대한소화기학회지 2006;48:19-24
서 론
Helicobacter pylori (H. pylori) 감염은 만성위염, 소화성 궤 양의 원인인자이며, 위선암과 점막연관림프조직형 위림프 종(gastric mucosa associated lymphoid tissue lymphoma)의 발
생과 밀접한 연관이 있다.1 또한, H. pylori의 치료는 궤양의 재발 억제뿐 아니라 위암 예방을 위해서도 필요하다.
현재 가장 많이 사용하고 있는 H. pylori 제균요법은 amo- xicillin, clarithromycin, metronidazole 혹은 tetracycline 중 2가 지 항생제와 프로톤 펌프 억제제(proton pump inhibitor, PPI)
Helicobacter pylori 제균치료에서 Levofloxacin 병합요법의 효과
포천중문의과대학교 분당차병원 소화기내과, 보건행정정보학부*
이지현․홍성표․권창일․편래현․이병석․송한얼․고광현․황성규․박필원․임규성․김세현*
The Efficacy of Levofloxacin Based Triple Therapy for Helicobacter pylori Eradication
Ji Hyun Lee, M.D., Sung Pyo Hong, M.D., Chang Il Kwon, M.D., Lea Hyun Phyun, M.D., Byoung Sok Lee, M.D., Han Ul Song, M.D., Kwang Hyun Ko, M.D.,
Seong Gyu Hwang, M.D., Pil Won Park, M.D., Kyu Sung Rim, M.D., and Sehyun Kim, Ph.D.*
Department of Internal Medicine, Department of Health Science*, Bundang CHA Hospital, Pochon CHA University College of Medicine, Seongnam, Korea
Background/Aims: The failure rates of first and second line therapies of Helicobacter pylori (H. pylori) eradi- cation range from 15 to 20%. This study was aimed to evaluate the efficacy and safety of levofloxacin based triple therapy compared with standard triple or quadruple therapy for H. pylori eradication in Korea. Methods:
We enrolled two hundred and sixty seven patients with presence of H. pylori infection. One hundred and forty- one patients were treated with levofloxacin based triple therapy (LAP; levofloxacin, amoxicillin, proton pump inhibitor; PPI), and 126 patients were treated with standard triple therapy (CAP; clarithromycin, amoxicillin, PPI).
We retreated the patients who had failed in H. pylori eradication with standard quadruple second-line therapy (MTPB; metronidazole, tetracycline, PPI, bismuth subcitrate) or levofloxacin based therapy (LAP or LCP; levo- floxacin, clarithromycin, PPI). Results: In first line therapy of H. pylori eradication, the eradication rates of levofloxacin based triple therapy and standard triple therapy were 69.8% and 74.0% respectively (p=0.52). In second-line therapy, the eradication rate of levofloxacin based triple therapy and standard quadruple therapy were 62.5% and 40.0% respectively (p=0.34). Conclusions: Levofloxacin based triple therapy is effective as standard regimen to eradicate H. pylori infection and is useful for an alternative rescue therapy as well. (Korean J Gastroenterol 2006;48:19-24)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Key Words: Helicobacter pylori; Levofloxacin; Eradication therapy
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 접수: 2005년 11월 25일, 승인: 2006년 5월 25일
연락처: 홍성표, 463-712, 경기도 성남시 분당구 야탑동 351 포천중문의대 분당차병원 소화기내과
Tel: (031) 780-5214, Fax: (031) 780-5219 E-mail: sphong@cha.ac.kr
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Correspondence to: Sung Pyo Hong, M.D.
