1208
Laparoscopic Partial Nephrectomy without Renal Arterial Clamping
Hye Min Hong, Ill Young Seo, Joung Sik Rim
From the Department of Urology, Wonkwang University School of Medicine, Iksan, Korea
Purpose: Renal vascular clamping during a laparoscopic partial nephrec- tomy is a time-consuming procedure with a risk of renal ischemia. To study the feasibility of laparoscopic partial nephrectomy without renal arterial clamping, we compared the procedure with laparoscopic partial nephrectomy with vascular clamping.
Materials and Methods: Seventeen patients underwent laparoscopic partial nephrectomy without renal arterial clamping (group 1) from February 2004 to June 2008. The operative results were reviewed retrospectively and compared with those of 16 patients who underwent laparoscopic partial nephrectomy with arterial clamping (group 2). Patient characteristics did not differ significantly between the 2 groups. However, exophytic tumors were detected in 13 patients in group 1 and 3 patients in group 2 (p=0.001).
Scores on the preoperative aspects and dimensions used for an anatomical (PADUA) classification were 6.9 in group 1 and 7.7 in group 2 (p=0.037).
All surgeries by the transperitoneal approach were performed by a single surgeon.
Results: The mean operative times were 103 and 130 minutes in groups 1 and 2, respectively (p=0.312). The mean renal arterial clamping time of group 2 was 27.6 minutes (range, 20-42 minutes). The mean estimated blood loss was 327 ml in group 1 and 315 ml in group 2 (p=0.971). The mean postoperative change in the glomerular filtration rate was 20.11 ml/min/1.73 m2 in group 1 and 18.95 ml/min/1.73 m2 in group 2 (p=0.748). The mean times to postoperative initiation of ambulation and of oral intake were 1.6 and 1.7 days (p=0.486) and 1.3 and 1.6 days (p=0.811) in groups 1 and 2, respectively. The mean length of hospital stay was 7.4 and 7.9 days in groups 1 and 2, respectively (p=0.9). The mean tumor size was 2.1 cm (range, 1-7 cm) in group 1 and 3.3 cm (range, 1.5-9 cm) in group 2.
Conclusions: Laparoscopic partial nephrectomy without renal arterial clamping is feasible for a localized renal tumor. However, patients should be selected carefully, such as those with an exophytic tumor. (Korean J Urol 2009;50:1208-1212)
Key Words: Kidney neoplasms, Laparoscopy, Nephrectomy
Korean Journal of Urology Vol. 50 No. 12: 1208-1212, December 2009
DOI: 10.4111/kju.2009.50.12.1208
원광대학교 의과대학 비뇨기과학교실 홍혜민ㆍ서일영ㆍ임정식
Received:May 21, 2009 Accepted:November 6, 2009 Correspondence to: Ill Young Seo
Department of Urology, Wonkwang University School of Medicine, 344-2, Shinyong-dong, Iksan 570-711, Korea
TEL: 063-859-1333 FAX: 063-842-1455
E-mail: seraph@wonkwang.ac.kr
Ⓒ The Korean Urological Association, 2009
서 론
1991년 Clayman 등이 복강경 신절제술 성공을 보고 [1]한 이후 비뇨기과 영역의 복강경수술은 많은 발전을 이루고 있다. 신장암에 대한 표준 치료방법으로 복강경 근치적신
절제술이 선택되고 있으며, 크기가 작은 국소 신장암의 경 우에는 복강경 부분신절제술이 가능해졌다. 신기능을 보전 할 수 있는 부분신절제술은 근치적신절제술에 비하여 고도 의 기술을 필요로 하지만 지속적인 술기의 발전으로 가능 해졌으며, 최근에는 근치적신절제술과 비교하여 종양 조절 효과가 비슷한 것으로 보고되고 있다 [2,3].
