대장정격 및 승격 자침이 정상 성인의 맥파에 미치는 영향 비교 연구※
조은, 이현*
대전대학교 한의과대학 침구의학교실
[Abstract]
The Effects of Sa-Am Acupuncture on Radial Pulse in Healthy Subjects:
A Comparative Study of Large Intestine Tonifying and Sedating※ Eun Cho and Hyun Lee*
Department of Acupuncture & Moxibustion Medicine, College of Korean Medicine, Daejeon University
Objectives : The purpose of this study is to find parameters to compare the effects of Sa-Am acupuncture with large intestine tonifying and sedating on radial pulse in healthy subjects.
Methods : Sixty healthy subjects participated in this study, divided into large intestine tonifying acupuncture group, large intestine sedating acupuncture group and control group. Radial pulse was measured by 3 dimensional pulse imaging system(DMP-3000) before, right after, 30 minutes after and 60 minutes after acupuncture at Cun, Guan, and Chi in the acupuncture group and in the control group at the same time points.
Results :
1. Angle of main peak and magnitude of fourier component significantly changed by integrated analysis of Cun, Guan and Chi.
2. Amplitude of H1, Pulse Power volume / min, elasticity, AIx / HR, Frequency and magnitude of fourier component significantly changed by analysis of Cun, Guan, and Chi.
Conclusions : The effect of Sa-Am acupuncture with large intestine tonifying and sedating in healthy human may be observed on time, amplitude, pulse area, augmentation index and fourier components parameters. The parameters analysed in this study may be used to differentiate the effects between Sa-Am acupuncture with large intestine tonifying and sedating on radial pulse. Further studies on the effects of Sa-Am acupuncture using radial pulse are needed.
Key words :
Sa-Am acupuncture with large intestine tonifying;
Sa-Am acupuncture with large intestine sedating;
Radial pulse;
CunGuan and Chi; 3 dimentional pulse
imaging system
Received : 2014. 08. 10.
Revised : 2014. 08.22.
Accepted : 2014. 08.22.
On-line : 2014. 09.20.
✱ Corresponding author : Department of Acupuncture & Moxibustion Medicine, Cheonan Oriental Hospital of Deajeon University, 4, Notaesan-ro, Seobuk-gu, Cheonan-si, Chungcheongnam-do, 331-958, Republic of Korea
Tel : +82-41-521-7550 E-mail : [email protected]
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
The Acupuncture is the Journal of Korean Acupuncture & Moxibustion Medicine Society. (http://www.TheAcupuncture.org) Copyright © 2014 KAMMS. Korean Acupuncture & Moxibustion Medicine Society. All rights reserved.
Ⅰ. 서 론
脈診은 한의학의 중요 진단법 중 하나로 四診 중 切診에 속하며, 脈動의 상태를 관찰하여 병의 원인, 진퇴 및 예후 와 관련 臟腑의 상태를 종합적으로 판단하는 의의가 있다.
그 진단 부위에 따라서 ≪黃帝內經≫에는 臟腑經脈遍診法, 三部九候法, 人迎寸口對比診, 獨取寸口脈法 등이 존재하며, 후세에 이르면서 寸口脈法이 주로 사용되어 인체 내부의 병 변을 관찰하였다1,2).
寸口脈法은 손목 요골동맥을 측정 대상으로 하여 요골 경 상돌기(styloid process)근처 高骨 부위를 關이라 칭하며, 그 좌우를 寸과 尺이라 칭한다. 각 위치에 脈象 및 病脈 유 무에 따라 병이 어느 經脈과 臟腑에 있는가에 대한 해석을 내리기도 한다3.4).
脈診은 현대의학에 비해 객관성과 재현성이 부족하여 이 러한 맥진 데이터의 객관화와 정량화를 위한 맥파의 측정 과 이를 이용하여 환자의 건강상태를 진단하기 위한 노력 이 필요하다5). 현재 이를 위해 맥파에 대한 다양한 연구가 진행되고 있으며6,7), 맥박을 측정하여 분석하는 다양한 맥 진기가 개발되어 임상에서 활용되고 있다8).
舍巖鍼法은 木ㆍ火ㆍ土ㆍ金ㆍ水 五兪穴을 선택하여 自經 補瀉 원칙에 더하여 他經補瀉法을 응용한 것으로, 그 원리 는 ‘虛則補其母, 實則瀉其子’의 원칙으로 五行의 相生, 相克 관계에 입각하여 正·勝格의 처방을 통해 經絡臟腑간 氣血의 虛實과 盛衰를 조정하여 平衡상태로 회복하게 하는 침법이다9).
舍巖鍼法에 대한 연구로는 문헌적 연구가 대부분인데10,11), 다양한 질환에 대한 증례 보고12-14) 등이 이루어지고 있으 며, 최근 들어 임상시험 연구가 활발히 진행되고 있다15,16). 이 중 자침 후 맥파 변화에 대한 연구17-21)가 이루어지고 있 었으나, 아직까지 舍巖鍼法의 正格과 勝格 자침 후 맥파 변 화를 비교한 연구는 없었다. 이에 저자는 만 20~39세까지 의 정상 성인 지원자에게 大腸正格과 大腸勝格 자침 이후 맥 파분석기로 맥파의 변화를 비교 분석한 결과 약간의 지견 을 얻었기에 이를 보고하는 바이다.
Ⅱ. 방 법
1. 대상선정
1) 대상자 모집
대상자는 대전대학교 교내ㆍ외 광고물을 통하여 2012년
11월 19일부터 2012년 12월 30일까지 공개 모집하였다. 시 험에 참가한 지원자는 시험에 대해 상세한 설명을 들은 후 서면 동의서에 서명하고 시험에 임하였으며 대상자들에 관 한 정보 수집 및 검사는 대전대학교 경락경혈학교실에서 시행하였다. 본 임상시험은 각 군의 대상자들의 동질성에 차이가 없었으며(Table 1), 헬싱키 선언에 근거한 대전대 학교 천안병원 산하 윤리위원회 승인 아래 실시하였다 (P2012-4-1).
2) 선정기준 및 제외기준 (1) 선정기준
제외기준에 해당되지 않으며, 최근 3주 이내 치료한 질 병이 없고, 현재 특별한 이상증상이 없는 신체 건강한 만 20~39세의 자원자로 하였다.
(2) 제외기준
Body mass index(BMI)가 18 kg/m2 미만 32 kg/m2 이 상인 사람, 부정맥이 있는 사람, 수축기 혈압이 110~120
㎜Hg, 이완기 혈압이 70~80 ㎜Hg범위를 벗어나는 사람, 맥진측정부위에 신체적 위해가 있었던 사람(심장 수술 후 손목 혈관의 손상, 기타 자상이나 찰과상으로 흉터가 남아 있는 사람), 최근 3주 이내 혈행개선 관련 약물을 복용한 사람, 월경 중인 여성, 임산부, 최근 3개월 내에 다른 임상 시험에 참가한 사람, 한의학 전공자는 제외하였다.