Department of Internal Medicine, Bundang CHA Hospital, Pochon CHA University College of Medicine, 351 Yatap-dong, Bundang- gu, Seongnam 463-712, Korea
Tel: +82-31-780-5214, Fax: +82-31-780-5219 E-mail: sphong@cha.ac.kr
20 대한소화기학회지: 제48권 제1호, 2006
를 사용하는 삼제요법이다. 이 삼제요법의 제균율은 80-90%
로 보고되고 있으나,2 최근 이 요법의 제균율이 감소추세에 있다.3
1차 치료에 실패한 경우 2차 치료로서 Maastricht 2-2000 Consensus Report에서는 PPI, bismuth, tetracycline 및 metro- nidazole을 포함하는 사제요법을 추천하고 있지만 이의 제균 율도 70-80% 정도이다.4,5
제균율에 영향을 미치는 인자로는 항생제 내성, 성별, 연 령, 흡연, nonsteroidal anti-inflammatory drugs (NSAIDs) 복용 등이 있다. 제균율 감소는 항생제 내성, 특히 clarithromycin 과 metronidazole에 대한 내성 증가와 연관된다. Clarithromy- cin에 내성인 경우는 제균율에 대한 영향이 커서, 제균율이 0-50%로 현저히 감소한다.6,7
Levofloxacin은 광범위 fluoroquinolone 제제로, 최근 여러 연구에서 이를 포함한 삼제요법의 제균 성적이 우수하였 다.8-14 이번 연구에서는 우리나라에서 현재 사용하고 있는 1, 2차 병합요법과 levofloxacin을 포함한 병합요법의 제균율 을 비교하고자 하였다.
대상 및 방법
1. 대상
2004년 12월부터 2005년 9월까지 포천중문의대 분당차병 원 소화기내과에 내원하여 상부위장관 내시경 검사 중에 조 직검사나 신속요소분해효소검사(rapid urease test)로 H. pylori 감염 진단을 받은 소화성 궤양, 장형화생을 동반한 만성위 축성위염, 선종 환자, 위암의 가족력이 있는 만성위염 환자 와 제균치료를 원하는 환자 267명을 대상으로 하였다.
2. 방법
1) H. pylori 제균 방법
141명은 1차 제균치료로 levofloxacin 병합요법을 시행 받 았고, 126명은 기존 PPI 삼제요법을 시행 받았다. Levofloxa- cin 병합요법은 levofloxacin 200 mg bid, amoxicillin 1.0 g bid, rabeprazole 20 mg bid를 7일간 투여하였고(LAP), PPI 삼제요 법은 clarithromycin 500 mg bid, amoxicillin 1.0 g bid, rabe- prazole 20 mg bid를 7일간 투여하였다(CAP). 1차 제균치료 에 실패한 환자들에 대해서는 2차 제균치료로 사제요법 또 는 levofloxacin 병합요법을 7일간 시행하였다. 사제요법은 metronidazole 500 mg bid, tetracycline 1.0 g bid, rabeprazole 20 mg bid, bismuth subcitrate 240 mg bid를 7일간 투여하였 고(MTPB), levofloxacin 병합요법은 1차 치료로 CAP 삼제요 법을 시행 받았던 환자들에서는 LAP 삼제요법을, 1차 치료 로 LAP 삼제요법을 시행 받았던 환자들에서는 levofloxacin
200 mg bid, clarithromycin 500 mg bid, rabeprazole 20 mg bid 를 7일 간 투여하였다(LCP). 치료군 선정은 의사별로 무작 위로 배정하였다. H. pylori 제균 판정은 제균요법 종료 후 최소 4주 이상 지난 후 요소호기검사를 시행하여 확인하였 고, 위궤양 등으로 추적 내시경 검사를 한 경우는 요소호기 검사와 조직검사가 모두 음성인 경우에 제균된 것으로 판정 하였다.
2) 통계 분석
제균율 분석을 위해 intention to treat (ITT) 분석과 per pro- tocol (PP) 분석을 시행하였다. 각 군 간의 성별, 기저질환의 비교를 위해 chi-square test를 시행하였고, 군 간 제균율과 연령 비교를 위해 t-test와 Mann Whitney U test를 시행하였 다. 유의성 검정은 p값이 0.05 미만일 때 통계적인 유의성이 있는 것으로 판정하였다.
