methods: We reviewed the medical records of 1,356 adults who visited a general hospital between January 2012 and December 2013. CAG was performed in 680 symptomatic patients who visited the emergency or outpatient department; and CCTA, in 676 asymptomatic patients who visited the health promotion center. Receiver-operating characteristic (ROC) analysis was used to determine the optimal cutoff BMI to predict coronary vascular abnormalities.
Results: The optimal cutoff BMIs in the CAG and CCTA groups were respectively 25.4 kg/m
2and 22.9 kg/m
2for males, and 23.5 kg/m
2and 24.7 kg/m
2for females.
Conclusion: The Regional Office for the Western Pacific (WPRO) criteria were used to categorize adult overweight and obesity. According to the WPRO criteria, overweight is defined by a BMI of 23 to 24.9 kg/m
2. The present results meet the WPRO criteria for overweight regardless of symptoms.
Keywords: Obesity; Body Mass Index; Receiver-Operating Characteristic; Coronary Artery Disease
http://dx.doi.org/10.21215/kjfp.2016.6.4.351eISSN 2233-9116
Korean J Fam Pract. 2016;6(4):351-355
KJFP
Korean Journal of Family PracticeReceived March 9, 2016 Revised May 6, 2016 Accepted June 1, 2016 Corresponding author Young-Keun Jang
Tel: +82-43-221-5000, Fax: +82-43-221-5010 E-mail: [email protected]
Copyright © 2016 The Korean Academy of Family Medicine
This is an open-access article distributed under the terms of the Creative Commons At- tribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Woo-Taek Lee, et al. Optimal Cutoff Points for BMI to Predict Coronary Artery Disease
Korean Journal of Family Practice
KJFP
다 . 여러 연구에 의하면 CCTA는 민감도 94%–100%, 특이도 75%–96%, 양성 예측도 78%–85%, 음성 예측도 97%–100%의 결과를 보여주었 다 .
9-12)최근 비만의 사회적 비용 증가에 따라 신체계측치의 최적 변별점 에 관한 여러 연구들이 시도되고 있다.
13-16)Yoo 등
17)연구에서 건강한 성인이 검진 시 시행한 CCTA의 결과를 이용하여 심혈관 이상 유무 에 따른 BMI의 최적 변별점을 추정한 바 있다. 이에 본 연구는 관상 동맥 질환의 예측을 위해 건강한 성인이 아닌 심혈관 증상을 보인 환자를 대상으로 시행한 CAG의 결과를 통해 BMI의 최적 변별점을 추정하고 이를 Yoo 등
17)의 결과와 비교해 보고자 한다.
방 법
1. 자료 출처 및 변수
2012년 1월 1일부터 2013년 12월 31일의 기간 동안 일개 종합병원 을 내원한 환자 중 심혈관 증상으로 응급실 또는 외래를 통해 CAG 를 시행한 836명과 건강 검진 시 CCTA를 시행한 무증상의 건강 성 인 762명을 연구 대상으로 선정하였다. 모든 자료는 의무 기록 확인 을 통해 획득하였다. CAG는 일개병원의 심장내과에 안정형 협십증, 불안정형 협심증, 급성 심근경색증의 상병으로 입원한 환자를 대상 으로 4명의 심장내과 전문의에 의해 시행되었다. CAG는 seldinger 방 법으로 대퇴동맥 또는 요골동맥에 삽입하여 시행하였으며 관상동 맥의 여러 투사면 중 가장 협착이 심한 부위의 내경을 caliper로 측정 하여 협착부에서 가장 가까운 거리에 있는 부위의 내경과 비교하여 백분율로 표시하였다. CCTA는 128-Slice-MDCT (optima 660 mode;
General Electronic, Fairfield, CT, USA)를 이용하였고 심장 박동수가 65회/분 이상이면 베타차단제를 복용시켜 65회/분 이하로 유지하였 다 . 대상자의 신장, 체중은 의료전문가가 직접 계측하였으며, 이를 통 해 BMI를 산출하였다. BMI는 체중(kg)을 신장의 제곱(m
2)으로 나누 어 구하였다.
