DOI : 10.3341/jkos.2009.50.2.303
= 증례보고 =
굴절교정레이저각막절제술 10년 후 각막조직의 공초점현미경 소견
신민규⋅구기홍⋅이종수
부산대학교 의학전문대학원 안과학교실목적: 굴절교정레이저각막절제술 10년 후 보이는 각막조직의 변화에 대하여 공초점현미경을 이용하여 정상각막과 비교 관찰하고자 하였다.
증례요약: Confocal microscopy (Confoscan 4.0, Fortune Technology, Italy)를 이용하여, 굴절교정레이저각막절제술 후 10년이 지난 외래 경과관찰 중인 40대 남, 여 각각 1명을 대상으로 하여 각막의 상피세포, 보우만막, 간질층, 데스메막, 내피세포층으로 나누어 정상 과 비교 관찰하였다. 굴절교정레이저각막절제술 후 각막의 상피세포는 거의 정상소견이었으며, 상피하 신경망은 어느 정도 회복되어 있었으나 아직도 고반사를 보이는 영역이 재생되는 신경에서 관찰되었다. 보우만막의 소실로 상피하 신경망 주위로 각막세포와 세포 외간질이 관찰되었다. 각막간질의 앞쪽 부위에서 불균등한 간질세포의 분포를 보였지만, 중간 및 심부의 간질세포는 큰 변화를 보이지 않았고, 각막내피세포의 변화도 관찰할 수 없었다.
결론: 굴절교정레이저각막절제술 후 10년이 지나더라도 각막조직 전안부 특히 상피하 신경망층과 각막간질조직의 앞쪽 각막간질세포 에서는 각막 창상 조직회복에 따른 조직의 변화를 관찰할 수 있었다.
<대한안과학회지 2009;50(2):303-307>
■ 접 수 일: 2008년 5월 9일 ■ 심사통과일: 2008년 8월 29일
■ 통 신 저 자: 이 종 수
부산시 서구 아미동 1-10 부산대학교병원 안과
Tel: 051‐240‐7957, Fax: 051‐242‐7341 E-mail: [email protected]
* 본 논문의 요지는 2008년 대한안과학회 제99회 춘계학술대회에서 포스터로 발표되었음.
Trokel et al1에 의해 굴절교정레이저 수술이 굴절교정방 법으로 도입된 이후, 중등도 근시환자를 치료할 수 있는 효 과적이고 안전한 방법이 되었다.2,3 비록 레이저굴절교정술 시행환자가 많이 늘어나는 추세이지만 3년 이상의 장기간 경과를 보고한 경우는 드물다.4,5Moilanen et al6에 의하면 굴절교정레이저각막절제술 후 5년이 지난 시점에서 상피하 신경층의 회복을 보였고 상피 및 각막실질, 내피세포에는 정상과 비교해 큰 차이가 없음을 보고하였고, Erie et al7은 각막간질 앞부분의 각막세포 밀도가 술 후 6개월 지점부터 감소하며, 각막간질 후반부의 각막세포의 밀도감소도 술 후 5년이 지나서야 관찰된다고 하였다. 따라서 굴절교정레이 저각막절제술 후 장기적 각막조직변화의 연구에 비침습적 인 방법인 공초점현미경을 이용하면 각막의 세포, 신경, 반 흔 조직 등을 쉽게 관찰할 수 있는 장점이 있어 굴절교정레 이저각막절제술 후 각막의 형태와 신경을 포함한 각막조직 의 변화를 분석할 수 있다.8-10
이에 저자들은 국내에서도 공초점현미경을 이용한 연구 가 진행되고 있으나, 굴절교정레이저각막절제술 후 장기간
이 경과한 후 각막소견에 대한 보고가 없기에 정상 대조군 과 비교하여 문헌고찰과 함께 보고하는 바이다.