결 과
1. 환자군의 임상 특징
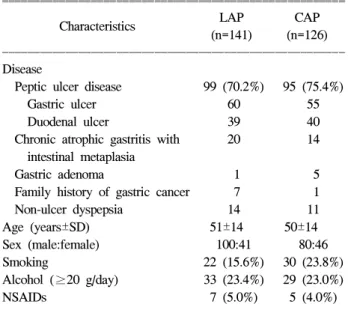
대상 환자는 총 267명이었고, 위궤양 115명, 십이지장궤양 79명, 장형화생을 동반한 위축성위염 34명, 선종 6명, 위암 가족력이 있는 만성위염 8명, 치료를 원한 기능성 소화불량 증 환자 25명이었다. 1차 제균치료 후 제균 여부가 확인된 환자는 LAP 삼제요법을 시행 받은 환자 141명 중 106명
Table 1. Characteristics of the Patients
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
LAP CAP
Characteristics
(n=141) (n=126) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Disease
Peptic ulcer disease 99 (70.2%) 95 (75.4%)
Gastric ulcer 60 55
Duodenal ulcer 39 40
Chronic atrophic gastritis with 20 14 intestinal metaplasia
Gastric adenoma 1 5
Family history of gastric cancer 7 1 Non-ulcer dyspepsia 14 11 Age (years±SD) 51±14 50±14 Sex (male:female) 100:41 80:46 Smoking 22 (15.6%) 30 (23.8%) Alcohol (≥20 g/day) 33 (23.4%) 29 (23.0%)
NSAIDs 7 (5.0%) 5 (4.0%)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ LAP, levofloxacin+amoxicillin+PPI; CAP, clarithromycin+amoxi- cillin+PPI; PPI, proton pump inhibitor; NSAIDs, non-steroidal anti-inflammatory drugs.
이지현 외 10인. Helicobacter pylori 제균치료에서 Levofloxacin 병합요법의 효과 21
(75.2%), CAP 삼제요법을 시행 받은 환자는 126명 중 96명 (76.2%)이었다. 양 군은 성별, 연령, 대상질환, 흡연력, 음주 력, NSAIDs 복용력에서 차이를 보이지 않았다(Table 1).
2. 제균 치료 성적
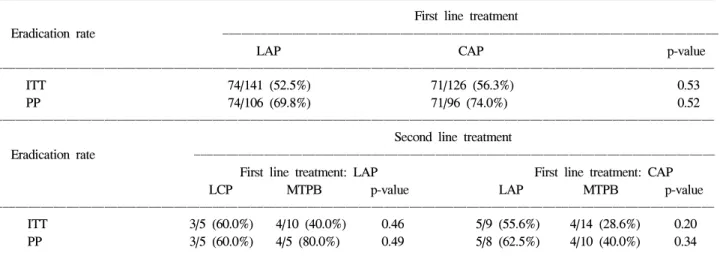
1차 LAP군의 제균율은 ITT 분석에서 52.5%, PP 분석에서 69.8%로 나타났고, CAP군의 제균율은 ITT 분석에서 56.3%, PP 분석에서 74.0%로 나타났으며 이들 사이에 통계적인 차 이는 보이지 않았다(p=0.53, p=0.52).
1차 LAP군에서 제균에 실패한 환자는 32명(30.2%)이었으 며, 2차 제균치료를 위해 환자들은 무작위 배정되었으나 이 들 중 17명에서는 추적관찰이 이루어지지 않았고 15명에 대 하여 2차 제균치료가 확인되었다. 5명에서 2차 LCP 삼제요 법이, 10명에서 MTPB 사제요법이 시행되었다. LCP군에서 5명 중 3명이 제균에 성공하여, 제균율은 ITT 분석과 PP 분 석에서 모두 60.0%로 나타났다. MTPB군에서는 10명 중 5명 에서 추적관찰이 이루어지지 않았고, 제균 여부를 확인할 수 있었던 5명 중 4명이 제균에 성공하여 ITT 분석과 PP 분 석에서 제균율은 각각 40.0%, 80.0%로 나타났다. LCP군과 MTPB군의 제균율은 ITT와 PP 분석 모두 통계적인 차이가 없었다(p=0.46, p=0.49).
