Arthrosc Orthop Sports Med 2014;1(2):120-123
120
Arthroscopic treatment of soft tissue impingement caused by extruded and a detached cement following total knee replacement arthroplasty
Shin Woo Nam, Yong Seuk Lee, Jun Sung Won, Beom Koo Lee
Department of Orthopedic Surgery, Gachon University Gil Medical Center, Gachon University School of Medicine, Incheon, Korea
INTRODUCTION
Impingement after total knee arthroplasty (TKA) is usually due to problems in soft tissue. It is often associated with pain and mechanical restriction of motion. As in patellar clunk syndromes, it usually develops between the patella and the femoral component [1,2]. We experienced an unusual complication of soft tissue impingement at the femoral component after posterior stabilization of TKA. An impingement of extruded and detached cement mantle into a substantial region of the fibrotic tissue between the posterior part of femoral component and the polyethylene insert occurred. We present this rare case of complication that developed as a result of a fibrous reaction to the extruded and detached cement mantle, which was successfully treated by arthroscopic intervention.
CASE REPORT
A 68yearold woman with a 20year history of tricom
partmental osteoarthritis in both knees underwent TKA (PFC Sigma rotatingplatform; Johnson & Johnson, Raynham, MA, USA). Postoperative radiographs showed components of TKA were properly implanted and subsequent postoperative recovery was uneventful.
At 3 month followup, pain score was much improved and range of motion was from 0o to 120o. However, at approximately 1 year postsurgery, the patient com
plained of pain that developed in the right knee. This pain was aggravated by weightbearing joint motions, especially in the varus position of the knee and when the knee was brought from 90o flexion to full extension along the medial joint line. This pain was relieved in the valgus position of the knee.
Upon physical examination, mild effusion was found whereas joint line tenderness, limitation of motion, coronal and sagittal plane instability, or unusual warmth was not found. Plain radiographs were checked for component loosening, malposition, misalignment, and wear, and it was confirmed that the femoral and tibial components were wellfixed with no abnormalities The clinical outcome to total knee arthroplasty of arthritic knees has been satisfactory, however the complications associated with this approach has continued to evolve. Soft tissue impingement is one of the complications, which can cause pain and limit range of motion. But it can be treated satisfactorily through arthroscopic intervention. We report a patient who suffered from a rare case of impingement caused by irritation of extruded and a detached cement mantle between the femoral component and the polyethylene insert in the medial compartment. In this particular case, arthroscopic treatment successfully treated the complication of impingement after total knee arthroplasty.
Keywords: Total knee arthroplasty; Cement; Impingement; Arthroscopic treatment
http://dx.doi.org/10.14517/aosm13015 pISSN 2289-005X·eISSN 2289-0068
Case Report
Copyright © 2014 Korean Arthroscopy Society and Korean Orthopedic Society for Sports Medicine. All rights reserved.
CC This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Arthroscopy and Orthopedic Sports Medicine
AOSM
Received September 23, 2013; Revised November 15, 2013; Accepted November 16, 2013
Correspondence to: Beom Koo Lee, Department of Orthopedic Surgery, Gachon University Gil Medical Center, Gachon University School of Medicine, 21 Namdong-daero 774beon-gil, Namdong-gu, Incheon 405-760, Korea. Tel: +82-32-460-3384, Fax: +82-32-468- 5437, E-mail: bklee@gilhospital.com
Shin Woo Nam, et al. Arthroscopic treatment of extruded cement following total knee arthroplasty
www.e-aosm.org 121
(Fig. 1A, B). Laboratory tests for infections, including complete blood counts, erythrocyte sedimentation rate and Creactive protein, were all within normal range.
Ultrasonography revealed that there were no specific findings, except for the presence of effusion.