증례보고
굴절교정레이저각막절제술 후 10년이 지난 40대 남녀 2 명 4눈에 대하여 공초점현미경(Confoscan 4.0, Fortune Technology, Italy)으로 각막조직을 관찰하였고, 술 전 각 막의 공초점현미경 촬영이 이루어지지 못했기에 이에 대응 하는 대조군으로 같은 연령대의 안과수술의 병력이 없으며 세극등 검사상 외안부 질환이 없는 건강한 눈을 비교 선택 하였다. 43세 여자환자 및 42세 남자환자는 각각 술전 -4 디옵터 및 -3.5 디옵터의 중등도의 근시를 가지고 있었으 며, 술후 큰 합병증은 없었다. 검사방법은 점안마취제로 Proparacaine hydrochloride 0.5% (Alcon, Ft. Worth, TX) 를 점안한 후, 시축이 기계의 중심에 오도록 눈높이를 조절 하여 중심부의 깊은 각막구조의 관찰이 가능하게 하였다.
ConfoScan 4.0의 대물렌즈를 70% isopropyl alcohol을 사용하여 깨끗이 닦고, ViscoTears Gel (0.2% acido poliacrilic), (CIBA Ophthalmicus, Macron, Italy)을 한 방 울 묻혀 각막 중심부의 상피세포층에 접촉시키고 조절막대 를 이용하여 1초당 32 micron씩 이동하면서 내피세포부 터 상피세포까지의 단면상을 관찰하였다. ConfoScan 4.0 은 약 40배의 objective magnification을 가지고 있고, 렌 즈의 앞면과 대상물체 사이, 즉 working distance는 2 mm,
A B
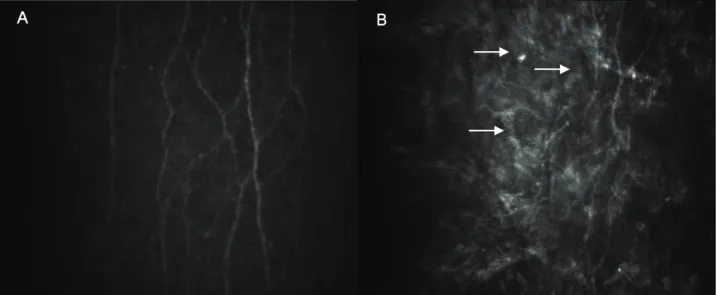
Figure 1. Confocal microscopic images of the subbasal nerve plexus layer of the cornea in the control (A) and corresponding post-PRK corneas (B). (A) Normal subbasal nerve plexus. (B) In post-PRK corneas, the anterior keratocyte and some hyperreflective ECM were imaged together with regenerated nerve plexus (arrow).
B A
Figure 2. Confocal microscopic images of the anterior stromal layer of the cornea in the control (A) and corresponding post-PRK corneas (B). (A) Evenly distributed anterior keratocytes. (B) Unevenly distributed anterior keratocytes (arrow) showed decreased cellular density and some hyperreflectivity.
numerical aperture가 0.75, 필드상의 크기는 340×255 micron이고 한번 검사할 때마다 약 350 images를 관찰할 수 있도록 되어 있다. 나아가optical slice thickness를 조절 할수 있는데, 이번 검사에서는 약 5~10 micron 정도를 유 지하도록 하고,1눈 당 3번씩의 검사를 시행하였다. 검사가 완 료되면 영상은 NAVIS software의 Digital Video Recorder (DVR)에 저장이 되어 자료가 필요할 경우 사용할 수 있었 다. 이를 이용하여 얻은 영상을 바탕으로 굴절교정레이저각 막절제술 후 10년이 경과한 시점의 각막상피세포, 보우만 막, 간질층, 데스메막, 내피세포층을 정상 대조군과 비교하