1차 CAP군에서 제균에 실패한 환자는 25명(26.0%)이었으 며, 이들 중 2명에서 추적관찰이 이루어지지 않았고, 23명에
대하여 2차 제균치료를 시행하였다. 이들 중 9명은 LAP 삼 제 요법, 14명은 MTPB 사제요법을 시행받았다. 2차 LAP군 에서 1명에 대해 추적관찰이 이루어지지 않았고, 제균 여부 를 확인할 수 있었던 8명 중 5명이 제균에 성공하여 ITT 분 석과 PP 분석에서 제균율은 각각 55.6%, 62.5%였다. MTPB 군에서 4명은 추적관찰은 하지 않았고, 제균 여부를 확인할 수 있었던 10명 중 4명이 제균에 성공하여 ITT 분석과 PP 분석에서 제균율은 각각 28.6%, 40.0%였다. 2차 LAP군과 MTPB군의 제균율 역시 ITT와 PP 분석 모두에서 유의한 차 이는 없었다(p= 0.20, p=0.34)(Fig. 1, Table 2).
3. 유순도와 부작용
추적관찰이 가능했던 환자들에서 치료 중 탈락은 양 군 모두에서 없었고, 부작용도 LAP군에서 1.4%, CAP군에서 4.0%로 큰 차이는 없었다(Table 3).
고 찰
현재 가장 널리 사용하고 있는 H. pylori의 1차 제균요법 은 clarithromycin, amoxicilline과 PPI를 포함하는 삼제요법으 로, 이의 제균율은 80-90%이나,2 2003년 보고된 국내의 연구 에서 75%로 제균율이 낮아졌다.3 이번 연구에서도 CAP 삼 제요법의 제균율은 74%로 이전의 보고들과 비교하였을 때 Fig. 1. Overview of the treatment. Eradication rates of each regimen were illustrated (per protocol analysis).
LAP, levofloxacin+amoxicillin+PPI; CAP, clarithromycin+amoxicillin+PPI; LCP, levofloxacin+clarithromycin+PPI; MTPB, metronidazole+tetracycline+PPI+bismuth; PPI, proton pump inhibitor; F/u, follow up.
22 The Korean Journal of Gastroenterology: Vol. 48, No. 1, 2006
낮게 나타나 최근 CAP 삼제요법의 제균율이 감소하고 있을 가능성이 있다. 제균 실패의 가장 흔한 원인은 항생제 내성 으로, 특히 clarithromycin 내성인 경우 제균율이 유의하게 감소한다.3-7,15 국내에서 clarithromycin에 대한 H. pylori 내성 률은 1994년부터 1999년 사이는 5.9%였으나,16 2003년에는 13.8%로 증가하는 경향이다.3
대한 Helicobacter 연구회에서는 1차 치료가 실패한 경우, 2차 제균요법으로 metronidazole, tetracycline, PPI, bismuth 사 제요법(MTPB)을 권장하고 있으며,17 이의 제균율은 70-80%이 다.5 이번 연구에서 MTPB 사제요법의 제균율은 1차 요법으 로 CAP 삼제요법을 사용한 경우, 환자수가 적었지만 40.0%
로 기존의 보고들에 비해 낮았다. Metronidazole에 대한 H.
pylori의 내성율도 증가 추세를 보이고 있어, 1994년부터 1999년 사이의 metronidazole 내성균주는 40.5%였으나,16 2003 년에는 66.2%로3 증가하였다. Metronidzole 내성이 제균율에 미치는 영향은 명확하지는 않지만, 내성 균주에서 제균율이
감소하는 경향을 보이고,18-20 내성률이 증가하는 경향이므로 MTPB의 제균율도 감소하고 있을 가능성이 있다.