3) 피험자 수 산정
본 연구는 舍巖鍼에 따른 맥 변화 연구이며, 탐색적 연구 자 임상연구로 피험자 수 선정은 자침에 의한 요골동맥파 의 변화를 분석한 선행연구들- Pierre Boutouyrie et al22) 의 연구(환자 19명, 정상인 8명), Wang WK et al23)의 연 구(정상인 15명) 및 肺正格과 胃正格 등의 시험결과를 바탕
으로18-21) 유의미한 결과도출을 위하여 피험자수를 군간 20
명, 총 60명을 모집하였다.
2. 시험방법
1) 맥파측정
측정은 DMP-3000(DAEYO MEDI, KOREA)을 사용하 여 앉은 자세에서 시행하였다. 실험 장소에 도착한 참가자 는 실험에 대한 상세한 설명을 듣고 동의서에 서명한 후 30분간 휴식을 취하였다. 맥 측정 부위가 일정하도록 유성 펜으로 좌우 關 부위에 표시를 하고, 좌우 寸ㆍ關ㆍ尺 6부
위에서 1차 맥 측정을 시행하였다. 寸ㆍ關ㆍ尺 부위 설정 은, 關 부위는 요골 경상돌기 부위를, 寸 부위는 關으로부 터 손목 쪽으로 약 9分 부위를, 尺 부위는 몸 쪽으로 약 1寸 의 거리에 정하였다.
자침군은 침대에 누운 자세로 20분간 자침시술을 받았 으며, 대조군은 침 시술 없이 침대에 같은 시간 동안 누워 있었다. 자침군은 침 시술이 끝난 후 1차 맥 측정 시 표시 한 關 부위 기준에 맞추어 拔鍼 직후, 30분 후, 60분 후에 같은 방법으로 2ㆍ3ㆍ4차 맥 측정을 시행하였으며, 대조군 도 침대에서 내려와 같은 방법으로 2ㆍ3ㆍ4차 맥 측정을 시행하였다.
실험이 진행되는 동안 참가자는 안정을 취하였으며, 물 이 외의 음식섭취나 흡연을 금하였다. 실내 온도는 24~26 ℃, 습도는 40~60 %를 유지하였다.
2) 자침
모든 자침 시술은 한의사 면허를 소지한 동일 시술자가 시술하였다. 지원자가 침대에 누운 후 자침 부위를 소독하 고, 일회용 침(0.25×30 ㎜, Dong Bang Acupuncture Co.
Korea)을 사용하여 大腸正格群은 曲池(LI11)ㆍ足三里(ST36) 補, 陽谿(LI5)ㆍ陽谷(SI5) 瀉의 순서로, 大腸勝格群은 陽谿 (LI5)ㆍ陽谷(SI5) 補, 二間(LI2)ㆍ足通谷(BL66) 瀉의 순서로, 迎隨補瀉를 사용하여 우측을 먼저 刺鍼한 후 좌측을 자침하 였다. 경혈 위치는 WHO 표준안에 준하였으며, 刺鍼 깊이 는 曲池(LI11)ㆍ足三里(ST36) 5~7分, 陽谿(LI5)ㆍ陽谷(SI5)ㆍ 二間(LI2)ㆍ足通谷(BL66) 2~5分 내외로 하였다. 자침 후 圓 方補瀉, 九六補瀉를 사용하여 자침 순서와 같은 순서로 補 瀉手技하고, 20분간 留鍼한 후, 같은 순서로 拔鍼하였다.
3. 맥파분석
1) 대표맥 추출
측정부위에 가하는 압력을 5단계로 하여, 각 단계에서 측정된 맥파 중 첫 번째 피크의 크기가 가장 큰 맥파를 대 표맥으로 설정하였다
2) 주요 분석 요소
중앙센서에서 얻은 대표맥을 분석하여 각 변수를 도출하 였다. 단, pulse energy는 중앙과 상하좌우 5개 센서에서 얻은 대표맥들로부터 계산하였다.
① Applied pressure : 대표 맥파를 얻을 때 외부에서 가해진 압력. 단위는 g
② Elasticity : 압력센서로봇의 이동거리 대비 가압의 변화. 단위는 gfm/cm2
③ H1 : 주파(main peak)의 크기(amplitude). 단위는 div(digital value for pressure)
④ Variance of magnitude : H1의 분산
⑤ T(pulse period) : 맥동 주기. 단위는 초(s)
⑥ T1 : 급성 사혈기 시간. 단위는 초(s)
⑦ T1/T : 맥동주기에 대한 급성 사혈기 시간의 비율
⑧ T4 : 수축기 시간. 단위는 초(s)
⑨ T-T4 : 이완기 시간. 단위는 초(s)
⑩ W : 주파 크기(H1)의 2 / 3가 되는 지점의 시간 축 너 비. 단위는 초(s)
⑪ Angle of main peak : 주파에서 W 사이의 각도. 단 위는 degree
⑫ Augmentation index(AIx) : H1에 대한 H3의 비율
⑬ AIx / HR : AIx를 박동 수로 나눈 값
⑭ P(pulse power volume) : 5개 센서에서 측정된 최대 변위 맥압의 적분값. 단위는 div3
⑮ Pulse power volume / min(P min) : 분당 pulse energy. 단위는 div3 / min
⑯ F1 : 맥파를 고속 퓨리에 변환(fast Fourier fransform : FFT)하여 얻은 첫 번째 퓨리에 성분(Fourier component)의 진동수(frequency). 단위는 Hz
⑰ M1 : 맥파를 고속 퓨리에 변환(fast Fourier fransform : FFT)하여 얻은 첫 번째 퓨리에 성분(Fourier component)의 파폭(magnitude). 단위는 div
3) 변화율
측정한 데이터는 자침 전의 측정값에 대한 변화율로 환 산하였다. 자침 전, 자침 후 0분, 30분 60분의 측정값을 각 각 Mbefore, M1, M2, M3라 할 때, 그 변화율 C1, C2, C3는 아 래와 같이 계산하였다.
Cn = Mn - Mbefore
Mbefore
Mn : nth measured value after acupuncture Mbefore : value measured before acupuncture Cn : change ratio from Mbefore to Mn
4) 통계분석
통계 분석은 PASW statistics 18(SPSS 18.0)을 이용하 였다. 데이터는 평균 ± 표준편차로 나타내었다. 좌우 寸ㆍ 關ㆍ尺 6부위 통합 분석은 repeated measures ANOVA (analysis of variance) test를 이용하였으며(n=120. 6부
위 당 20명), 각 time point별 군간 비교는 one way ANOVA를 이용하고 사후분석은 least significant difference(LSD) test를 사용하였다. 좌우 寸ㆍ關ㆍ尺 부위 별 분석은 각 time point별로 Kruskal-Wallis 방법을 사 용하고(n=20), 다시 Mann-Whitney U test를 사용하여 군간 비교하였다. 유의 검정 수준은 신뢰도 95 % 이상 (p<0.05)으로 하였다.
