807 서 론
최근 척수손상 환자에 대한 장기 생존율을 증가시키기 위해 비뇨기계 합병증을 감소시키기 위한 노력이 진행 중 이다.1 이 중 요로결석은 가장 흔한 합병증의 하나이며,2 신 기능은 악화를 초래할 수 있으므로 중요한 질환의 하나로 간주되고 있으며,3 보고된 바에 의하면 손상 후 8년간 관찰 한 신결석의 유병률은 약 7%이고,4 방광결석의 경우 약 36%이다.5 그러나 지난 30년간 보고된 통계를 보면 방광결
석의 유병률은 감소추세를 보이고 있지만,6 신결석의 경우 지난 25년간 감소하지 않아 이에 대한 위험인자를 분석할 필요가 있다고 판단하였다.7
국내에서도 척수손상 환자를 대상으로 한 다수의 연구가 발표된 바 있으나,8-11 현재까지 나온 보고에 의하면 배뇨방 법 및 척수손상의 특성에 따른 위험인자의 중요도는 아직 논쟁의 여지가 있으며, 대다수 단기간에 걸친 연구인 점을 고려하여 본 연구에서는 한국전쟁, 베트남전쟁 및 군복무 시 발생한 척수손상 환자들을 대상으로 배뇨방법 및 척수 손상의 특성에 따라 분류하고, 이에 대하여 장기간에 걸친
추적관찰 연구
Risk Factors for Urinary Stone Formation in Male Patients with Spinal Cord Injury: A 17-Year Follow-Up Study
Won Jun Choi, Ja Hyun Ku, Hong Bang Shim
From the Department of Urology, Seoul Veterans Hospital, Seoul, Korea
Purpose: This study was initiated to establish the hazard ratios for risk of urinary stone formation in chronic spinal cord injury (SCI) patients.
Materials and Methods: A total of 140 male patients who were injured before 1987 were eligible for this investigation and they were followed up on a yearly basis from January 1987 and December 2003.
Results: Over the 17 years, 39 patients (27.9%) and 21 patients (15.0%) were diagnosed with bladder and renal stones for a total of 59 and 25 episodes, respectively. On multivariate analysis, bladder stone was more common for the patients who were injured at 24 years old or older than is was for those patients who were injured at less than 24 years old (odds ratio [OR]: 2.490; 95% confidence interval [CI]: 1.092-5.677; p=0.030). In another model, the patients with complete injury had a greater risk of renal stone formation than those with incomplete injury (OR: 4.095; 95% CI: 1.295- 12.944; p=0.016). We also found that renal stone was more common for the patients with urethral catheterization (UC) than for the patients who could spontaneous void (OR: 5.668; 95% CI: 1.306-24.604; p=0.021), and for patients with bladder stone than for those without bladder stone (OR:
4.678; 95% CI: 1.447-15.126; p=0.010).
Conclusions: Injury characteristics are important for the development of urinary stone in chronic traumatic SCI patients. In addition, our findings suggest that for the cases who cannot undergo intermittent catheterization or when the bladder cannot empty spontaneously, suprapubic cystostomy is better than UC is regards to renal stone formation in this population.
(Korean J Urol 2006;47:807-812) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Key Words: Spinal cord injury, Urinary stone, Risk factors, Catheterization
대한비뇨기과학회지 제 47 권 제 8 호 2006
서울보훈병원 비뇨기과
최원준․구자현․심홍방
접수일자:2006년 2월 7일 채택일자:2006년 6월 20일
교신저자: 심홍방
서울보훈병원 비뇨기과 서울시 강동구 둔촌동 6-2 ꂕ 134-060
TEL: 02-2225-1393 FAX: 02-487-9586 E-mail: [email protected]
자료를 통해 요로결석의 위험인자를 알고자 하였다.
대상 및 방법
저자들은 1987년 1월부터 2003년 12월까지 본원에서 추 적 관찰된 외상성 척수손상 환자를 대상으로 의무기록을 후향적으로 조사하였다.
대상군은 18세 이상의 남성으로서 신경학적 손상이 확인 가능하며, 손상기전은 외상성으로 한정지었다. 또한 배뇨방 법으로는 자가 배뇨, 간헐적 청결도뇨법, 상치골방광루, 요 도유치카테터로 구분하였다. 환자 중 2년 이상 추적관찰이 되지 않는 경우나 체외 회장도관술을 시행한 환자는 본 연 구에서 제외하였다.