기존의 항생제 내성 증가에 따라, clarithromycin이나 metro- nidazole을 대체하는 항생제로서 levofloxacin,8-13 moxifloxa- cin,21-25 rifabutin26,27 등이 연구되고 있다. 이들 중 rifabutin은 주로 1차 또는 2차 제균치료에 실패한 환자들에 대한 구제 요법으로 연구되었으며, 그 결과 60-79% 정도의 제균율을 보였고, 현재까지는 rifabutin에 대한 내성을 갖는 H. pylori 균주가 보고된 바 없어28 기존 제균요법에 실패한 환자들에 대한 구제요법으로서 효과가 크다. 그러나 rifabutin은 가격 이 비싸고, 백혈구 감소증, 혈소판 감소증을 포함한 골수 독 성 등의 심각한 부작용이 발생할 수 있으며,2 우리나라와 같 이 결핵 유병률이 높은 지역에서 사용할 경우 다약제 내성 결핵균의 발생 가능성이 높다는 단점이 있다.
Moxifloxacin은 최근 개발된 광범위 fluoroquinolone 제제 로, 국외 연구에 의하면 1차 제균 치료 시 moxifloxacin을 포 함한 삼제요법의 제균율이 90%까지도 보고되었다.22,23 국내 에서는 1, 2차 제균요법에 실패한 환자들을 대상으로 한 연 구에서 3차 구제요법으로 투여했을 경우 88.9%의 제균율을 보였으나 대상 환자가 10명으로 적었고,21 2차 제균요법으로 47명에 대해 시행한 연구에서는 46.5%의 낮은 제균율이 보 고되었다.29 Levofloxacin은 광범위 fluoroquinolone 제제로 in vitro에서 H. pylori에 대한 활성이 높으며, 내성률이 1.9%로 매우 낮다.30 1차 제균치료에서 levofloxacin 포함 병합요법의 제균율은 90% 내외로 보고되었으며,8,14 2차 제균요법으로는 63-94%의 제균율이 보고되었다.9-13
이번 연구에서는 levofloxacin 포함 병합요법을 기존의 1, 2차 제균요법과 비교하였다. 그 결과 1차 제균치료 제균율 Table 2. Comparison of Helicobacter pylori Eradication Rates by Different Treatment Regimens
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
First line treatment
Eradication rate ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
LAP CAP p-value
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
ITT 74/141 (52.5%) 71/126 (56.3%) 0.53
PP 74/106 (69.8%) 71/96 (74.0%) 0.52
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Second line treatment
Eradication rate ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ First line treatment: LAP First line treatment: CAP
LCP MTPB p-value LAP MTPB p-value
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ ITT 3/5 (60.0%) 4/10 (40.0%) 0.46 5/9 (55.6%) 4/14 (28.6%) 0.20 PP 3/5 (60.0%) 4/5 (80.0%) 0.49 5/8 (62.5%) 4/10 (40.0%) 0.34 ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ LAP, levofloxacin+amoxicillin+PPI; CAP, clarithromycin+amoxicillin+PPI; LCP, levofloxacin+clarithromycin+PPI; MTPB, metronidazole+tetracycline+PPI+bismuth; PPI, proton pump inhibitor; ITT, intention to treat; PP, per protocol.
Table 3. The Adverse Events in Each Treatment Regimen
ꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧꠧ
Adverse events LAP CAP
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Abdominal pain 1 -
Abdominal bloating - 2
Dyspepsia - 2
Nausea 1 -
Diarrhea - 1
Total 2/141 (1.4%) 5/126 (4.0%) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ LAP, levofloxacin+amoxicillin+PPI; CAP, clarithromycin+
amoxicillin+PPI; PPI, proton pump inhibitor.
Lee JH, et al. The Efficacy of Levofloxacin Based Triple Therapy for Helicobacter pylori Eradication 23
은 per protocol 분석에서 LAP군 69.8%, CAP군 74.0%로 양 군 간에 통계적인 차이를 보이지 않았고, 1차 제균요법으로 CAP 삼제요법을 시행 받고 제균에 실패한 환자들에서 2차 치료의 제균율은 per protocol 분석에서 LAP군 62.5%, MTPB 군 40.0%로, LAP군의 제균율이 높게 나타났으나 통계적인 차이는 보이지 않았다.