의무기록으로 키, 체중의 정보를 확인할 수 없었던 31명과 검사 결 과를 확인할 수 없는 8명은 연구에서 제외하였다. 또한 이전에 심혈 관 질환으로 심장 시술을 받은 139명을 분석에서 제외하였고 인공물 (motion artifact)로 인해 관상동맥 협착 정도를 정확하게 평가하기 어 려웠던 70명의 자료도 분석에서 제외하여 CCTA를 시행한 환자 676 명과 CAG를 시행한 680명을 포함한 1,356명의 자료를 분석하였다.
2. 통계 분석 및 방법
CCTA를 시행한 군과 CAG를 시행한 군으로 이분화하여 BMI의 receiver-operating characteristic (ROC) 곡선을 구하였다. 심혈관 질환
유무에 따른 BMI의 최적 변별점 결정을 위해 ROC 곡선과 Youden 지수를 이용하여 추정하였다. Youden 지수를 이용하여 민감도와 특 이도의 합에서 1을 뺀 값이 최대가 되는 값으로 최적 변별점 선정하
였다.
18,19)모든 분석은 SAS version 9.3 (SAS Institute, Cary, NC, USA) 그
리고 R version 3.2.2 (Package ‘pROC’) 프로그램을 이용하여 분석하였 다.
결 과
1. 대상자의 일반적 특성
본 연구에는 총 1,356명의 대상자가 분석에 포함되었다. 이들 중 CAG를 시행한 군은 680명이었고 CCTA를 시행한 군은 676명이었다.
CAG를 시행한 군의 평균 연령은 남자 61.2세, 여자 67세로 여자가 더 높았다 (P<0.001). BMI는 남자 24 kg/m
2, 여자 24.5 kg/m
2으로 유의한 차이가 없었으며 평균 키는 남자 167.3 cm, 여자 154 cm였고 몸무게 는 남자 67.5 kg, 여자 58.1 kg으로 키와 몸무게 모두 남자가 더 높았다 (P<0.001). CCTA를 시행한 군의 평균 연령은 남자 48.7세, 여자 50.5세 로 유의한 차이가 없었다. BMI는 남자 24.6 kg/m
2, 여자 23.5 kg/m
2으 로 남자가 더 높았다(P<0.001). 평균 키는 남자 170.9 cm, 여자 158.1 cm로 남자가 더 높았으며, 몸무게는 남자 72 kg, 여자 58.8 kg으로 남 자가 더 높았다(P<0.001) (Table 1).
2. 심혈관 질환 이상 유무에 따른 환자 분류
CAG를 시행한 군은 여러 투사면 중 가장 협착이 심한 부위의 내 경을 caliper로 측정하여 협착부에서 가장 가까운 거리에 있는 부위 의 내경과 비교하여 백분율로 표시한 후, 내경이 50% 이상의 의미 있 는 협착을 보인 경우와 그렇지 않은 경우로 분류하였으며 병변의 형 태는 American College of Cardiology/American Heart Association
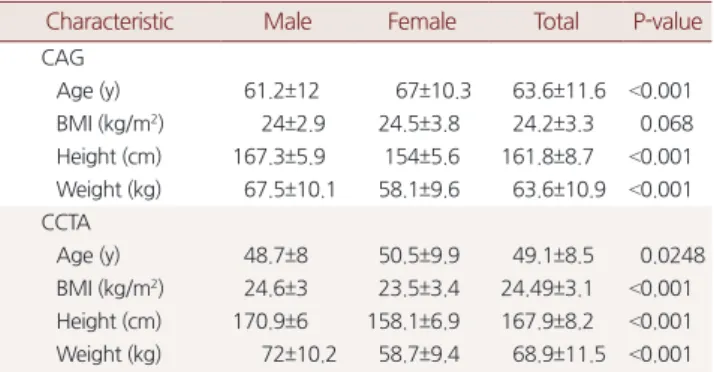
Table 1. Baseline characteristics by study groups
Characteristic Male Female Total P-value
CAG
Age (y) 61.2±12 67±10.3 63.6±11.6 <0.001 BMI (kg/m2) 24±2.9 24.5±3.8 24.2±3.3 0.068 Height (cm) 167.3±5.9 154±5.6 161.8±8.7 <0.001 Weight (kg) 67.5±10.1 58.1±9.6 63.6±10.9 <0.001 CCTA
Age (y) 48.7±8 50.5±9.9 49.1±8.5 0.0248
BMI (kg/m2) 24.6±3 23.5±3.4 24.49±3.1 <0.001 Height (cm) 170.9±6 158.1±6.9 167.9±8.2 <0.001 Weight (kg) 72±10.2 58.7±9.4 68.9±11.5 <0.001 Values are presented as mean±standard deviation.