4. 이상반응
침 시술 이후 발생할 수 있는 心悸, 惡心, 眩暈, 자침 부 위 피하출혈 등의 이상반응은 60명의 자원자 모두 관찰되 지 않았다.
Ⅲ. 결 과
1. 좌우 寸ㆍ關ㆍ尺 6부위 통합 맥파 분석
1) Angle of main peak
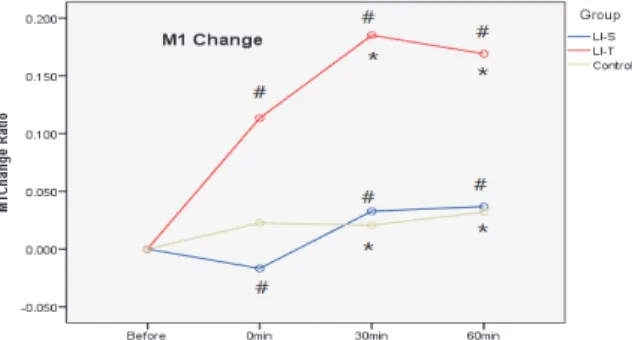
大腸正格群과 大腸勝格群의 주파각이 유의한 차이를 나타 내었다. 각 time point별 군간 비교 결과, 발침 직후 大腸 勝格群에서 大腸正格群에 비하여 주파각이 유의하게 증가하 였다(Fig. 1).
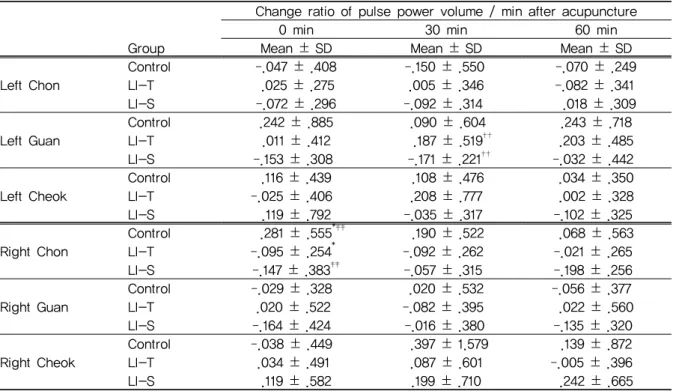
2) Magnitude of Fourier component 1(M1) 大腸正格群과 大腸勝格群의 M1이 군간 유의한 차이를 나 타내었다. 각 time point별 군간 비교 결과, 발침 직후 大 腸正格群에서 大腸勝格群에 비하여 M1이 유의하게 증가하 였으며, 발침 30분 후와 발침 60분 후 大腸正格群에서 대 조군과 大腸勝格群에 비하여 M1이 유의하게 증가하였다 (Fig. 2).
2. 좌우 寸ㆍ關ㆍ尺 부위별 맥파 분석
1) Elasticity
발침 60분 후 왼쪽 尺 부위에서 대조군과 大腸勝格群 에 비하여 大腸正格群의 탄성도가 유의하게 감소하였다 (Table 1).
Fig. 1. Effect of Sa-Am large intestine tonifying and sedating acupuncture on main peak angle of radial pulse
Healthy subjects in LI-T and LI-S group were given large intestine tonifying Sa-Am acupuncture and large intestine sedating Sa-Am acupuncture respectively. Those in control group took rest without acupuncture. Radial pulse was measured using 3 dimensional pulse imaging system at six different measuring locations before, right after, 30 minutes after and 60 minutes after acupuncture. Change ratio of main peak angle after acupuncture at each time point were analyzed. Data were expressed as mean ± SD(n=120).
LI-T : large intestine tonifying Sa-Am acupuncture group.
LI-S : large intestine sedating Sa-Am acupuncture group.
# : p<0.05, LI-T vs LI-S by ANOVA.
Fig. 2. Effect of Sa-Am large intestine tonifying and sedating acupuncture on M1 of radial pulse
Healthy subjects in LI-T and LI-S group were given large intestine tonifying Sa-Am acupuncture and large intestine sedating Sa-Am acupuncture respectively. Those in control group took rest without acupuncture. Radial pulse was measured using 3 dimensional pulse imaging system at six different measuring locations before, right after, 30 minutes after and 60 minutes after acupuncture. Change ratio of M1 after acupuncture at each time point were analyzed. Data were expressed as mean ± SD(n=120).
LI-T : large intestine tonifying Sa-Am acupuncture group.
LI-S : large intestine sedating Sa-Am acupuncture group.
* : p<0.05, LI-T vs control by ANOVA.
# : p<0.05, LI-T vs LI-S by ANOVA.
2) Amplitude of H1
발침 30분 후 왼쪽 關 부위에서 대조군과 大腸勝格群에 비하여 大腸正格群의 H1이 유의하게 증가하였다(Table 2).
Change ratio of elasticity after acupuncture
0 min 30 min 60 min
Group Mean ± SD Mean ± SD Mean ± SD
Left Chon
Control .110 ± .186 .068 ± .407 .165 ± .247
LI-T .041 ± .307 .279 ± .405 .190 ± .411
LI-S .202 ± .378 .187 ± .341 .137 ± .414
Left Guan
Control .104 ± .430 .022 ± .284 .210 ± .601
LI-T .129 ± .409 .227 ± .660 .118 ± .315
LI-S .031 ± .409 ‐.037 ± .332 .075 ± .423
Left Cheok
Control .145 ± .388 .085 ± .355 .155 ± .329*
LI-T ‐.008 ± .289 .119 ± .335 ‐.039 ± .336*†
LI-S .071 ± .286 .100 ± .295 .159 ± .358†
Right Chon
Control .072 ± .517 .189 ± .479 .146 ± .362
LI-T .286 ± .821 .201 ± .574 .112 ± .535
LI-S .010 ± .283 .022 ± .372 .052 ± .337
Right Guan
Control .170 ± .412 .182 ± .555 .106 ± .437
LI-T .153 ± .563 .212 ± .583 .247 ± .680
LI-S .088 ± .352 .088 ± .465 .041 ± .463
Right Cheok
Control ‐.008 ± .238 .108 ± .243 .001 ± .207
LI-T ‐.039 ± .326 .040 ± .287 .133 ± .615
LI-S .078 ± .377 ‐.017 ± .327 .074 ± .320
LI-T : large intestine tonifying Sa-Am acupuncture group. LI-S : large intestine sedating Sa-Am acupuncture group.