여, 그 차이를 관찰하였다. 정상 대조군의 각막 공초점현미 경 소견으로 상피세포는 밝은 핵을 가지고 있었고, 날개세 포는 세포경계가 뚜렸하였고, 아래로 상피하 신경층이 명확 하게 관찰되었다(Fig. 1A). 각막간질세포는 전형적으로 앞 쪽 부위에서는 각막세포의 밀집을 보였고(Fig. 2A), 핵의 형태가 내피세포에 가까울수록 원형의 모양을 보였다. 간혹 각막간질에서도 신경망이 관찰되기도 하고, 내피세포는 균 일하게 분포된 전형적인 육각형의 모양을 보였다. 이에 반 해 굴절교정레이저각막절제술을 한 눈의 경우 각막상피 및 날개세포는 정상과 큰 차이를 보이지 않았고, 상피하 신경
C D A B
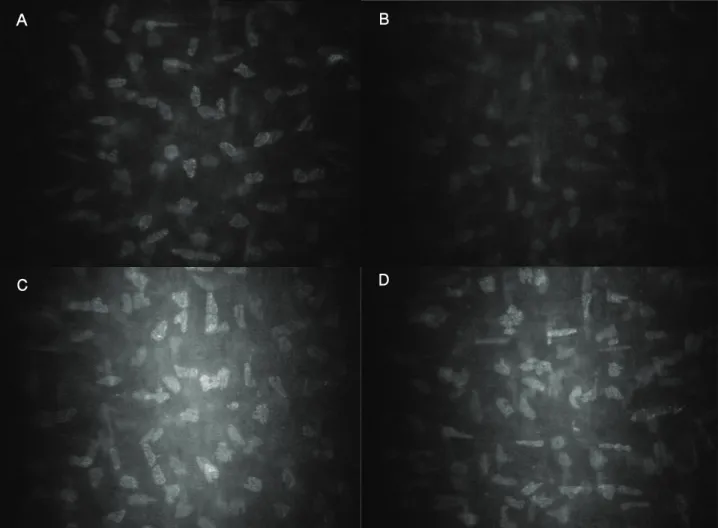
Figure 3. Confocal microscopy images of the middle and posterior stromal layer of the cornea in the control (A, C) and corresponding post-PRK corneas (B, D). (A) Midstromal keratocytes. (B) Only minor changes were observed in the post-PRK midstroma. (C, D) The posterior cornea appeared unaffected in both groups.
층은 거의 회복된 모습이었으나 주위에는 부분적으로 염주 알 모양의 고반사 음영이 신경부위에서 관찰되었으며, 상피 하혼탁 및 각막실질 세포가 관찰되었다(Fig. 1B). 이때 새 로 재생된 신경망은 정상과는 달리 울퉁불퉁한 분절을 이 루는 모양을 취하고 있었고, 각막간질세포는 앞쪽에서 불균 등한 각막세포의 분포를 보였다. 즉 각막간질세포의 밀도가 감소되어 있었고, 고반사를 나타내는 세포외기질의 축적인 주변 구조물이 관찰되었다(Fig. 2B). 중간 및 뒷부위의 각 막간질세포는 정상 대조군의 유사한 각막층의 조직변화에 비해서 미묘한 것이었고(Fig. 3), 각막내피세포는 육각형의 모양을 나타내면서 거의 정상 소견을 보였다.
고 찰
최근의 연구에 따르면, 굴절교정레이저각막절제술 후 세 극등 검사상 깨끗하게 보이는 각막도 공초점현미경 하에서 는 상피하 신경망 및 상피하 각막세포층에 변화가 있음이
보고 되었다.6이전의 연구에 따르면 상피하 신경망은 굴절 교정레이저각막절제술 후 1~4달이 지나면 각막중심부에서 관찰이 가능하다고 하였다.11 Erie12에 의하면, 굴절교정레 이저각막절제술 후 2년이 지나면 술전의 상피하 신경망이 재생된다 하였다. 10년이 지난 본 증례의 소견은, 환자의 신경망은 정상각막과 유사하게 새로이 재생이 되었으나, 분 지하는 형태가 다소 구불구불한 모양을 보였다. 이런 재생 되는 상피하 신경섬유는 장기간이 경과하면서 원래의 신경 패턴으로 재생된다. 그러나, 이러한 상피하 신경망의 재생 이 기능적으로 완전한 회복을 의미하는 지에 대해서는 아 직 연구가 진행되고 있다. 굴절교정레이저각막절제술 후 보 고되는 첫 1달 이내의 건성안의 증상은 이러한 신경층의 손 상과 연관이 있는 것으로 보인다.13굴절교정레이저각막절 제술 후 보우만막이 결여되는 것은 신경의 재생 및 방향성 에 장애를 초래하며, 상피세포과 기질세포간의 상호관계에 변화를 초래할 수 있다.14,15 본 연구에서도 상피하 신경망 주위에 각막 앞부분의 각막세포가 같이 관찰되는 것으로
막은 각막에서 필수적인 요소는 아니며, 새로 형성된 기저 막이 신경의 재생에 충분히 작용할 수 있을 것으로 생각되 며, 본 증례의 경우 공초점현미경으로는 반사를 보이지 않 는 기저막을 감지할 수 없었다.