CAG, conventional coronary angiography; BMI, body mass index; CCTA, coro- nary computed tomography angiography.
이우택 외. 관상동맥 질환의 예측을 위한 체질량지수의 최적 변별점 Korean Journal of Family Practice
KJFP
(ACC/AHA) 분류를 참고하였다.
20)CCTA를 시행한 군은 Journal of The American College of Cardiology (JACC) 발행된 자료에 근거해 6 단계
21)중 심혈관 협착 유무에 따라 두 군으로 분류하였다. 두 군 모 두 성별에 따라 분류하였다(Table 2).
3. 체질량지수의 최적 변별점
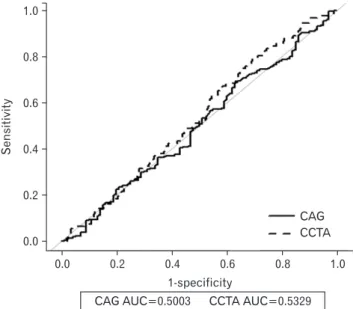
CAG를 시행한 군에서의 50% 이상의 심혈관 협착을 예측하기 위 한 BMI의 곡선 아래 면적(area under the curve, AUC)은 남자 0.5003, 여자 0.5601로 관찰되었다(Figures 1, 2). CAG군의 심혈관 질환 이상 유무를 예측하기 위한 최적 변별점은 남자 25.4 kg/m
2(민감도 68.9%, 특이도 37%), 여자 23.5 kg/m
2(민감도 45.6%, 특이도 67.4%)였다. CCTA
군의 AUC는 남자 0.5329, 여자 0.5173이었으며 심혈관 질환 이상 유 무를 예측하기 위한 최적 변별점은 남자 22.9 kg/m
2(민감도 79.4%, 특 이도 30.5%), 여자 24.7 kg/m
2(민감도 41.2%, 특이도 71.6%)였다(Table 3).
고 찰
비만은 과도한 지방이 체내에 축적된 상태로 고혈압, 당뇨병, 이상 지질혈증 , 관상동맥질환 등의 질환과 관련되어 유병률과 사망률을 증가시키는 것으로 알려져 있다. 비만 평가 지표로는 비만의 BMI, 허 리둘레 , 허리둘레-키 비 등이 있는데 그 중 BMI가 세계적으로 가장 널리 통용되고 있다.
BMI를 통해 비만 관련 질환들의 이환율과 사망률에 대한 다양한
Table 2. Distribution of participants by coronary vascular abnomality*,sex
Coronary vasculature Male Female Total
CAG Stenosis <50% 100 89 189
Stenosis ≥50% 296 195 491
Total 396 284 680
CCTA Normal 426 141 567
Abnormal 92 17 109
Total 518 158 676
Values are presented as number.
CAG, conventional coronary angiography; CCTA, coronary computed tomogra- phy angiography.
*We distributed participants two groups as coronary artery stenosis <50% and coronary artery stenosis ≥50% by CAG result. And we distributed participants two groups as normal group that have no coronary abnomality & abnormal group have any obstructive lesion by CCTA result.