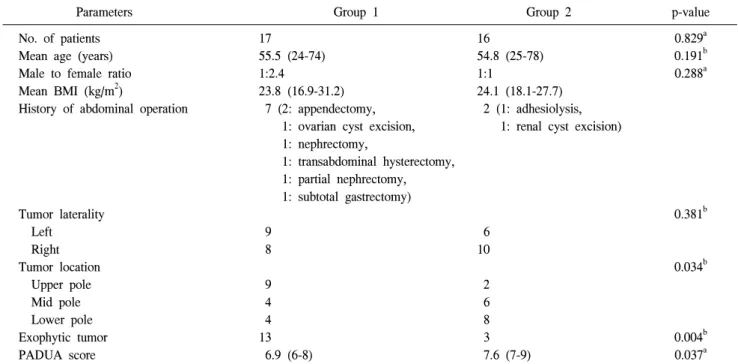
Table 1. Patient characteristics
Parameters Group 1 Group 2 p-value
No. of patients Mean age (years) Male to female ratio Mean BMI (kg/m2)
History of abdominal operation
Tumor laterality Left
Right Tumor location Upper pole Mid pole Lower pole Exophytic tumor PADUA score
17
55.5 (24-74) 1:2.4
23.8 (16.9-31.2) 7 (2: appendectomy,
1: ovarian cyst excision, 1: nephrectomy,
1: transabdominal hysterectomy, 1: partial nephrectomy, 1: subtotal gastrectomy) 9
8 9 4 4 13 6.9 (6-8)
16
54.8 (25-78) 1:1
24.1 (18.1-27.7) 2 (1: adhesiolysis,
1: renal cyst excision)
6 10 2 6 8 3 7.6 (7-9)
0.829a 0.191b 0.288a
0.381b
0.034b
0.004b 0.037a BMI: body mass index, PADUA: preoperative aspects and dimensions used for an anatomical classification, Group 1: laparoscopic partial nephrectomy without renal arterial clamping, Group 2: laparoscopic partial nephrectomy with renal arterial clamping, a: Mann-Whitney U test, b: Pearson chi-square test
복강경 부분신절제술은 덜 침습적인 수술방법으로, Winfield 등의 보고 [4] 이후 적응증이 확대되어 종양의 크 기가 작은 국한된 신암에 대해서도 시도되고 있다 [5,6]. 그 러나 아직까지 술기가 어려운 도전적인 수술법이며, 특히 수술 중 출혈을 방지하기 위해 일시적으로 신혈관을 결찰 하는 과정이 필요하다 [7]. 신동맥 및 정맥을 박리하기 위해 서는 수술 시간이 추가로 소요되며, 신동맥 결찰로 인한 신 허혈 위험이 있어 신동맥 결찰시간을 최소화해야하는 등 술기의 제한이 있다. 저자들은 신동맥을 결찰하지 않고 복 강경 부분신절제술을 시행하였으며, 그 결과를 신동맥을 결찰한 경우와 비교하여, 신혈관 결찰없이 시행한 복강경 부분신절제술의 가능성에 대해 알아보고자 하였다.