상피세포하 혼탁의 발생은 각막세포가 고반사를 보이는 근섬유모세포로의 변환 및 새로 합성된 세포외 기질의 불 규칙적인 침착으로 인한 빛의 산란과 연관이 있다고 보고
되었다.16,17각막상피층은 정상과 거의 유사하게 재생이 되
고, 앞부분의 각막실질에 혼탁이 보이는 것은 상피와 기질 세포간의 상호작용에 의한 것으로 보이며 신경장애가 이러 한 변화에 관계하는 것으로 보인다.18 보우만막의 결여와 상피와 각막 기질세포간의 불균일한 접촉면은 reflectivity 를 초래하며 이는 상피하 신경망의 확인을 다소 힘들게 한 다. 이러한 변화된 구조이지만 상피하 신경망은 수년에 걸 쳐서 재생을 한다. 그러나 이러한 변화는 공초점현미경에 서만 관찰가능했으며, 환자는 주관적 증상을 호소하지 않 았다.
저자들은 굴절교정레이저각막절제술 후 10년이 지난 환 자에서 공초점현미경을 통하여 각막의 형태학적 변화를 정 상각막과 비교하여, 상피세포, 각막 간질 후반부 및 내피세 포에는 정상과 차이가 없음을 확인하였고, 각막 상피하 신 경층의 구불구불한 재생형태, 주변부 혼탁, 고반사를 띄는 세포외기질 및 각막 전부 간질세포의 불균등한 분포 등을 일부 확인할 수 있었다. 향 후 보다 많은 증례를 이용한 장 기간 관찰을 통한 자료의 수집 및 분석으로 굴절교정레이 저각막절제술 후 각막의 재생에 대한 검증이 이루어 질 수 있을 것이며, 술 후 비정상적 소견의 진단 및 치료계획 수 립 및 예후를 평가하는데 유용하게 활용할 수 있을 것이다.
참고문헌
1) Trokel SL, Srinnivasan R, Braren B. Excimer laser surgery of the cornea, Am J Ophthalmol 1983;96:710-5.
2) Epstein D, Fagerholm P, Hamberg-Nyström H, Tengroth B.
Twenty-four month follow-up of excimer laser photorefractive keratectomy for myopia: refractive and visual acuity results.
Ophthalmology 1994;101:1558-63.
3) Dutt S, Steinert RF, Raizman MB, Puliafito CA. One-year
moderate myopia. Arch Ophthalmol 1994;112:1427-36.
4) Kim JH, Kim MS, Hahn TW, et al. Five year results of photo- refractive keratectomy for myopia. J Cataract Refract Surg 1997;23:731-5.
5) Stephenson CG, Gartry DS, O’Brart DP, et al. Photo- refractive keratectomy: a 6-year follow-up study. Ophthalmology 1998;105:273-81.
6) Moilanen JA, Vesaluoma MH, Müller LJ, Tervo TM. Long- term corneal morphology after PRK by in vivo confocal microscopy. Invest Ophthalmol Vis Sci 2003;44:1064-9.
7) Erie JC, McLaren JW, Hodge DO, Bourne WM. Long-term corneal keratoctye deficits after photorefractive keratectomy and laser in situ keratomileusis. Trans Am Ophthalmol Soc 2005;103:56-68.