* : p<0.05, LI-T vs control by Mann-Whitney test. † : p<0.05, LI-T vs LI-S by Mann-Whitney test.
Table 1. Effect of Sa-Am Large Intestine Tonifying and Sedating Acupuncture on the Change of Elasticity of Radial Pulse at Each Measuring Point
Change ratio of H1 after acupuncture
0 min 30 min 60 min
Group Mean ± SD Mean ± SD Mean ± SD
Left Chon
Control ‐.027 ± .278 ‐.111 ± .403 .008 ± .266
LI-T .065 ± .189 .106 ± .346 .051 ± .262
LI-S .038 ± .246 .035 ± .269 .097 ± .236
Left Guan
Control .070 ± .176 .038 ± .273* .131 ± .272
LI-T .164 ± .565 .318 ± .450*† .376 ± .513
LI-S ‐.053 ± .237 .010 ± .241† .145 ± .411
Left Cheok
Control ‐.056 ± .209 .022 ± .212 ‐.000 ± .201
LI-T ‐.014 ± .206 .154 ± .288 .072 ± .204
LI-S ‐.087 ± .220 .000 ± .187 ‐.052 ± .233
Right Chon
Control .063 ± .381 .058 ± .338 ‐.007 ± .374
LI-T .561 ± 2.571 .682 ± 3.056 .657 ± 2.809
LI-S ‐.067 ± .360 .042 ± .294 ‐.091 ± .268
Right Guan
Control .113 ± .419 .069 ± .522 .135 ± .437
LI-T .061 ± .343 .076 ± .344 .127 ± .467
LI-S ‐.080 ± .259 .052 ± .221 ‐.023 ± .321
Right Cheok
Control ‐.024 ± .258 .093 ± .774 ‐.007 ± .462
LI-T .010 ± .202 .072 ± .176 .026 ± .203
LI-S .210 ± .618 .226 ± .607 .238 ± .709
LI-T : large intestine tonifying Sa-Am acupuncture group. LI-S : large intestine sedating Sa-Am acupuncture group.
* : p<0.05, LI-T vs control by Mann-Whitney test. † : p<0.05, LI-T vs LI-S by Mann-Whitney test.
Table 2. Effect of Sa-Am Largeintestine Tonifying and Sedating Acupuncture on the Change of H1 of Radial Pulse at Each Measuring Point
Change ratio of AIx / HR after acupuncture
0 min 30 min 60 min
Group Mean ± SD Mean ± SD Mean ± SD
Left Chon
Control .074 ± .286 .063 ± .449 .061 ± .303
LI-T 210 ± .447 .239 ± .475 .234 ± .371
LI-S .129 ± .385 .250 ± .401 .218 ± .377
Left Guan
Control .033 ± .168 .122 ± .439 .178 ± .343
LI-T .172 ± .292 .209 ± .367 .159 ± .244
LI-S .104 ± .311 .282 ± .328 .179 ± .345
Left Cheok
Control .110 ± .341 .096 ± .476 .193 ± .322
LI-T .208 ± .275 .228 ± .427 .259 ± .444
LI-S .210 ± .369 .225 ± .403 .259 ± .358
Right Chon
Control ‐.099 ± .297 .144 ± .580 .136 ± .490
LI-T .054 ± .440 .005 ± .257 .092 ± .360
LI-S .066 ± .382 .216 ± .409 .091 ± .417
Right Guan
Control ‐.034 ± .409 .147 ± .674 .156 ± .445
LI-T .027 ± .258 .113 ± .279 .002 ± .251
LI-S .093 ± .256 .052 ± .206 .275 ± .665
Right Cheok
Control .176 ± .736 .149 ± .637 .114 ± .548
LI-T ‐.077 ± .240 .001 ± .354†† ‐.041 ± .322
LI-S .192 ± .450 .343 ± .462†† .179 ± .319
LI-T : large intestine tonifying Sa-Am acupuncture group. LI-S : large intestine sedating Sa-Am acupuncture group.
†† : p<0.01, LI-T vs LI-S by Mann-Whitney test.
Table 3. Effect of Sa-Am Large Intestine Tonifying and Sedating Acupuncture on the Change of AIx / HR of Radial Pulse at Each Measuring Point
3) AIx / HR
발침 30분 후 오른쪽 尺 부위에서 大腸勝格群의 AIx / HR이 大腸正格群에 비하여 유의하게 증가하였다(Table 3).
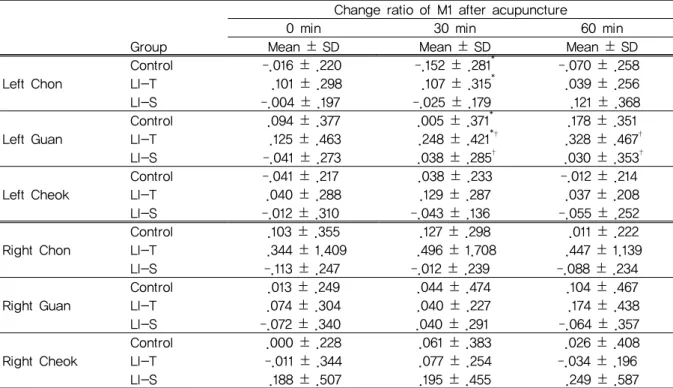
4) Pulse power volume / min
발침 30분 후에는 왼쪽 關 부위에서 大腸正格群의 분당 pulse power volume이 大腸勝格群에 비하여 유의하게 증 가하였다(Table 4).
5) Frequency of Fourier component 1(F1) 발침 직후 오른쪽 關 부위에서 大腸正格群의 F1이 대조군
에 비하여 유의하게 감소하였고, 오른쪽 尺 부위에서 大腸 勝格群의 F1이 대조군에 비하여 유의하게 감소하였다. 발 침 30분 후에는 왼쪽 關과 오른쪽 尺 부위에서 大腸勝格群 의 F1이 대조군과 大腸正格群에 비하여 유의하게 감소하였 다. 발침 60분 후에도 오른쪽 尺 부위에서 大腸勝格群의 F1 이 대조군에 비하여 유의하게 감소하였다(Table 5).
6) Magnitude of Fourier component 1(M1) 왼쪽 關 부위에서 大腸正格群의 M1이 대조군과 大腸勝格 群에 비하여 유의하게 증가하였다. 발침 60분 후에는 왼쪽 關 부위에서 大腸正格群의 M1이 大腸勝格群에 비하여 유의 하게 증가하였다(Table 6).