Table 3. Optimal BMI cut-points to predict CAG & CCTA result
Variable Male Female
CAG Optimal BMI cut-point (kg/m2) 25.4 23.5
Sensitivity (%) 68.9 45.6
Specificity (%) 37 67.4
AUC (95% confidence interval) 0.5003 (0.4336–0.5671)
0.5601 (0.4891–0.6312) CCTA Optimal BMI cut-point (kg/m2) 22.9 24.7
Sensitivity (%) 79.4 41.2
Specificity (%) 30.5 71.6
AUC (95% confidence interval) 0.5329 (0.4712–0.5945)
0.5173 (0.3636–0.6711) BMI, body mass index; CAG, conventional coronary angiography; CCTA: coro- nary computed tomography angiography; AUC, area under the curve.
0.0 0.2 0.4 0.6 0.8
1.0
0.8
0.6
0.4
0.2
1.0
Sensitivity
1-specificity 0.0
CAG CCTA
CAG AUC=0.5003 CCTA AUC=0.5329
Figure 1. Receiver-operating characteristic curve of body mass index and their AUC for male predicting coronary vascular abnormality.
CAG, conventional coronary angiography; CCTA, coronary computed tomography angiography; AUC, area under the curve.
0.0 0.2 0.4 0.6 0.8
1.0
0.8
0.6
0.4
0.2
1.0
Sensitivity
1-specificity 0.0
CAG CCTA
CAG AUC=0.5601 CCTA AUC=0.5173
Figure 2. Receiver-operating characteristic curve of body mass index and their AUC for female predicting coronary vascular abnormality.
CAG, conventional coronary angiography; CCTA, coronary computed tomography angiography; AUC, area under the curve.
Woo-Taek Lee, et al. Optimal Cutoff Points for BMI to Predict Coronary Artery Disease
Korean Journal of Family Practice
KJFP
연구들이 시도되었다.
Zheng 등
22)의 연구에서는 중국인, 일본인, 한국인을 포함한 극동 아시아인에서 BMI가 22.6–27.5 kg/m
2사이일 때 비만 관련 질환으로 인한 사망률의 위험도가 가장 낮았다고 보고하였다. 사망 위험도는 BMI가 35 kg/m
2보다 높으면 1.5배, 15 kg/m
2보다 낮으면 2.8배 증가하 였다고 한다. 한국인만을 대상으로 한 Jee 등
23)의 연구에 따르면, BMI 가 23–24.9 kg/m
2사이일 때 비만 관련 질환으로 인한 사망률이 가장 낮았으며 심혈관 질환의 경우에는 BMI가 높을수록 위험도가 증가 하는 것으로 보고 하였다. Low 등
24)은 논문 리뷰를 통해 아시아인의 비만 기준이 낮아져야 한다고 주장하였다. 이러한 연구들을 근거로 세계보건기구 아시아태평양 지역과 대한비만학회에서는 과체중의 기준을 BMI가 23 kg/m
2이상, 비만의 기준을 25 kg/m
2이상으로 정의 하였다 .
8)이는 동양인은 서양인에 비해 상대적으로 복부지방과 체지 방률이 높아 BMI를 30 kg/m
2이상으로 정의하면 비만관련 건강위험 을 과소평가할 우려가 있기 때문이다.
BMI의 최적 변별점에 대한 국내외에서 활발한 연구들이 시행되 었다 . Razak 등
13)은 유럽인과 비교하였을 때 남부 아시아인에서 비만 기준이 6 kg/m
2더 낮아져야 한다고 주장하였다. Lin 등
16)은 타이완 사람들을 대상으로 진행한 연구에서 ROC 분석을 통해 BMI의 최적 변별점은 남자 23.6 kg/m
2, 여자 22.1 kg/m
2으로 보고하였다. 한편 한 국인을 대상으로한 Oh 등
25)의 코호트 연구에서는 백인과 비교하였 을 때 한국인에서 BMI 25 kg/m
2이상이 더 큰 위험도를 보이지 않았 다고 보고하였다. 그러나 BMI 25 kg/m
2이상이 빠르게 증가하고 있 고 비만과 관련된 건강문제도 빠르게 증가하고 있기 때문에 질병의 예방을 위해 BMI 25 kg/m
2을 사용하는 것을 권장하였다.