8) Rosenberg ME, Tervo TM, Petroll WM, Vesaluoma MH. In vivo confocal microscopy of patient with corneal recurrent erosion syndrome or epithelial basement membrane dystrophy.
Ophthalmology 2000;107:565-73.
9) Rosenberg ME, Tervo TM, Immonen IJ, et al. Corneal structure and sensitivity in typeⅠdiabetes mellitus. Invest Ophthalmol Vis Sci 2000;41:2915-21.
10) Linna T, Tervo T. Real-time confocal microscopic observations on human corneal nerves and wound healing after excimer laser photorefractive keratectomy. Curr Eye Res 1997;16:
640-49.
11) Frueh BE, Cadez R, Böhnke M. In vivo confocal microscopy after photorefractive keratectomy in humans: a prospective, long-term study. Arch Ophthalmol 1998;116:1425-31.
12) Erie JC. Corneal wound healing after photorefractive kera- tectomy: a 3-year confocal microscopy study. Trans Am Ophthalmol Soc 2003;101:287-328.
13) Ozdamar A. Aras C, Karakas N, et al. Changes in tear flow and tear film stability after photorefractive keratectomy.
Cornea 1999;18:437-9.
14) Seiler T, McDonnell P. Excimer laser photorefractive kera- tectomy. Surv Ophthalmol 1995;40:89-118.
15) Li DQ, Tseng SC. Three patterns of cytokine expression potentially invlolved in epithelial-fibroblast interactions of human ocular surface. J Cell Phys 1995;163:61-79.
16) Møller-Pedersen T, Cavanagh HD, Petroll WM, Jester JV.
Stromal wound healing explains refractive instability and haze development after photorefractive keratectomy: a 1-year confocal microscopic study. Ophthalmology 2000;107:1235-45.
17) Lohmann C, Gartry D, Kerr Muir M, et al. “Haze” in photorefractive keratectomy; its origins and consequences.
Laser Light Ophthalmol 1991;4:15-34.
18) Wilson SE, Liu JJ, Mohan RR. Stromal-epithelial interactions in the cornea. Prog Retin Eye Res 1999;18:293-309.
=ABSTRACT=
Confocal Microscopic Changes in the Cornea 10 Years After Photorefractive Keratectomy
Min Kyu Shin, MD, Gi Hong Koo, MD, Jong Soo Lee, MD, PhD
Department of Ophthalmology, School of Medicine, Pusan National University, Pusan, Korea
Purpose: The present study compares, using a new generation high‐resolution in vivo confocal microscope, the corneas of patients who underwent photorefractive keratectomy (PRK) 10 years previously with those of healthy persons.
Case Summary: A confocal microscope (Confoscan 4.0, Fortune Technology, Italy) was used to get the data from healthy volunteers and patients. Corneal cross‐sectional images of the epithelium, Bowman's layer, stromal layer (anterior, middle and posterior keratocyte), Descemet's membrane, and endothelium were compared. In PRK corneas, the superficial epithelium was nearly intact and the subbasal nerve plexus was visible, but some hyperreflective areas were also found in the nerve plexus.
Because of the absence of the Bowman's layer, some ECM and keratocytes were visualized in their optical section. Although anterior keratocytes showed uneven distribution with less cellularity, middle and posterior keratocytes looked unaffected.
Likewise, there were no differences in the endothelium between the two groups.
Conclusions: Ten years after PRK, the subbasal nerve plexus and anterior keratocytes showed histologic changes after corneal wound recovery.
J Korean Ophthalmol Soc 2009;50(2):303-307
Key Words: Confocal microscopy, Photorefractive keratectomy
Address reprint requests to Jong Soo Lee, MD, PhD
Department of Ophthalmology, Pusan National University Hospital
#1‐10 Ami‐dong, Seo‐gu, Pusan 602‐739, Korea
Tel: 82-51‐240‐7957, Fax: 82-51‐242‐7341, E-mail: [email protected]