대상 및 방법
2004년 2월부터 2008년 6월까지 본원에서 복강경 부분신 절제술을 받은 환자 중에서 추적검사가 가능했던 34명 중 술 중 종물의 크기가 커서 수술 공간의 부족으로 개복을 하였던 한 명을 제외한 33명을 대상으로 하였으며, 모든 수 술은 단일 술자에 의해서 이루어졌다. 이 중 신동맥을 결찰 하지 않고 복강경 부분신절제술을 받은 환자는 17명 (1군) 이었으며, 신동맥을 결찰하고 수술을 받은 환자는 16명 (2 군)이었다. 평균 연령은 1군에서 55.5세 (24-74), 2군에서
54.8세 (25-78)이었고, 남녀비는 1:2.4와 1:1이었으며, 평균 체질량지수는 23.8 kg/m2 (16.9-31.2)와 24.1 kg/m2 (18.1- 27.7)로 두 군 간에 차이가 없었다. 제1군에서 7명, 2군에서 2명이 복부수술의 과거력이 있었다. 모든 환자에서 수술 전 에 복부 전산화단층촬영을 실시하여 종양의 위치 및 크기, 신혈관 개수 등을 확인하였다. 종양은 1군에서 좌측 9례, 우 측 8례였으며, 2군에서는 좌측 6례, 우측 10례였다. 종양의 위치는 1군에서 신 상극 8례, 중극 4례, 하극 5례였으며, 2군 에서 신 상극 3례, 중극 6례, 하극 7례로 두 군 간의 차이가 없었다. 복부 전산화단층촬영 사진에서 종양의 50% 이상이 신실질 밖에 위치한 경우를 돌출된 종양으로 정의하였고, 제1군에서 13명, 2군에서는 3명으로 신동맥을 결찰하지 않 은 군에서 돌출된 종양이 더 많았다 (p=0.001). 또한 Preoperative Aspects and Dimensions Used for An anatomical (PADUA) 분류방법을 이용하여 모든 환자를 분류하였으며 1군에서 6.9점 (6-8), 2군에서 7.6점 (7-9)으로 신동맥을 결찰 하지 않은 군에서 신동맥을 결찰하지 않은 군에서 돌출된 종양이 많아 점수가 더 낮았다 (p=0.037) (Table 1) [8].
복강경 부분신절제술은 모두 경복막접근법으로 이루어 졌다. 종물의 위치를 찾기 어려운 경우에는 복강경 초음파 를 이용하여 종물을 확인하였다. 제2군에서는 신문부를 박 리하여 신동맥과 정맥을 노출시킨 후 불독겸자를 이용하여 신동맥을 결찰하였다. 종양의 절제는 제1군의 경우 출혈을
Table 4. Difference in the glomerular filtration rate in patients who underwent partial nephrectomy
Group 1 Group 2 p-value
Difference of GFR between preoperation and POD1 (ml/min/1.73 m2) Difference of GFR between preoperation and last follow-up (ml/min/1.73 m2)
−18.95
−21.80
−20.11
−16.94
0.748 0.179 GFR: glomerular filtration rate, POD: postoperative day, Group 1: laparoscopic partial nephrectomy without renal arterial clamping, Group 2: laparoscopic partial nephrectomy with renal arterial clamping
Table 3. Pathologic results of renal tumors
Parameters Group 1 Group 2 p-value
Mean mass size (cm) Pathologic results RCC
AML Adenoma
Positive surgical margin
2.1 (1-7) 8 9 0 0
3.3 (1.2-9) 9
6 1 0
0.057a 0.743b
RCC: renal cell carcinoma, AML: angiomyolipoma, Group 1: laparoscopic partial nephrectomy without renal arterial clamping, Group 2:
laparoscopic partial nephrectomy with renal arterial clamping, a: Mann-Whitney U test, b: Pearson chi-square test Table 2. Operative results
Parameters Group 1 Group 2 p-value
Operation time (minutes) Estimated blood loss (cc)
Postoperative initiation of ambulation (days) Postoperative initiation of intake (days) Hospital stay (days)
103 (60-180) 327 (70-960)
1.6 (1-4) 1.3 (1-2) 7.4 (5-11)
130 (60-240) 315 (5-668)
1.7 (1-4) 1.6 (1-4) 7.9 (5-14)
0.312 0.971 0.486 0.811 0.9 Group 1: laparoscopic partial nephrectomy without renal arterial clamping, Group 2: laparoscopic partial nephrectomy with renal arterial clamping
방지하기 위해서 초음파메스 (SonoSurgⓇ, Olympus optical, Japan)를 이용하였고, 제2군의 경우에는 복강경 가위를 이 용하여 종물과 5 mm 이상 떨어진 경계부위를 절제하였다.