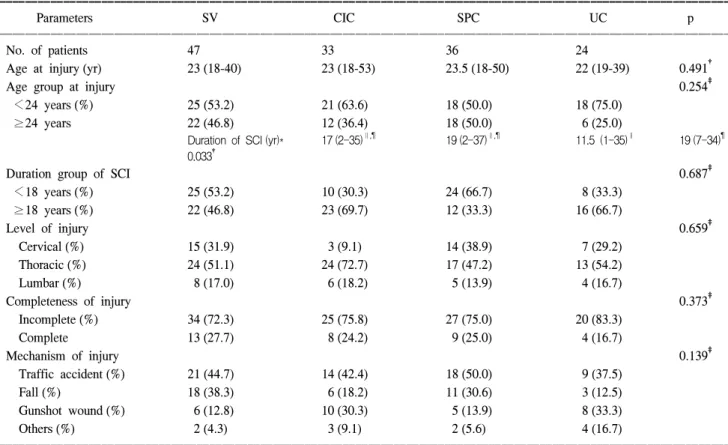
총 140명의 환자가 포함되었으며, 대상군의 배뇨방법은 자가 배뇨, 간헐적 청결도뇨법, 상치골방광루, 요도유치카 테터로 구분하였다. 대상군 중 많은 수에서 적어도 1회 이 상 배뇨방법을 변경하였기 때문에 Weld와 Dmochowski12가 기술한 바와 같이 손상 후 가장 장기간 사용된 대상군의 배뇨방법으로 결정하였다. 배뇨방법에 따라 자가 배뇨군은
47명, 간헐적 청결도뇨군은 33명, 상치골방광루군은 36명, 요도카테터군은 24명이었으며, 상치골방광루군과 요도카 테터군은 1개월 간격으로 카테터를 교환하였다.
척수손상 시 나이는 평균 24.8세 (중간값: 24, 범위: 18-53) 였으며, 척수손상 기간은 평균 16.9년 (중간값: 18, 범위:
1-37년)이었다. 척수손상 기간은 상치골방광루 군이 가장 길었으며, 요도유치카테터 군이 가장 짧았다. 총 34명 (23.3%)은 완전손상이었고, 106명 (75.7%)은 불완전손상이 었으며, 각각의 척수손상 부위는 같은 비율이었다 (Table 1).
복부단순촬영 (KUB)은 결석의 유무를 판단하기 위해 매 년 정기적으로 시행되었고, 임상적으로 결석이 의심되는 경우는 비정기적으로 시행하였다. 결석이 진단된 경우 복 부초음파 및 방광내시경을 시행하였다. 방광요관역류는 배 설성방광요관조영술을 통해 진단하였다.
본 연구에서 연속변수의 비교는 Kruskal-Wallis test를 이 용하였고, 비연속변수의 비교는 Fisher's exact test, chi- square test, 또는 Armitage test를 이용하였다. 결석의 크기나 개수 등은 분석에 고려하지 않았으며, 한 환자의 결석발생 횟수만을 고려하였다. 결석의 누적유병률 (accumulated inci-
Table 1. Clinical parameters
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Parameters SV CIC SPC UC p
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
No. of patients 47 33 36 24
Age at injury (yr) 23 (18-40) 23 (18-53) 23.5 (18-50) 22 (19-39) 0.491†
Age group at injury 0.254‡
<24 years (%) 25 (53.2) 21 (63.6) 18 (50.0) 18 (75.0)
≥24 years 22 (46.8) 12 (36.4) 18 (50.0) 6 (25.0)
Duration of SCI (yr)* 17 (2-35)∥,¶ 19 (2-37)∥,¶ 11.5 (1-35)∥ 19 (7-34)¶ 0.033†
Duration group of SCI 0.687‡
<18 years (%) 25 (53.2) 10 (30.3) 24 (66.7) 8 (33.3)
≥18 years (%) 22 (46.8) 23 (69.7) 12 (33.3) 16 (66.7)
Level of injury 0.659‡
Cervical (%) 15 (31.9) 3 (9.1) 14 (38.9) 7 (29.2)
Thoracic (%) 24 (51.1) 24 (72.7) 17 (47.2) 13 (54.2)
Lumbar (%) 8 (17.0) 6 (18.2) 5 (13.9) 4 (16.7)
Completeness of injury 0.373‡
Incomplete (%) 34 (72.3) 25 (75.8) 27 (75.0) 20 (83.3)
Complete 13 (27.7) 8 (24.2) 9 (25.0) 4 (16.7)
Mechanism of injury 0.139‡
Traffic accident (%) 21 (44.7) 14 (42.4) 18 (50.0) 9 (37.5)
Fall (%) 18 (38.3) 6 (18.2) 11 (30.6) 3 (12.5)
Gunshot wound (%) 6 (12.8) 10 (30.3) 5 (13.9) 8 (33.3)
Others (%) 2 (4.3) 3 (9.1) 2 (5.6) 4 (16.7)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*years from the injury to the start of the study (1987), †Kruskal-Wallis test, ‡Armitage test. ∥,¶The same letters indicate non-significant differences between groups based on multiple comparison test. Data are presented are medians (range) or numbers (%). SV: spontaneous voiding, CIC: clean intermittent catheterization, SPC: suprapubic cystostomy, UC: urethral catheterization, SCI: spinal cord injury
dence)은 결석 기왕력이 있는 환자 수를 총 환자 수로 나누 었고, 추적관찰 기간 동안 100명의 환자를 기준으로 하였다.