Change ratio of pulse power volume / min after acupuncture
0 min 30 min 60 min
Group Mean ± SD Mean ± SD Mean ± SD
Left Chon
Control ‐.047 ± .408 ‐.150 ± .550 ‐.070 ± .249
LI-T .025 ± .275 .005 ± .346 ‐.082 ± .341
LI-S ‐.072 ± .296 ‐.092 ± .314 .018 ± .309
Left Guan
Control .242 ± .885 .090 ± .604 .243 ± .718
LI-T .011 ± .412 .187 ± .519†† .203 ± .485
LI-S ‐.153 ± .308 ‐.171 ± .221†† ‐.032 ± .442
Left Cheok
Control .116 ± .439 .108 ± .476 .034 ± .350
LI-T ‐.025 ± .406 .208 ± .777 .002 ± .328
LI-S .119 ± .792 ‐.035 ± .317 ‐.102 ± .325
Right Chon
Control .281 ± .555*‡‡ .190 ± .522 .068 ± .563
LI-T ‐.095 ± .254* ‐.092 ± .262 ‐.021 ± .265
LI-S ‐.147 ± .383‡‡ ‐.057 ± .315 ‐.198 ± .256
Right Guan
Control ‐.029 ± .328 .020 ± .532 ‐.056 ± .377
LI-T .020 ± .522 ‐.082 ± .395 .022 ± .560
LI-S ‐.164 ± .424 ‐.016 ± .380 ‐.135 ± .320
Right Cheok
Control ‐.038 ± .449 .397 ± 1.579 .139 ± .872
LI-T .034 ± .491 .087 ± .601 ‐.005 ± .396
LI-S .119 ± .582 .199 ± .710 .242 ± .665
LI-T : large intestine tonifying Sa-Am acupuncture group. LI-S : large intestine sedating Sa-Am acupuncture group.
* : p<0.05, LI-T vs control by Mann-Whitney test. ‡‡ : p<0.001, LI-S vs control by Mann-Whitney test.
†† : p<0.01, LI-T vs LI-S by Mann-Whitney test.
Table 4. Effect of Sa-Am Large Intestine Tonifying and Sedating Acupuncture on the Change of Pulse Power Volume / Min at Each Measuring Point
Change ratio of F1 after acupuncture
0 min 30 min 60 min
Group Mean ± SD Mean ± SD Mean ± SD
Left Chon
Control ‐.033 ± .103 ‐.018 ± .179 ‐.052 ± .139
LI-T ‐.069 ± .138 ‐.092 ± .115 ‐.102 ± .149
LI-S ‐.060 ± .136 ‐.083 ± .189 ‐.103 ± .162
Left Guan
Control ‐.015 ± .115 ‐.062 ± .175‡ ‐.075 ± .080
LI-T ‐.079 ± .126 ‐.062 ± .159† ‐.136 ± .103
LI-S ‐.099 ± .103 ‐.150 ± .145‡† ‐.127 ± .122
Left Cheok
Control ‐.010 ± .111 ‐.017 ± .210 ‐.073 ± .152
LI-T ‐.063 ± .129 ‐.084 ± .107 ‐.122 ± .113
LI-S ‐.036 ± .126 ‐.073 ± .138 ‐.070 ± .139
Right Chon
Control .011 ± .140 ‐.038 ± .108 ‐.046 ± .077
LI-T .016 ± .187 ‐.039 ± .154 ‐.035 ± .208
LI-S ‐.005 ± .200 ‐.098 ± .120 ‐.064 ± .131
Right Guan
Control .012 ± .117** ‐.000 ± .180 ‐.050 ± .072
LI-T ‐.078 ± .112** ‐.065 ± .110 ‐.100 ± .150
LI-S ‐.017 ± .102 ‐.065 ± .133 ‐.056 ± .156
Right Cheok
Control ‐.025 ± .053‡‡ ‐.015 ± .146‡‡ ‐.027 ± .091‡‡
LI-T ‐.043 ± .109 ‐.016 ± .139† ‐.078 ± .156
LI-S ‐.085 ± .080‡‡ ‐.117 ± .126‡‡† ‐.119 ± .084‡
LI-T : large intestine tonifying Sa-Am acupuncture group. LI-S : large intestine sedating Sa-Am acupuncture group.
** : p<0.01, LI-T vs control by Mann-Whitney test. † : p<0.05, LI-T vs LI-S by Mann-Whitney test.
‡ : p<0.05, ‡‡ : p<0.001, LI-S vs control by Mann-Whitney test.
Table 5. Effect of Sa-Am Large Intestine Tonifying and Sedating Acupuncture on the Change of F1 of Radial Pulse at Each Measuring Point
Change ratio of M1 after acupuncture
0 min 30 min 60 min
Group Mean ± SD Mean ± SD Mean ± SD
Left Chon
Control ‐.016 ± .220 ‐.152 ± .281* ‐.070 ± .258
LI-T .101 ± .298 .107 ± .315* .039 ± .256
LI-S ‐.004 ± .197 ‐.025 ± .179 .121 ± .368
Left Guan
Control .094 ± .377 .005 ± .371* .178 ± .351
LI-T .125 ± .463 .248 ± .421*† .328 ± .467†
LI-S ‐.041 ± .273 .038 ± .285† .030 ± .353†
Left Cheok
Control ‐.041 ± .217 .038 ± .233 ‐.012 ± .214
LI-T .040 ± .288 .129 ± .287 .037 ± .208
LI-S ‐.012 ± .310 ‐.043 ± .136 ‐.055 ± .252
Right Chon
Control .103 ± .355 .127 ± .298 .011 ± .222
LI-T .344 ± 1.409 .496 ± 1.708 .447 ± 1.139
LI-S ‐.113 ± .247 ‐.012 ± .239 ‐.088 ± .234
Right Guan
Control .013 ± .249 .044 ± .474 .104 ± .467
LI-T .074 ± .304 .040 ± .227 .174 ± .438
LI-S ‐.072 ± .340 .040 ± .291 ‐.064 ± .357
Right Cheok
Control .000 ± .228 .061 ± .383 .026 ± .408
LI-T ‐.011 ± .344 .077 ± .254 ‐.034 ± .196
LI-S .188 ± .507 .195 ± .455 .249 ± .587
LI-T : large intestine tonifying Sa-Am acupuncture group. LI-S : large intestine sedating Sa-Am acupuncture group.
* : p<0.05, LI-T vs control by Mann-Whitney test. †: p<0.05, LI-T vs LI-S by Mann-Whitney test.
Table 6. Effect of Sa-Am Large Intestine Tonifying and Sedating Acupuncture on the Change of M1 of Radial Pulse at each Measuring Point
Ⅳ. 고 찰
脈診은 한의학 진단법인 四診의 切診 중 하나로 脈搏의 常과 變에 근거하여 인체의 건강상태를 살피고, 病이 어느 經絡과 臟腑에 있는지, 寒熱·表裏·虛實 중의 어디에 속하는 지, 疾病의 진퇴와 豫後 등을 진단하는 중요한 의의가 있다1).