종양을 절제한 후 냉동생검은 시행하지 않았으며, 절제한 기저부를 추가로 절제하여 병리검사에 이용하였다. 절제된 조직을 복강경 주머니에 넣어 제거하였다. 절제부위의 출 혈은 argon beam 소작기, fibrin sealant (TissucolⓇ, Baxter AG, Austria), cellulose mesh (SurgicelⓇ, Ethicon Inc., USA) 등을 이용하여 조절하였으며, 손상된 집뇨계는 폴리머클립 (Hem-o-lokⓇ, Weck closure systems, USA)이 고정된 Vicryl 3-0사를 이용하여 연속 봉합하였고 신 실질 내에 흡수성 봉 합클립 (Lapra-TyⓇ, Ethicon Inc., USA)으로 매듭을 만들었 다. 피막을 포함한 신 실질은 Vicryl 2-0사와 흡수성 봉합클 립으로 봉합하였다.
두 군에서 수술 결과를 후향적으로 비교하여 분석하였다.
신 기능의 변화를 알기 위해 술 전, 술 후 1일째, 그리고 술 후 추적 관찰 중에 혈청 creatinine을 측정하였다. 술 전과
술 후 1일째, 그리고 술 후 추적 관찰 중의 사구체 여과율을 Modification of Diet in Renal Disease Study Group (MDRD) 연구의 공식인 GFR (in ml per minute per 1.73 m2)=186x sCr−1.154xage−0.203(x0.742 여성일 경우)를 이용하여 계산하였 다 [9,10]. 통계처리는 SPSS 12.0K for Windows 통계프로그 램을 이용하였고 Mann-Whitney U test와 Pearson chi-square test로 분석하였으며, p값이 0.05 미만인 경우 통계학적으로 유의한 것으로 판정하였다.
결 과
평균 수술시간은 1군에서 103분 (60-180), 2군에서 130분 (60-240)으로 신동맥을 결찰한 군에서 더 길었으나 통계학 적인 차이는 없었다 (p=0.312). 제2군에서 신동맥 결찰시간 은 평균 27.6분 (20-42)이었다. 두 군의 평균 출혈량은 327 cc와 315 cc로 통계적인 차이는 없었다 (p=0.971). 수술과 관 련된 합병증은 2군에서 2명 발생하였다. 한 명은 수술 중
간 손상이 발생하였으나 보전적인 치료로 치료되었고, 다 른 한 명은 술 후 수술 부위 탈장이 발생하여 외과에서 수 술 받았다.
수술 후 평균 보행개시일은 1군에서 1.6일, 2군에서 1.7일 이었고, 평균 식이개시일은 1.3일과 1.6일이었다 (p=0.486, 0.811). 평균 재원기간은 7.4일과 7.9일로 의의있는 차이는 없었다 (p=0.9) (Table 2). 적출된 조직의 병리검사에서 1군 의 경우 종양의 크기는 평균 2.1 cm (1-7)였으며, 신세포암 8례, 혈관지방종 9례였다. 제2군의 경우 종양의 크기는 평 균 3.3 cm (1.2-9)였으며, 신세포암 9례, 혈관지방종 6례, 선 종 1례였다. 두 군 모두에서 절제면 양성소견은 관찰되지 않았다 (Table 3).
제1군에서 수술 전과 수술 후 1일째의 사구체여과율의 차이는 −18.95 ml/min/1.73 m2였으며, 2군에서는 −20.11 ml/min/1.73 m2로 두 군 간의 의미 있는 차이는 없었다 (p=
0.748). 수술 전과 추적 관찰기간 중의 사구체여과율의 차이 도 1군에서 −21.80 ml/min/1.73 m2, 2군에서 −16.94 ml/min/
1.73 m2으로 의의있는 차이가 없었다 (p=0.179) (Table 4).
수술 후 평균 추적기간은 1군에서 26.1개월 (9-36), 2군에 서 31.3개월 (9-48)이었으며 추적기간 중 실시한 방사선검 사에서 종물의 재발은 없었다.