After 6 months of conservative management com
prising of medication, activity modification, and physical therapy failed to resolve the pain, we planned an arthro
scopic intervention for a definitive diagnosis with motives to proceed to treatment as we had suspicions of soft tissue impingement. The arthroscopic procedure was performed through two standard portals. Each
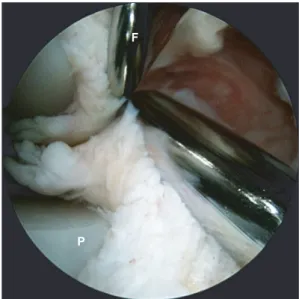
compartment was inspected carefully and dynamically during knee motion. Surprisingly, in the medial gutter, we observed hypertrophic fibrous tissue with generalized synovial reactive processes in each space. In addition, we observed entrapped tissue between components while the knee was flexed from an extension position (Fig. 2). An anterolateral portal was used to inspect and an anteromedial portal was used to remove hypertrophic fibrous tissue with a motorized shaver. After debridement of the fibrous tissue, we saw an unstable cement fragment, which seemed to be the stalk, attached to the distal surface of the femoral component (Fig. 3A). Any
Fig. 2. An arthroscopic view of the medial compartment during dynamic evaluation shows hypertrophic fibrous tissue that is trapped between the femoral components and the polyethylene insert during flexion of the knee from an extension position. F, femoral component; P, polyethylene insert.
Fig. 3. (A) Arthroscopic imaging shows the cement remnant after debriding the hypertrophic fibrous tissue. (B) Removed cement fragment. (C) An arthroscopic view of the upper surface of the medial side of the polyethylene insert shows wears on the polyethylene (arrowhead).
Fig. 1. Anteroposterior (A) and lateral (B) view radiographs of the right knee joint with PFC Sigma rotatingplatform (Johnson & Johnson) pro
sthesis show that the femoral and tibial components are wellcemented and wellsized without any overhang.
Shin Woo Nam, et al. Arthroscopic treatment of extruded cement following total knee arthroplasty
www.e-aosm.org
122
unstable and detached cement fragments were removed with a grasper (Fig. 3B). In addition, wears from scratches were observed on the surface of the medial portion of the polyethylene (Fig. 3C).
Histologically, the hypertrophic fibrous tissue demon
strated mature fibrosis without evidence of inflammation (Fig. 4). Twentytwo months after arthroscopic removal of the cement fragments, the patient was able to maintain a normal range of motion and remain completely pain free.
DISCUSSION
Several types of impingement commonly occur in the patellofemoral compartment. After Hozack et al. [1] first described a patellar clunk syndrome, Thorpe et al. [3]
reported a tethered patellar syndrome and Pollock et al. [4] reported a synovial entrapment syndrome. These syndromes all cause soft tissue impingement due to hyperplasia of fibrous tissue, which is induced by repeated stress. Causative factors of soft tissue impingement are;
design of the femoral component, inflammation due to inadequate soft tissue debridement, extensive surgical trauma, altered extensor mechanism, misalignment of components, and inflammatory diseases such as rheumatoid arthritis [2,5,6]. In fact, extruded cement is an extremely rare cause of impingement after TKA [7,8]. In our case, the patient showed localized pain at the medial joint, which became more intense with motion in the knee. On arthroscopic examination, we found extruded cement once the fibrotic soft tissue was removed in the
medial gutter. Although the etiology of the fibrosis has not been fully understood, the extruded cement seems to have caused the impingement and scratched the upper surface of the medial side of the polyethylene insert. Thus, we suspect that repeated stress induced a reactive synovitis, which in turn caused a detachment of the impinged cement fragment, subsequently forming hypertrophic fibrous tissue [7].
There are two explanations for the medial knee pain elicited by knee motion. First, the hypertrophic fibrous tissue was trapped between the femoral component and the polyethylene insert during flexion and then was compressed and/or jerked during extension. Second, the extruded cement mantle irritated the surrounding synovial tissue or fibrous scar tissue. However, the trapped scar tissue is probably a more reasonable cause of the medial knee pain, because the pain was relieved by valgus position of the knee.
Pseudomeniscus has been reported as a causative factor for impingement after TKA [9]. A buildup of fibrous cartilage after exposure of mesenchymalderived cells to compressive forces is what produces pseudomenisci.
They are associated with a mechanical block such as crepitus. However, in our case, only fibrosis was present without a mechanical block. Thus, we assumed that in our case impingement was induced by fibrous hyper
plasia resulting from repeated stimulation by the ex truded and detached cement fragment as opposed to a pseu do
meniscus.
We observed a relatively premature wearing of the poly ethylene insert near its posterior edge. Saouti et al.