한국인의 BMI 변별점 측정을 한 박의 연구에서는 BMI와 유의한 양의 상관성을 갖는 질환 이환율을 기준으로 추정된 한국 성인의 BMI 최적 변별점을 23.0–24.5 kg/m
2사이로 추정하였다.
26)본 연구에 서 CAG를 시행한 군의 평균 BMI는 남자 24 kg/m
2, 여자 24.5 kg/m
2였 고 CCTA를 시행한 군의 평균 BMI는 남자 24.6 kg/m
2, 여자 23.5 kg/
m
2으로 Park
26)의 평균 BMI 23.13–24.08 kg/m
2, 여자 23.01–23.17 kg/m
2보다 높았다. 본 연구에서 급성 관상동맥 증후군으로 CAG를 시행 한 군에서는 남자 25.4 kg/m
2, 여자 23.5 kg/m
2으로 BMI의 최적 변별 점으로 나타났으며 CCTA를 시행한 군에서는 남자 22.9 kg/m
2, 여자 24.7 kg/m
2으로 나타났다. 이는 Park
26)연구의 추정치와 유사하며 세 계보건기구 서태평양지역회의에서 재정의한 아시아인의 과체중 구 간의 범위와 유사하다. 이는 한국인에서는 백인보다 낮은 BMI 변별 점을 적용하는 BMI의 재정의가 유효하다는 점을 지지하고 있다. 본 연구의 AUC 값이 낮은 이유는 대상자의 평균 연령이 높아 정확성이 떨어지는 것으로 보인다. Park
26)의 연구에서도 60세 이상의 고연령구
간에서 AUC 값이 0.6 이하였다. CAG군의 결과에는 80세 이상이 49 명이 포함되어 있어 비만 역설
27,28)의 영향이 있을 수 있다. 실제로 CCTA군에서는 77세가 최고령이었고 CAG군에서는 106세가 최고령 이었다.
본 연구의 제한점은 첫째, 일개 종합병원을 내원한 수검자를 대상 으로 이루어졌기 때문에 한국인의 일반적 특성으로 보기에는 편견 이 있을 수 있다는 점이다. 둘째, 심혈관 이상 유무만을 반영하였고 고혈압 , 당뇨병, 고지혈증 등의 다양한 질환의 이환율을 고려하지 않 았다 . 셋째, 성별에 구분을 두어 결과를 도출하였으나 연령대별로 분 석하지 못해 결과 해석에 제한이 있을 수 있다. 넷째, 여러 연구
6,29)에 따르면 허리둘레-키 비, 허리둘레, BMI 순으로 심혈관 질환의 발생에 큰 영향을 미친다고 보고되고 있는데 본 연구에서는 CAG군의 허리 둘레에 대한 의무기록이 없어 허리둘레-키 비, 허리둘레에 대한 최 적 변별점을 제시하지 못한 점이다.
그럼에도 불구하고 본 연구는 BMI의 최적 변별점이 기존 연구 결 과들과 유사한 결과를 보였다는 점과 증상 여부의 차이에도 두 군 에서 비슷한 결과를 보인 점에서 의의가 있다고 하겠다. 이러한 결과 는 건강한 성인의 심혈관 질환 예방을 위하여 적절한 BMI 기준 제시 에 기여할 것으로 생각된다. 향후 고연령군에 대한 다른 접근 방법과 중심성 비만에 대한 추가적인 연구가 필요하며 이는 비만 평가의 기 준을 정하는 데 도움이 될 것으로 기대된다.
요 약
연구배경: 비만은 심혈관 질환의 독립적인 위험요인으로 알려져 있 다. 비만 지표 중 체질량지수는 널리 이용되며 최근 최적 변별점에 대한 연구가 활발히 진행되고 있다. 이에 따라 본 연구에서는 관상 동맥의 평가에 흔히 사용되는 관상동맥 조영술과 관상동맥 전산화 단층촬영 혈관조영술을 이용하여 관상동맥 질환의 예측을 위해 체 질량지수의 최적 변별점을 추정하고자 한다.