고 찰
복강경 부분신절제술은 신기능을 보전할 수 있는 장점이 있어 일측신을 가진 신장암 환자 혹은 양측 신기능에 장애 가 있는 환자에서 표준적 치료로 이용되고 있다 [5-7,11]. 최 근에는 그 적응증이 확대되어 크기가 작은 국소 신장암 환 자에서 성공적인 치료방법으로 보고되고 있다. 특히, 영상 의학의 발전으로 국소 신장암의 발견율이 높아지면서 복강 경 부분신절제술에 대한 관심은 높아지고 있으며 실제로 4 cm 이하의 신종양의 치료로 복강경 부분신절제술의 적용 이 증가하고 있는 추세이다.
복강경 부분신절제술의 술기 중 가장 중요한 부분 중 하 나가 지혈이다. 따라서 수술 중 출혈을 예방하기 위해서 일 반적으로 신혈관을 결찰하게 된다. Ramani 등의 연구에서 는 초기 복강경 부분신절제술을 시행받은 환자 200명의 합 병증을 조사하였으며, 조사 결과 39명의 환자에서 부작용 이 발생하였고, 그 중 신출혈이 21명으로 가장 큰 비중을 차지하였으며 이는 신동맥의 불충분한 결찰에서 기인한 것 이라고 보고하였다 [12]. Guillonneau 등은 신동맥를 결찰한 복강경 부분신절제술 환자군과 신동맥 결찰을 하지 않고 수술한 군을 비교하였으며 결찰한 군에서의 출혈량은 평균 270 cc였으나, 결찰하지 않은 군에서의 출혈량은 708 cc로
결찰하지 않은 군에서의 출혈량이 유의하게 많았다고 보고 하였다 [13].
그러나 신동맥 결찰과정에 수술 시간이 소요되며, 박리과 정 중에 신혈관이 손상될 수 있으며, 신혈관결찰 시간이 길 경우 신허혈이 발생할 수 있다 [14]. Desai 등은 70세 이상의 고령이나 술 전 크레아틴 수치가 1.5 mg/dl인 환자에서 30분 이상의 신동맥 결찰 시 술 후 신기능저하가 올 수 있다고 보 고하였으며 [14], Kobayashi 등도 비슷한 결과를 보고하였다 [15]. 따라서 신동맥 결찰을 시행한 복강경 부분신절제술에서 는 신동맥 결찰 후 30분 이내에 부분신절제술을 시행해야 하 는 시간의 제한이 있으며 고령의 환자나 술 전 신기능이 감소 된 환자에서 술 후 신기능 저하 가능성이 존재한다.
신허혈로 인한 신기능 감소를 줄이기 위해 여러 가지 냉 각요법들이 보고되었다. Landman 등이 처음 동물 모델에서 복강경 부분신절제술 시 신실질 냉각요법을 보고하였으며 [16], Janetschek 등은 신동맥으로 통과된 카테터에 냉각수 를 주사하며 수술한 부분신절제술 15례를 보고하였다 [17].
그러나 이런 방법들은 복강경 수술로 시행하기가 어렵고 신냉각효과도 만족스럽지 못하다.
따라서, 최근에는 신혈관을 결찰하지 않고 시행한 복강 경 부분신절제술이 보고되고 있다. 신동맥결찰 없이 시행 한 복강경 부분신절제술은 신동맥 결찰 후 시행한 수술에 비하여 술 후 허혈이 발생하지 않는 장점이 있으며, 종양의 크기가 작고 외부로 돌출된 경우엔 복강경 부분신절제술시 신동맥을 결찰하지 않고도 수술이 가능하였다. 또한 수술 결과에서 결찰한 경우와 의의있는 차이가 없었다. Ven- katesh 등은 신 밖으로 돌출된 종양에서 신동맥을 결찰한 군과 결찰하지 않은 군에서 합병증의 증가가 일어나지 않 았다고 보고하였다 [18]. Finley 등은 1 cm 미만의 신종물에 서 ‘샌드위치’ 방식으로 시행한 복강경 부분신절제술을 보 고하였으며 [19], Jeon과 Kim은 평균 2.3 cm의 신종양 환자 에서 신동맥 결찰없이 ‘샌드위치’ 방식으로 Floseal, Sur- gicel, Tisseel 등을 이용한 복강경 부분신절제술을 보고하였 다 [20]. Fogarty 등도 4 cm 이하의 신종양을 신동맥 결찰없 이 복강경 부분신절제술로 치료한 것을 보고하였다 [21].