脈診은 ≪黃帝內經≫에서 시작되었으며, 그 진단 부위에 따라 臟腑經脈遍診法, 三部九候法, 人迎寸口對比診, 獨取寸口 脈法 등이 있다1). 이중 寸口脈法이 간편하여 실행하기 쉽고 개괄성이 강하며 전신 臟腑의 질병을 알 수 있는 장점 때문 에 후세에 주로 사용되고 있다24-26).
寸口脈法의 장부 배속에 대한 여러 가지 이론이 있으나, 일반적으로 왼쪽 寸에서는 心을, 오른쪽 寸에서는 肺를 살 피며, 왼쪽 關에서는 肝膽을, 오른쪽 關에서는 脾ㆍ胃를 살 피며, 왼쪽 尺에서는 腎ㆍ膀胱ㆍ小腸을, 오른쪽 尺에서는 大腸ㆍ命門ㆍ三焦의 상태를 반영한다. 이중 오른쪽 尺은 주 로 三焦의 상태를 나타내는 것으로 알려져 있으나, 최근 여 러 연구와 문헌에 따르면2)大腸은 腹中을 주관하는 尺部에 배속하여 살펴볼 수 있다. 각 위치는 각기 다른 장부의 기 능과 연결하여 해석하며, 각 부위 맥동의 힘, 주기, 맥의
팽창과 수축 빠르기, 맥의 촉지깊이, 맥의 폭, 맥의 유효한 촉지 길이 등의 차이에 따라 진단한다8).
이러한 脈診은 진단자인 한의사의 감각, 지능, 경험 등에 의존하여 주관적으로 건강상태를 판단하기 때문에 현대의 학에 비해 객관성ㆍ계량성ㆍ재현성이 부족한 진단 방법으 로 지적되어 왔다5).
맥진 데이터의 정량화와 객관화를 위해서는 맥파의 측정 으로 환자의 건강상태를 진단하는 노력이 필요하다5). 현재 이를 위해 맥진 위치의 표준화4)와 맥상의 분석 및 측정 가 능한 물리량에 대한 맥상의 재정의27), 맥상을 재현할 맥진 기의 개발28) 등 다양한 연구가 진행되고 있다.
舍巖鍼法은 臟腑의 虛, 實, 寒, 熱을 판별하여 각각 正, 勝, 熱, 寒格을 통해 臟腑의 기능을 정상화 하여 치료함을 원칙으로 한다. 이 중 正格은 해당 經脈의 기능을 증강시키 기 위한 것으로서 補法이 되며, 勝格은 해당 經脈의 기능을 억제하기 위한 것으로서 瀉法이 된다. 그러나 正格과 勝格 을 단순히 장부론적 개념으로 補瀉한다는 의미로 국한시킬 수 없으며, 경락의 三陰三陽과 六氣 배속의 관계를 고려해 보고 각 正․勝格을 구성하는 五兪穴 개개의 특성 파악 및 이 들 조합의 연쇄적 유기 관계를 생각해야한다29).
현재 舍巖鍼法에 대한 연구로는 문헌적 연구10,11), 다양한
질환에 대한 증례 보고12-14) 및 최근 들어 임상시험 연구가 활발히 진행되고 있다15,16). 이 중 舍巖鍼 자침 후 맥파 변화 에 대한 기존 연구로 특정 舍巖鍼 후 寸ㆍ關ㆍ尺 脈波변화를 비교하는 연구17-21)가 있었으나 아직까지 舍巖鍼法의 正格 과 勝格 자침 후 正ㆍ勝格 간의 맥파 변화를 비교한 연구는 없었다.
이에 저자는 20세부터 39세까지의 정상 성인을 대상으 로 大腸正格과 大腸勝格 시술 후 맥파분석기을 통하여 正․勝 格 자침에 의해 변화되는 맥파의 맥상 데이터를 비교 분석 하기 위해 연구를 진행하였다.
본 연구에서는 정상 성인 60명을 대상으로 시행하였는 데 大腸正格과 大腸勝格 자침군을 각 20명씩, 침 시술 받지 않은 대조군을 20명으로 배정하여 각 군간 자침 전, 발침 직후, 발침 30분 후, 발침 60분 후 변화를 寸ㆍ關ㆍ尺 6부 위에 통합 및 부위별로 비교하여 분석하였다.
좌우 寸ㆍ關ㆍ尺 6부위를 통합 분석한 결과, Angle of main peak, M1은 大腸正格·勝格群 간에서 유의하게 변화하 였다.
맥파 면적 및 파형관련 변수로 Angle of main peak은 주파 크기(H1)의 2 / 3 되는 지점의 시간축 너비인 W 사이 의 각도로 大腸正格群과 勝格群 모두 대조군에 비하여 유의 한 차이를 나타냈으며, 발침 직후 大腸勝格群이 正格群에 비 하여 주파각이 유의하게 증가하였다(Fig. 1). 주파각이 작 을수록 급성 사혈기 시간이 매우 작거나, 심박출량이 크고 사혈속도를 매우 빠르게 하는 의미가 있다30). 大腸勝格群이 박동 주기 증가로 인하여 급성 사혈기 시간 비율이 감소된 것으로 보였으며, 주파의 크기(H1)에 유의한 변화를 보이 지 않아 주파각 감소의 의미를 유추하긴 어려워 이에 관한 연구가 더욱 필요할 것으로 생각된다.
주파수 영역분석을 위해 자침 후 맥파를 고속 퓨리에 변 환(fast Fourier transform : FFT)하여 얻은 첫 번째 성분 의 진동수(frequency of Fourier component 1 : F1)와 첫 번째 성분의 파폭(magnitude of fourier component 1 : M1)을 분석하였다. 비교 분석 결과 M1은 발침 직후, 발침 30분 후 와 발침 60분 후 모두 大腸正格群에서 유의하게 증 가하였다(Fig. 2). 따라서 퓨리에 성분의 파폭의 변화로 大 腸正格과 大腸勝格의 자침에 의해 맥파에 서로 다른 변화를 일으킨다는 차이점을 알 수 있어 연결된 장부의 기능에 서 로 다른 영향을 미칠 것으로 생각된다31).