방법: 2012년 1월 1일부터 2013년 12월 31일의 기간 동안 일개 종합병 원을 내원한 1,356명을 연구 대상에 포함하였다. 그 중 680명은 심혈 관 증상으로 응급실 또는 외래를 통해 관상동맥 조영술을 시행하였 고 , 676명은 건강한 성인으로 검진센터에서 관상동맥 전산화 단층 촬영 혈관조영술을 시행하였다. Receiver-operating characteristic 곡선 을 통해 심혈관 이상을 예측하기 위한 체질량지수의 최적 변별점을 추정하였다 .
결과: 관상동맥 조영술을 시행한 군의 최적 변별점은 남녀 각각 25.4
kg/m
2, 23.5 kg/m
2으로 추정되었다. 관상동맥 전산화 단층촬영술 검
사를 받은 군의 최적 변별점은 남녀 각각 22.9 kg/m
2, 24.7 kg/m
2였다 .
이우택 외. 관상동맥 질환의 예측을 위한 체질량지수의 최적 변별점 Korean Journal of Family Practice
KJFP
결론: 심혈관 질환 예측을 위한 체질량지수의 최적 변별점은 심혈 관 증상에 관계없이 세계보건기구 서태평양지역회의에서 정의한 과 체중 구간과 유사한 값을 보였다.
중심단어: 비만; 체질량지수; 수신자 조작 특성; 관상동맥 질환
REFERENCES
1. Fact sheet. Cause of death statistics 2014 [Internet]. Daejeon: Statistics Ko- rea; 2015 [cited 2016 Feb 29]. Available from: http://www.kostat.go.kr.
2. Fuster V, Badimon L, Badimon JJ, Chesebro JH. The pathogenesis of coro- nary artery disease and the acute coronary syndromes (1). N Engl J Med 1992; 326: 242-50.
3. Yadav P, Joseph D, Joshi P, Sakhi P, Jha RK, Gupta J. Clinical profile & risk factors in acute coronary syndrome. National J Comm Med 2010; 1: 150-1.
4. Hubert HB, Feinleib M, McNamara PM, Castelli WP. Obesity as an inde- pendent risk factor for cardiovascular disease: a 26-year follow-up of partic- ipants in the Framingham heart study. Circulation 1983; 67: 968-77.
5. Lee CM, Huxley RR, Wildman RP, Woodward M. Indices of abdominal obesity are better discriminators of cardiovascular risk factors than BMI: a meta-analysis. J Clin Epidemiol 2008; 61: 646-53.
6. Dobbelsteyn CJ, Joffres MR, MacLean DR, Flowerdew G. A comparative evaluation of waist circumference, waist-to-hip ratio and body mass index as indicators of cardiovascular risk factors. The Canadian Heart Health Sur- veys. Int J Obes Relat Metab Disord 2001; 25: 652-61.
7. Savva SC, Tornaritis M, Savva ME, Kourides Y, Panagi A, Silikiotou N, et al.
Waist circumference and waist-to-height ratio are better predictors of car- diovascular disease risk factors in children than body mass index. Int J Obes Relat Metab Disord 2000; 24: 1453-8.
8. World Health Organization. The Asia-Pacific Perspective: Redefining obe- sity and its treatment. Geneva: World Health Organization Western Pacific Regional Office; 2000.
9. Alkadhi H, Stolzmann P, Desbiolles L, Baumueller S, Goetti R, Plass A, et al.
Low-dose, 128-slice, dual-source CT coronary angiography: accuracy and radiation dose of the high-pitch and the step-and-shoot mode. Heart 2010;
96: 933-8.
10. Leschka S, Stolzmann P, Desbiolles L, Baumueller S, Goetti R, Schertler T, et al. Diagnostic accuracy of high-pitch dual-source CT for the assessment of coronary stenoses: first experience. Eur Radiol 2009; 19: 2896-903.
11. Carrascosa P, Capuñay C, Deviggiano A, Goldsmit A, Tajer C, Bettinotti M, et al. Accuracy of low-dose prospectively gated axial coronary CT angiogra- phy for the assessment of coronary artery stenosis in patients with stable heart rate. J Cardiovasc Comput Tomogr 2010; 4: 197-205.