저자들의 경우도 신동맥 결찰없이 복강경 부분신절제술 을 성공적으로 시행하였다. 결찰하지 않은 군과 비교할 때 기본적인 조건은 같았으나 결찰하지 않은 군에서 돌출된 종양의 빈도가 높았다. 그러나 수술 결과에서 수술 시간 및 출혈량 등에 의의있는 차이가 없었다. 즉 신장 밖으로 돌출 된 종양의 경우 신동맥 결찰없이도 부분신절제술이 가능함 을 알 수 있었다. 통계적인 차이는 없었지만, 복부수술의 과 거력이 있는 경우에 신문부 박리의 위험 때문에 상대적으 로 신동맥을 결찰하지 않은 경우가 더 많았던 것으로 추측
된다. 술기적인 문제로, 신동맥을 결찰하지 않은 경우 적절 한 지혈과 빠른 봉합을 위해서 종양을 절제할 때 초음파메 스를 이용하여 지혈을 하면서 조직을 절제하였다. 집뇨계 의 봉합은 폴리머클립을 이용하여 연속적으로 봉합하였고 흡수성클립으로 결찰하였으며, 신 실질의 봉합도 폴리머클 립을 이용하여 연속적으로 봉합하였다. 이 방법을 이용할 경우 신 실질을 압박하면서 빠르게 봉합할 수 있어 지혈 및 수술 시간 단축에 효과적이다 [21]. 수술 전후의 사구체 여과율은 환자 수술 후 금식과 혈액 손실량에 따른 체중 변화를 고려하여 MDRD 연구의 공식을 이용하여 계산하였 다. 수술 후 신기능의 변화에 대한 저자들의 결과, 신동맥을 결찰한 군과 비교하였을 때 유의한 차이가 없어 동맥결찰 시간이 짧다면 동맥결찰 유무가 신기능변화에 영향을 미치 지 않을 것으로 추측된다. 그러나 저자들의 신기능 평가방 법이 혈청 creatinine과 사구체 여과율 만을 이용하였으므로 분리 신기능을 완전히 평가하지는 못하였다.
결 론
국한된 신장 종양에 대해서 신동맥을 결찰하지 않고서도 복강경 부분신절제술이 가능하다. 특히, 신장 밖으로 종양 이 돌출된 경우 적용이 가능하다. 그러나 종양절제 후 지혈 및 봉합에 대한 적절한 술기가 필요하므로 복강경 수술에 대한 충분한 경험이 필요할 것으로 생각한다. 또한 수술 후 신기능의 변화에 대한 분리신기능 평가방법을 적용하기 위 해서 전향적인 연구가 필요할 것이다.
REFERENCES
1. Clayman RV, Kavoussi LR, Soper NJ, Dierks SM, Meretyk S, Darcy MD, et al. Laparoscopic nephrectomy: initial case report. J Urol 1991;146:278-82.
2. Fergany AF, Hafez KS, Novick AC. Long-term results of nephron sparing surgery for localized renal cell carcinoma:
10-years follwup. J Urol 2000;163:442-5.
3. Lerner SE, Hawkins CA, Blute ML, Grabner A, Wollan PC, Eickholt JT, et al. Disease outcome in patients with low stage renal cell carcinoma treated with nephron sparing or radical surgery. 1996. J Urol 2002;167:884-9.