좌우 寸ㆍ關ㆍ尺 6부위별 맥파 분석에서 유의한 차이를 보인 변수 중 맥압 관련 변수 H1, pulse power volume / min는 모두 왼쪽 關 부위에서 大腸正格群이 유의하게 증가 한 경향을 보여 이는 장부의 臟腑相通의 개념과 연결 지어 볼 수 있다(Table 2, 4). ≪醫學入門≫에 “肝與大腸相通, 肝
病宜踈大腸; 大腸病宜平肝經爲主”라 하여 肝과 大腸이 相通 관계임을 알 수 있다. 相通관계는 그 축이 開闔樞관계로 陰 陽, 각각 氣의 출입 및 승강 조절이라는 측면에서의 기능 활동을 의미한다고 볼 수 있다32). 이와 연결 지어 볼 때 왼 쪽 關은 肝을 진단하는 부위로2)大腸勝格의 자침이 편승한 大腸의 기운을 瀉하여 이와 相通하는 肝의 기운에 영향을 미쳐 왼쪽 關의 맥압 및 주파의 세기가 감소한 것으로 여겨 지며, 大腸正格의 자침이 大腸의 기운을 補하여 기능을 활 성화시키며 생리 병리적 기능상 연계된 肝의 기능에도 영 향을 미쳐 왼쪽 關 부위 맥의 세기가 유의하게 증가한 것으 로 보인다. 이전 임상연구18,19,21)에서 자침 후 母子相生관계 로 寸ㆍ關ㆍ尺 맥파 변화를 분석하였는데, 이는 舍巖鍼法이 단순히 五行의 相生相克관계로만 설명되지 않은 경락의 三 陰三陽과 六氣 배속 관계까지 고려해야 하는 것을 추론할 수 있다29). 맥의 세기 모두 大腸正格과 勝格의 발침 직후 오 른쪽 寸에서 유의하게 감소한 것은 大腸經에 대한 舍巖鍼法 의 일반적인 효과로 사료되며, 大腸과 表裏관계인 肺의 기 능에 영향을 미친다고 해석할 수 있다. 그러나 이는 大腸經 에 특이적인 舍巖鍼의 효과와 일반적인 자침의 효과의 구별 이 어려워, 脈診과 舍巖鍼에 대한 추가적인 연구가 필요할 것으로 보인다.
탄성 관련 변수로 elasticity, AIx / HR이 유의한 변화 를 보였다. Elasticity는 압력센서 로봇의 이동거리 대비 가압의 변화로 혈관의 탄성도를 의미하며33), AIx / HR는 혈관 경화도 분석 결과로 H1에 대한 H3의 비율인 AIx와 이를 심박 수로 보정한 것으로 AIx는 혈관벽의 순응성, 혈 관벽의 탄성 등의 정보가 있어30) 연령이 증가함에 따란 혈 관 경직도가 증가하며 말초혈관으로부터 돌아오는 반사파 의 진행이 빨라진다6). Elasticity는 발침 60분 후 왼쪽 尺 부위에서 大腸正格群에서 유의한 감소를 보였다(Table 1).
AIx / HR은 발침 30분 후 오른쪽 尺 부위에서 大腸勝格群 이 유의한 증가를 보였다(Table 3). 그러나 본 연구는 정상 성인을 대상으로 연구한 것으로 병리적 변화 및 실제 경화 가 진행되었다고 보기 어렵다. 大腸正格과 大腸勝格이 각기 혈관 탄성과 경화도에 다른 영향을 미친다는 것을 알 수 있 으나, 규칙성을 찾기는 어려웠다. 그러므로 향후 大腸正格 과 勝格의 적응증에 혈관 탄성 및 경화도 변수가 어떠한 관 계가 있는지에 대한 연구가 필요할 것으로 사료된다.
주파수 관련 변수로 좌우 寸ㆍ關ㆍ尺 6부위의 맥파를 고 속 퓨리에 변환하여 하여 얻은 첫 번째 퓨리에 성분의 진동 수(F1)와 파폭(M1)에서 유의한 변화를 보였다(Table 5, 6).
주파수 관련 변수는 寸ㆍ關ㆍ尺 부위에서 규칙적인 변화 가 보이진 않으나, 寸ㆍ關ㆍ尺 각 부위가 특정 장부에 배속 되어, 또한 특정 퓨리에 성분이 그 장부와 관련이 있다면,
그 부위에서 퓨리에 성분이 중요한 역할을 할 것으로 추정 할 수 있다31,34,35). 寸ㆍ關ㆍ尺 부위에 어떠한 퓨리에 성분 이 배속 및 변화되는지는 객관적으로 검증된 바가 없다. 향 후 각 퓨리에 성분의 변화에 관한 데이터를 구축하여, 자침 이후 각 퓨리에 성분 변화를 통해 이와 연관된 臟腑, 經絡 및 寸ㆍ關ㆍ尺 부위에 미치는 영향을 분석할 단서가 되길 기대한다.
본 연구는 20~39세의 정상 성인 지원자를 대상으로 大 腸正格과 大腸勝格 자침이 맥파에 미치는 영향을 비교한 기 초 연구로서 대상 인원이 군당 20명씩, 총 60명으로 그 수 가 적고, 대조군이 단순 안정 대조군인 점, 그리고 大腸正 格과 勝格의 자침 혈위 간 비교가 어렵다는 점 등이 한계점 이다.
향후 본 연구의 결과를 바탕으로 다른 經絡의 자침 후 변 화된 데이터가 축적된다면 각 臟腑별로 및 자침법에 따른 특이적 맥상 변화를 정확히 알 수 있을 것이며, 그와 연결 된 臟腑와 相生相克 및 三陰三陽의 관계에 따른 臟腑와 經絡 의 변화를 아는 지표가 될 것으로 사료된다.
Ⅴ. 결 론
맥파분석기을 이용하여 신체 건강한 성인 만 20~39세의 지원자를 대상으로 대조군 20명, 大腸勝格群과 大腸正格群 20명씩으로 총 60명을 대상으로 大腸正格과 大腸勝格의 자 침이 맥파에 미치는 영향을 비교 분석하였다. 침 시술을 받 지 않은 대조군과 大腸勝格과 大腸正格을 각각 자침한 시험 군을 자침 전, 발침 직후, 30분 후, 60분 후 좌우 寸ㆍ關ㆍ 尺 통합한 맥파 변화와 및 각 6부위에서의 맥파 변화를 비 교 분석한 결과 아래와 같은 결론을 얻었다.
1. 좌우 寸ㆍ關ㆍ尺 6부위 통합 맥파 분석 결과, angle of main peak, M1은 大腸正格·勝格群 간에서 유의하게 변화하였다.
2. 좌우 寸ㆍ關ㆍ尺 6부위별 맥파 분석 결과, amplitude of H1는 左關 부위, pulse power volume / min는 왼 쪽 關 부위, elasticity는 왼쪽 尺 부위, AIx/HR은 오 른쪽 尺 부위, F1은 左關과 오른쪽 尺 부위, M1은 왼 쪽 關 부위에서 大腸正格群과 大腸勝格群 간에 유의한 차이를 보였다.
3. 이상의 결과에서 大腸正格과 大腸勝格의 자침이 맥파 에 서로 다른 변화를 유도할 수 있음을 확인하였으며, 향후 추가적인 연구가 필요할 것으로 사료된다.