Levofloxacin 포함 병합요법의 제균율은 다른 연구들에서 도 다양하게 보고되고 있고, 투여 기간에 따른 제균율의 차 이도 있으며, 7일 투여 시 보다 10일 투여 시 제균율이 유의 하게 높았다.31 이번 연구에서 LAP 삼제요법의 제균율은 CAP 삼제요법, MTPB 사제요법과 유사하였는데, 투여 용량 이 하루에 400 mg으로 다른 연구들의 500 mg보다 100 mg 이 적었고, 투여 기간이 7일이었으므로, 용량 또는 기간을 늘린다면 제균율이 보다 증가할 수 있을 것으로 생각되나 앞으로 이에 대한 추가 연구가 필요하다. 또한 2차 제균치 료에 있어서는 대상 환자 수가 적었으므로, 더 많은 환자들 을 대상으로 한 연구가 필요하다. 추가로 clarithromycin과 levofloxacin의 약가를 비교했을 때, levofloxacin이 clarithro- mycin의 60% 정도로 저렴하므로 비용 효과적인 측면에서도 유용할 것으로 생각한다.
결론으로, H. pylori 제균치료에서 levofloxacin 포함 삼제 병합요법은 기존의 H. pylori 1차 병합요법과 제균율에 있어 서 유사하며, 부작용과 환자 유순도에서도 차이를 보이지 않았다. 2차 병합요법에서는 환자 수가 적어 제한점이 있으 나, 기존의 사제요법과 제균율에서 큰 차이를 보이지 않았 다. 따라서 levofloxacin 포함 병합요법은 H. pylori 1차 제균 치료에서 효과적이며, 기존 제균치료에 실패한 환자에서 구 제요법으로서의 가능성이 높아 추가 연구가 필요하다.
요 약
목적: 현재 사용하는 Helicobacter pylori (H. pylori) 1차 제 균 요법은 치료실패가 15-20%이며, 주로 항생제 내성과 연 관된다. 이번 연구에서는 H. pylori 제균치료에서 기존 1, 2 차 제균요법과 levofloxacin을 포함한 병합요법의 효과를 비 교하고자 하였다. 대상 및 방법: 2004년 12월부터 2005년 9 월까지 H. pylori 양성 진단을 받고 제균 치료를 받은 267명 의 환자들을 대상으로 무작위 배정하여, 141명에서 levoflo- xacin 포함 병합요법을, 126명에서 기존 PPI 삼제요법을 시 행하였다. Levofloxacin 병합요법은 levofloxacin 200 mg bid, amoxicillin 1.0 g bid, rabeprazole 20 mg bid를 7일간 투여하 였고(LAP), PPI 삼제요법은 clarithromycin 500 mg bid, amo- xicillin 1.0 g bid, rabeprazole 20 mg bid를 7일간 투여하였다 (CAP). 이들 중 1차 제균 치료에 실패한 환자들은 2차 치료 로 levofloxacin 병합요법 또는 사제요법을 시행 받았다. 사
제요법은 metronidazole 500 mg bid, tetracycline 1.0 g bid, rabeprazole 20 mg bid, bismuth subcitrate 240 mg bid를 7일간 투여하였고(MTPB), levofloxacin 병합요법은 1차 치료로 CAP 삼제요법을 시행 받았던 환자들에서는 LAP 삼제요법 을, 1차 치료로 LAP 삼제요법을 시행 받았던 환자들에서는 levofloxacin 200 mg bid, clarithromycin 500 mg bid, rabepra- zole 20 mg bid를 7일간 투여하였다(LCP). 제균치료가 끝나 고 최소 4주 이상 지난 후 요소호기검사로 제균 여부를 확 인하였다. 결과: 양 군에서 성별, 연령, 진단, 흡연, 음주 등 의 차이는 보이지 않았다. LAP군과 CAP군의 제균율은 per protocol 분석에서 69.8%와 74.0%로 통계적인 차이를 보이 지 않았고, 2차 제균치료의 제균율은 LAP군과 MTPB군에서 각각 62.5%와 40.0%로 LAP군의 제균율이 높게 나타났으나 통계적인 차이는 없었다(p=0.52, p=0.34). 치료 중 약물부작 용에 의한 탈락은 양 군 모두에서 없었고, 부작용도 LAP군 에서 1.4%, CAP군에서 4.0%로 차이를 보이지 않았다. 성별, 음주, 흡연 여부는 제균율에 영향을 미치지 않았고, 기저 질 환에 따른 제균율의 차이도 없었다. 결론: Levofloxacin 포 함 병합요법은 기존의 H. pylori 1차 제균요법과 제균율에서 유사하며, 부작용과 환자 유순도에서도 차이가 없었다. 따 라서 levofloxacin 포함 병합요법은 H. pylori 1차 제균치료에 있어 효과적이며, 기존의 제균치료에 실패한 환자에서 구제 요법으로서의 가능성이 있어 추가 연구가 필요하다.