4. Winfield HN, Donovan JF, Godet AS, Clayman RV. Laparo- scopic partial nephrectomy: initial case report for benign disease. J Endourol 1993;7:521-6.
5. Hong SH, Ryu KY, Yoo JS, Seo SI, Kim JC, Hwang TK.
Laparoscopic partial nephrectomy for the 4cm or less renal tumors. Korean J Urol 2006;47:1256-62.
6. Seo IY, Bae BJ, Rim JS. Early experience of laparoscopic partial nephrectomy for renal tumor. Korean J Urol 2007;
48:1-5.
7. Jeschke K, Peschel R, Wakonig J, Schellander L, Bartsch G, Henning K. Laparoscopic nephron-sparing surgery for renal tumors. Urology 2001;58:688-92.
8. Ficarra V, Novara G, Secco S, Macchi V, Porzionato A, De Caro R, et al. Preoperative aspects and dimensions used for an anatomical (PADUA) classification of renal tumors in patients who are candidates for nephron-sparing surgery. Eur Urol 2009;Epub ahead of print
9. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method to estimate glomerular filtration rate from serum creatinine: a new prediction equation.
Modification of Diet in Renal Disease Study Group. Ann Intern Med 1999;130:461-70.
10. Stevens LA, Coresh J, Greene T, Levey AS. Assessing kidney function--measured and estimated glomerular filtration rate. N Engl J Med 2006;354:2473-83.
11. Gill IS, Colombo JR Jr, Moinzadeh A, Finelli A, Ukimura O, Tucker K, et al. Laparoscopic partial nephrectomy in solitary kidney. J Urol 2006;175:454-8.
12. Ramani AP, Desai MM, Steinberg AP, Ng CS, Abreu SC, Kaouk JH, et al. Complications of laparoscopic partial ne- phrectomy in 200 cases. J Urol 2005;173:42-7.
13. Guillonneau B, Bermudez H, Gholami S, El Fettouh H, Gupta R, Adorno Rosa J, et al. Laparoscopic partial nephrectomy for renal tumor: single center experience comparing clamping and no clamping techniques of the renal vasculature. J Urol 2003;
169:483-6.
14. Desai MM, Gill IS, Ramani AP, Spaliviero M, Rybicki L, Kaouk JH. The impact of warm ischaemia on renal function after laparoscopic partial nephrectomy. BJU Int 2005;95:377-83.
15. Kobayashi Y, Usui Y, Shima M, Akio H, Miyakita H, Inatsuchi H, et al. Evaluation of renal function after laparo- scopic partial nephrectomy with renal scintigraphy using 99mtechnetium-mercaptoacetyltriglycine. Int J Urol 2006;13:
1371-4.
16. Landman J, Rehman J, Sundaram CP, Bhayani S, Monga M, Pattaras JG, et al. Renal hypothermia achieved by retrograde intracavitary saline perfusion. J Endourol 2002;16:445-9.
17. Janetschek G, Abdelmaksoud A, Bagheri F, Al-Zahrani H, Leeb K, Gschwendtner M. Laparoscopic partial nephrectomy in cold ischemia: renal artery perfusion. J Urol 2004;171:68-71.
18. Venkatesh R, Weld K, Ames CD, Figenshau SR, Sundaram CP, Andriole GL, et al. Laparoscopic partial nephrectomy for renal masses: effect of tumor location. Urology 2006;67:
1169-74.
19. Finley DS, Lee DI, Eichel L, Uribe CA, McDougall EM, Clayman RV. Fibrin glue-oxidized cellulose sandwich for laparoscopic wedge resection of small renal lesions. J Urol 2005;173:1477-81.
20. Jeon SS, Kim IY. Laparoscopic partial nephrectomy without hilar control. J Endourol 2008;22:1937-9.
21. Fogarty JD, Hafron JM, Hoenig DM, Ghavamian R. Laparo- scopic nephron-sparing surgery for the small exophytic renal mass. JSLS 2005;9:199-204.