Ⅵ. References
1. Lee BG, Park YB, Kim TH. Diagnostics of oriental medicine. Seoul : Seongbosa. 2004 : 161-3, 173-6.
2. Yang KY. A study on The assignment of Jangbu to Chon Gwan Cheok in Maekyojeongmiron. J Korean Medical Classics. 2009 ; 22(1) : 27-34.
3. Lee J, Lee YJ, Jeon YJ, Lee HJ, Yoo HH, Kim JY.
An example of test on differences of pulse waveform characteristics at Cun Guan and Chi. Korean Jounal of Oriental Medicine. 2008 ; 14(2) : 107-12.
4. Kim HH, Lee J, Kim KW, Kim JY. Proposal for pulse diagnosis positions(Chon-Kwan-Chuk) for pulse analyzer based on literature review and anthropometry. The Journal of Korean Acu- puncture & Moxibustion Society. 2007 ; 28(3) : 13-22.
5. Na CS, Youn DH, Kim YS et al. The study of non- contact/non-invasive pulse analyzing system using optical coherence tomography(OCT) for oriental pulse diagnosis. Korean Journal of Acupuncture. 2009 ; 26(2) : 1-13.
6. Kwon SM, Kang HJ, Yim YK, Lee YH. Analysis of arterial stiffness by age using pulse waveform measurement of 5-levels graded pressure. The Journal of Korean Am-meridian & Pointology Society. 2010 ; 27(2) : 107-20.
7. Kim GC, Lee JW, Ryu GH, Kang HJ. Study on the character of the old aged pulsation. Journal of Korean Institute of Oriental Medical Diagnostics.
2009 ; 12(2) : 1-6.
8. Lee DH, Hong YS, Lee SS. Development of oriental- western fusion patient monitor by using the clip-type pulsimeter equipped with a hall sensor, the electrocardiograph, and the photoplethysmo- graph. Journal of the Korean Magnetics Society.
2013 ; 23(4) : 135-43.
9. National institute of Korean acupuncture & Moxi- bustion Medicine Society. The acupuncture &
moxibustion. Seoul : Jipmoondang. 2008 : 259-62.
10. Park SH, Shin JC, Ryu CR, Cho MR. A study on InyeongㆍChon spot pulse about application of
Ohaeng-acupuncture. The Journal of Korean Acupuncture & Moxibustion Society. 2004 ; 21(4) : 149-58.
11. Lee IS. Study of combination principles of points in Sa-am acupuncture therapy. Korean J. oriental physiology & pathology. 2012 ; 26(4) : 432-6.
12. Im YG, Hwang WD. A case report of interstitial cystitis treated with Sa-am acupuncture treatments. The Journal of Korean Acupuncture
& Moxibustion Society. 2012 ; 29(2) : 107-11.
13. Oh KC. A clinical report on episodic vertigo with Meniere’ disease treated by Sa-Am acupuncture Sojangjungkyuk. The Journal of the Korea Institute of Oriental Medical Diagnostics. 2012 ; 16(1) : 35-44.
14. Lee SM, Kim SH, Jeong HH et al. Effects of Sa- am acupuncture treatment on a ALS (amyotrophic lateral sclerosis) patient. The Journal of Korean Acupuncture & Moxibustion Society. 2012 ; 29(5) : 187-95.
15. Park YS, Kim EM, Kim YI, Hong KE, Lee H. The depressive effect of Sa-Am acupuncture treatment in stroke patients. The Journal of Korean Acupuncture & Moxibustion Society. 2004 ; 21(4) : 217-23.
16. Choi WJ, Lee SG, Son IB, Sun SH. The effects of Sa-am Acupuncture Simpojeongkyeok treatment on Hwa-byung: randomized, patient-assessor blind, placebo-controlled acupuncture, pilot clinical trial. J. of Oriental Neuropsychiatry. 2011 ; 22(2) : 1-13.
17. Yim YK, LEE H, Lee BR, Lee YH, Yoon YJ, Ro JY.
Effect of Sa-Am acupuncture on radial pulse: a comparative study of stomach-tonification and spleen-tonification. Korean Journal of Acupuncture. 2011 ; 28(3) : 25-32.
18. Choi JY, Kang JH, Yim YK, Lee H. The effect of Sa-Am stomach tonifying acupuncture on radial pulse in healthy human subjects. The Journal of Korean Acupuncture & Moxibustion Medicine Society.
2012 ; 29(6) : 57-71.
19. Kim NY, Kang JH, Lee H. The effects of Sa-Am lung tonifying acupuncture on radial pulse in healthy human subjects. The Journal of Korean
Acupuncture & Moxibustion Medicine Society.
2012 ; 29(5) : 17-29.
20. Kim SJ, LEE H. The effects of Sa-Am stomach tonifying acupuncture on radial pulse in healthy human subjects. The Journal of Korean Acu- puncture & Moxibustion Medicine Society. 2012 ; 29(6) : 57-71.
21. Yoon KS, Lee H. The effects of Sa-Am spleen- tonifying acupuncture on radial pulse in healthy human subjects. The Journal of Korean Acu- puncture & Moxibustion Medicine Society. 2013 ; 30(4) : 1-14.
22. Pierre Boutouyrie, Robert Orvisier, Michel Azizi el al. Effects of acupuncture on radial artery hemodynamics: effects of acupuncture on radial artery hemodynamics: controlled trials in sensitized and naive subjects. Am J Physiol Heart Circ Physiol. 2001 ; 280(2) : 628-33.
23. Wang WK, Hsu TL, Chang HC. Effect of acu- puncture at Hsien-Ku(ST43) on the pulse spectrum and a discussion of the evidence for the frequency structure of Chinese medicine. The American Journal of Chinese Medicine. 2000 ; 28(1) : 41-55.
24. Lee HG, Yoon CY. The studies on the history of development of diagnotics of Myeong dynasty(明 代). Korean Medical Classics. 2001 ; 5(1) : 56-75.
25. Kim JI, Ahn HM, Kim KS, Goo BS. Studies on Chonguinyoung pulse diagnosis. Journal of the Korean Academy of Medical Gigong. 2001 ; 11(1) : 170-85.
26. Lim SC, Hwang MS, Son SC, Lee KM, Kim KS, Yoon JH. The study of pulse diagnosis about twelve meridians. The Journal of Korean Acu- puncture & Moxibustion Society. 2002 ; 19(5) : 1-9.
27. Ryu HH, Lee SW, Lee J, Lee YJ, Kim JY. Analysis of physical quantification of pulse types by pulse diagnosis literatures. Korean J Oriental Physiology & Pathology. 2007 ; 21(6) : 1381-87.
28. Jeon YJ, Lee J, Ryu HH, Lee JH, Lee SW, Kim JY. Development of the pulse analyzing system using FBG. Korean Journal of Oriental Medicine.
2007 ; 13(3) : 105-10.