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ 색인단어: Helicobacter pylori, Levofloxacin, 제균요법
참고문헌
1. Suerbaum S, Michetti P. Helicobacter pylori infection. N Engl J Med 2002;347:1175-1186.
2. Kim JG. Treatment of Helicobacter pylori infection. Korean J Gastroenterol 2005;46:172-180.
3. Kim JM, Kim JS, Jung HC, Kim NY, Song IS. Antibiotic resistance of Helicobacter pylori isolated from Korean pa- tients in 2003. Korean J Gastroenterol 2004;44:126-135.
4. Malfertheiner P, Megraud F, O'Morain C, et al. Current concepts in the management of Helicobacter pylori infection- the Maastricht 2-2000 Consensus Report. Aliment Pharmacol Ther 2002;16:167-180.
5. Gisbert JP, Pajares JM. Review article: Helicobacter pylori
“rescue” regimen when proton pump inhibitor-based triple therapies fail. Aliment Pharmacol Ther 2002;16:1047-1057.
6. Lamouliatte H, Samoyeau R, De Mascarel A, Megraud F.
Double vs. single dose of pantoprazole in combination with clarithromycin and amoxycillin for 7 days, in eradication of Helicobacter pylori in patients with non-ulcer dyspepsia.
24 대한소화기학회지: 제48권 제1호, 2006
Aliment Pharmacol Ther 1999;13:1523-1530.
7. Wurzer H, Rodrigo L, Stamler D, et al. Short course therapy with amoxycillin-clarithromycin triple therapy for 10 days (ACT-10) eradicate Helicobacter pylori and heals duodenal ulcer. ACT-10 Study Group. Aliment Pharmacol Ther 1997;
11:943-952.
8. Cammarota G, Cianci R, Cannizzaro O, et al. Efficacy of two one-week rabeprazole/levofloxacin-based triple therapies for Helicobacter pylori infection. Aliment Pharmacol Ther 2000;
14:1339-1343.
9. Bilardi C, Dulbecco P, Zentilin P, et al. A 10-day levoflo- xacin based therapy in patients with resistant Helicobacter pylori infection: a controlled trial. Clin Gastroenterol Hepatol 2004;2:997-1002.
10. Nista EC, Candelli M, Cremonini F, et al. Levofloxacin- based triple therapy vs. quadruple therapy in second-line Heli- cobacter pylori treatment: a randomized trial. Aliment Phar- macol Ther 2003;18:627-633.
11. Perri F, Festa V, Merla A, Barberani F, Pilotto A, Andriulli A. Randomized study of different ‘second-line’ therapies for Helicobacter pylori infection after failure of the standard
‘Maastricht triple therapy'. Aliment Pharmacol Ther 2003;18:
815-820.
12. Watanabe Y, Aoyama N, Shirasaka D, et al. Levofloxacin based triple therapy as a second-line treatment after failure of Helicobacter pylori eradication with standard triple therapy.
Dig Liver Dis 2003;35:711-715.
13. Zullo A, Hassan C, De Francesco V, et al. A third line levo- floxacin-base rescue therapy for Helicobacter pylori eradica- tion. Dig Liver Dis 2003;35:232-236.