12. Pugliese F, Mollet NR, Runza G, van Mieghem C, Meijboom WB, Malagutti P, et al. Diagnostic accuracy of non-invasive 64-slice CT coronary angiogra- phy in patients with stable angina pectoris. Eur Radiol 2006; 16: 575-82.
13. Razak F, Anand SS, Shannon H, Vuksan V, Davis B, Jacobs R, et al. Defining
obesity cut points in a multiethnic population. Circulation 2007; 115: 2111-8.
14. Ko GT, Tang JS. Waist circumference and BMI cut-off based on 10-year car- diovascular risk: evidence for “central pre-obesity”. Obesity (Silver Spring) 2007; 15: 2832-9.
15. Oka R, Kobayashi J, Yagi K, Tanii H, Miyamoto S, Asano A, et al. Reassess- ment of the cutoff values of waist circumference and visceral fat area for identifying Japanese subjects at risk for the metabolic syndrome. Diabetes Res Clin Pract 2008; 79: 474-81.
16. Lin WY, Lee LT, Chen CY, Lo H, Hsia HH, Liu IL, et al. Optimal cut-off val- ues for obesity: using simple anthropometric indices to predict cardiovascu- lar risk factors in Taiwan. Int J Obes Relat Metab Disord 2002; 26: 1232-8.
17. Yoo MJ, Kim SH, Jang YK, Shin WY, Han JW, Lee WT. Optimal cut off points for obesity indices to predict coronary vascular abnormality. Korean J Fam Pract 2015; 5: S912-6.
18. Fluss R, Faraggi D, Reiser B. Estimation of the Youden index and its associat- ed cutoff point. Biom J 2005; 47: 458-72.
19. Böhning D, Böhning W, Holling H. Revisiting Youdens index as a useful measure of the misclassification error in meta-analysis of diagnostic studies.
Stat Methods Med Res 2008; 17: 543-54.
20. Guidelines for percutaneous transluminal coronary angioplasty: a report of the American College of Cardiology/American Heart Association Task Force on assessment of diagnostic and therapeutic cardiovascular proce- dures (subcommittee on percutaneous transluminal coronary angioplasty).
J Am Coll Cardiol 1988; 12: 529-45.
21. Arbab-Zadeh A, Hoe J. Quantification of coronary arterial stenoses by mul- tidetector CT angiography in comparison with conventional angiography:
methods, caveats, and implications. JACC Cardiovasc Imaging 2011; 4: 191- 202.
22. Zheng W, McLerran DF, Rolland B, Zhang X, Inoue M, Matsuo K, et al. As- sociation between body-mass index and risk of death in more than 1 mil- lion Asians. N Engl J Med 2011; 364; 719-29.
23. Jee SH, Sull JW, Park J, Lee SY, Ohrr H, Guallar E, et al. Body-mass index and mortality in Korean men and women. N Eng J Med 2006; 355; 779-87.
24. Low S, Chin MC, Ma S, Heng D, Deurenberg-Yap M. Rationale for redefin- ing obesity in Asians. Ann Acad Med Singapore 2009; 38: 66-9.
25. Oh SW, Shin SA, Yun YH, Yoo T, Huh BY. Cut-off point of BMI and obesity- related comorbidities and mortality in middle-aged Koreans. Obes Res 2004; 12: 2031-40.
26. Park JH. Measuring BMI cutoff points of Korean adults using morbidity of BMI- related diseases. Korean J obes 2011; 20: 36-43.
27. Dorner TE, Rieder A. Obesity paradox in elderly patients with cardiovascu- lar diseases. Int J Cardiol 2012; 155: 56-65.
28. Oreopoulos A, Kalantar-Zadeh K, Sharma AM, Fonarow GC. The obesity paradox in the elderly: potential mechanisms and clinical implications. Clin Geriatr Med 2009; 25: 643-59.
29. Park SH, Choi SJ, Lee KS, Park HY. Waist circumference and waist-to-height ratio as predictors of cardiovascular disease risk in Korean adults. Circ J 2009; 73: 1643-50.