[10] demonstrated earlier that delamination of an anter
omedial part of the insert is associated with substantial synovitis due to a mechanical blockage of the remnant meniscus and a subsequently redistributed stress. Also, Carro and Suarez [11] indicated that impinged tissues cause anomalous stress on the polyethylene insert during repetitive knee motion. Therefore, we considered that wear of the polyethylene insert may have been produced by repeated stress induced by the extruded cement because the scratched line is a definitive linear pattern.
Many studies have previously demonstrated that arthroscopy is effective for diagnosing and treating problematic TKA cases, such as soft tissue impingement, breakage or wear of the polyethylene insert, as well as occult infection. The advantages of arthroscopic intervention are low morbidity, quick functional recovery, reduced risk of infection, and technical simplicity.
Fig. 4. A histologic examination shows degenerated fibrous tissue with an attenuated synovial cell (H&E, ×100).
Shin Woo Nam, et al. Arthroscopic treatment of extruded cement following total knee arthroplasty
www.e-aosm.org 123
Arthroscopic removal of loose bodies has been shown to have good results [1,7,8,11,12]. However, some reports have shown that arthroscopy without sufficient clinical information can lead to incorrect diagnoses [7,12,13] and uncommon infections [14]. Such potential complications should be taken into consideration when surgeons perform arthroscopy. Nevertheless, Diduch et al. [13]
concluded that when welllocalized tissue treatment fails due to impingementinduced generalized synovitis arthroscopy provides the most effective treatment, which is in good agreement with our case.
Conclusively, cautious attention should be paid to the meticulous cleaning of the cement mantle during TKA.
Further, we show that arthroscopic management could be an effective approach to treat patients with postoperative complication, such as impingement by extruded and detached cement mantle, after TKA.
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
1. Hozack WJ, Rothman RH, Booth RE Jr, Balderston RA. The patellar clunk syndrome. A complication of posterior stabilized total knee arthroplasty. Clin Orthop Relat Res 1989;(241):203-8.
2. Koh YG, Kim SJ, Chun YM, Kim YC, Park YS. Arthroscopic treatment of patellofemoral soft tissue impingement after posterior stabilized total knee arthroplasty. Knee 2008;15:36-9.
3. Thorpe CD, Bocell JR, Tullos HS. Intra-articular fibrous bands.
Patellar complications after total knee replacement. J Bone Joint Surg Am 1990;72:811-4.
4. Pollock DC, Ammeen DJ, Engh GA. Synovial entrapment: a complication of posterior stabilized total knee arthroplasty. J Bone Joint Surg Am 2002;84:2174-8.
5. Ip D, Wu WC, Tsang WL. Comparison of two total knee prostheses on the incidence of patella clunk syndrome. Int Orthop 2002;26:48-51.
6. Nakamura I, Michishita K, Tanno M, Ito K. Synovial impingement after posterior cruciate-retaining total knee arthroplasty for rheumatoid arthritis. J Orthop Sci 2006;11:303-7.
7. Bocell JR, Thorpe CD, Tullos HS. Arthroscopic treatment of symptomatic total knee arthroplasty. Clin Orthop Relat Res 1991;(271):125-34.
8. Otani T, Fujii K, Ozawa M, et al. Impingement after total knee arthroplasty caused by cement extrusion and proximal tibiofibular instability. J Arthroplasty 1998;13:589-91.
9. Scher DM, Paumier JC, Di Cesare PE. Pseudomeniscus following total knee arthroplasty as a cause of persistent knee pain. J Arthroplasty 1997;12:114-8.
10. Saouti R, van Royen BJ, Fortanier CM. An impinging remnant meniscus causing early polyethylene failure in total knee arthroplasty: a case report. J Med Case Rep 2007;1:48.
11. Carro LP, Suarez GG. Intercondylar notch fibrous nodule after total knee replacement. Arthroscopy 1999;15:103-5.
12. van Mourik JB, Verhaar JA, Heijboer RP, van Kampen A. Limited value of arthroscopic evaluation and treatment of painful knee prostheses: a retrospective study of 27 cases. Arthroscopy 1998;14:877-9.
13. Diduch DR, Scuderi GR, Scott WN, Insall JN, Kelly MA. The efficacy of arthroscopy following total knee replacement.
Arthroscopy 1997;13:166-71.
14. Klinger HM, Otte S, Baums MH, Lorenz F. Infection after arthro- scopic treatment of symptomatic total knee arthroplasty. Arthroscopy 2003;19:e111-3.