14. Gasbarrini A, Nista EC, Candelli M, et al. Levofloxacin based triple therapy in first line treatment for H. pylori eradication:
update. Gastroenterology 2005;128(abstr):63A.
15. Nam SW, Roe IH, Kim SB, et al. Detection of clarithro- mycin-resistant Helicobacter pylori by polymerase chain reac- tion. Korean J Gastroenterol 2000;36:450-456.
16. Kim JJ, Reddy R, Lee M, et al. Analysis of metronidazole, clarithromycin and tetracycline resistance of Helicobacter pylori isolates from Korea. J Antimicrob Chemother 2001;47:
459-461.
17. Korean H. pylori study Group. Diagnosis and treatment of Helicobacter pylori infection in Korea. Korean J Gastro- enterol 1998;32:275-289.
18. Kim NY, Lim CN, Lim SH, et al. Establishment of an Heli- cobacter pylori-eradication regimen in consideration of drug
recrudescence and reinfection rate of H. pylori. Korean J Med resistance, 1999;56:279-291.
19. Mun GH, Hahm JS, Ryu KH, et al. Metronidazole resistance and the eradication of Helicobacter pylori. Korean J Gastro- intest Endosc 1998;18:847-852.
20. Yoo HM, Lee YC, Lee SI, Moon YM, Kang JK, Park IS.
Effect of omeprazole quadruple therapy on eradication of Helicobacter pylori. Korean J Gastroenterol 1999;33:473-481.
21. Cheon JH, Kim NY, Lee DH, et al. Trial of moxifloxacin- containing triple therapy after initial and second-line treatment failures for Helicobacter pylori infection. Korean J Gastro- enterol 2005;45:111-117.
22. Di Caro S, Ojetti V, Zocco MA, et al. Mono, dual and triple moxifloxacin based therapies for Helicobacter pylori eradica- tion. Aliment Pharmacol Ther 2002;16:527-532.
23. Nista EC, Carloni E, Candelli M, et al. Moxifloxacin-based anti-Helicobacter pylori therapy. Helicobacter 2003;8(abstr):
462A-463A.
24. Nista EC, Cazzato IA, Franceschi F, et al. First-line treatment for eradication: new moxifloxacin based strategies. Gastro- enterology 2003;124(abstr):359A.
25. Nista EC, Candelli M, Zocco MA, et al. Moxifloxacin-based strategies for first-line treatment of Helicobacter pylori infec- tion. Aliment Pharmacol Ther 2005;21:1241-1247.
26. Gisbert JP, Calvet X, Bujanda L, Marcos S, Gisbert JL, Pajares JM. ‘Rescue' therapy with rifabutin after multiple Heli- cobacter pylori treatment failures. Helicobacter 2003;8:90-94.
27. Perri F, Festa V, Clemente R, Quitadamo M, Andriulli A.
Rifabutin-based ‘rescue therapy' for Helicobacter pylori in- fected patients after failure of standard regimens. Aliment Phar- macol Ther 2000;14:311-316.
28. Heep M, Beck D, Bayerdorffer E, Lehn N. Rifampin and rifabutin resistance mechanism in Helicobacter pylori. Anti- microb Agents Chemother 1999;43:1497-1499.
29. Chung SJ, Lee DH, Kim NY, et al. Efficacy of moxifloxacin- rabeprazole-amoxicillin triple therapy as the second-line treat- ment for Helicobacter pylori infection in Korea: preliminary report. J Gastroenterol Hepatol 2005;20(abstr):163A-164A.
30. Zou J, Yang ZX, Qin ZM. Laboratory and clinical study of levofloxacin against Helicobacter pylori. Zhonbua Yi Xue Za Zhi 2003;83:1777-1781.
31. Saad R, Schoenfeld P, Kim HM, Che WD. Levofloxacin triple or PPI quadruple salvage therapy for persistent Helico- bacter pylori infection: results of a systematic review. Gas- troenterology 2005;128(abstr):64A.