유병률은 Esclarin De Ruz 등13의 방법을 일부 수정하여, 대상 군의 총 결석 발생수를 100인년 (person-year)으로 나눈 것으 로 정의하였다. 100인년의 총수는 100명이 1년 동안 결석이 없는 것으로 정의하였다. 결석 형성에 대한 위험인자를 알기 위해 로지스틱 회귀분석을 이용하였고, 각변수의 대응위험 도 (odd ratio)와 신뢰구간을 측정하였다.
방광결석에 대한 분석에는 척수손상 당시의 연령, 척수 손상 기간, 손상 기전, 배뇨방법을 포함하였고, 신결석에 대 한 분석은 방광결석 유무와 방광요관역류를 포함시켰다.
그러나 요로감염은 척수손상 환자에 있어서 치료를 받아야 하는 시기 및 치료를 요하는 요로감염에 대한 정의가 확립 이 되지 않았으므로 본 연구에서는 제외하였으며,14 척수손 상당시의 연령 및 기간은 중간값을 기준으로 2개 군으로 분류하였다. 통계학적 유의수준은 0.05 미만으로 정하였으 며, 모든 분석은 양측검증을 시행하였다. 통계분석은 SPSS version 10.0을 사용하였다.
결 과
방광요관역류의 유병률은 12.1%였으며, 자가배뇨군은 10.6%, 간헐적 청결도뇨군은 9.1%, 상치골방광루군은 22.2%,
요도유치카테터군은 4.2%로 배뇨방법에 따른 유의한 차이 는 없었다. 방광결석과 신결석은 추적기간 동안 각각 39명 (27.9%), 21명 (15%)에서 발생하였으며, 총 결석 횟수는 각각 총 59회, 25회로 관찰되었다. 방광결석에 대한 유병률 및 누 적유병률은 상치골방광루군에서 각각 5.065/100인년과 41.7%
였으며, 간헐적 청결도뇨군에서 각각 0.891/100인년과 15.2%
였다. 신결석은 요도유치카테터군에서 8명 (33%)이었으며, 다른 배뇨방식군보다 유의하게 높았다 (Table 2).
다변량 분석에서 24세 이후 손상이 발생한 환자는 24세 이전 손상이 발생한 환자보다 방광결석이 발생할 위험도가 유의하게 높았다 (대응위험도; 2.490, 95% 신뢰구간; 1.092- 5.677, p=0.030). 그러나 손상기간에 따른 방광결석의 위험 도는 유의하지 않았다 (대응위험도; 2.108, 95%신뢰구간;
0.903-4.922, p=0.085). 완전손상 환자는 불완전손상 환자보 다 신결석 위험도가 유의하게 증가하였다 (대응위험도;
4.095, 95%신뢰구간; 1.295-12.944, p=0.016). 요도 카테터군 은 자가배뇨군보다 신결석 위험도가 증가하였으며, 방광결 석 발생도 신결석의 위험도를 증가시켰다 (대응위험도;
5.668, 95%신뢰구간; 1/447-15.126; p=0.010). 그러나 그 이외 의 변수에서는 방광결석 및 신결석발생에 유의한 영향을 주지 않았다 (Table 3).
고 찰
요로결석은 척수손상 이후 2년 이내, 특히 첫 6개월에 흔 히 발생하며 그 원인은 다양하다. 이전의 코호트 연구에서 방광결석에 대한 위험인자는 젊은 연령, 신경학적 병변의 정도, 배뇨방법 등이었다.7 8,314명을 대상으로 한 연구에서 는 수상 후 1년 이내, 연령이 45세 이상인 경우 방광결석의 위험도가 증가하였으며,4 신결석은 척수손상 1년 후부터 배 뇨방식 및 손상정도와 연관이 있다. 그러나 이전의 연구들 은 첫 번째 요로결석의 발생에만 초점을 맞추고 있으며, 재 발된 결석에 대한 분석은 포함하지 않았다.
이전의 보고에서는 장기간의 카테터 유치가 방광결석 형 성에 영향을 준다고 하였다.12,14-21 척수손상 환자에서 stru- vite 결석의 빈도는 일반인보다 높으며, 척수손상 환자에서 결석의 화학적 성분은 struvite:carbonate apatite의 비율이 손 상기간이 길수록 증가하는 것으로 보고되었다.22 그러나 일 부 보고에서 유치카테터와 요로결석의 발생은 무관하였으 며,3,23 저자들의 경우에도 장기간의 카테터가 척수환자에서 방광결석에 대한 위험도를 증가시키지 않았다.
척수손상 환자의 방광요관역류 유병률은 17-25%까지 보 고되고 있고,24 방광요관역류는 신결석의 위험인자로 알려 져 있다.25 Comarr 등25은 1,507명을 대상으로 한 연구에서 Table 2. Incidence of bladder and renal stones according to the
bladder management methods
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Parameters SV CIC SPC UC
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
No. of patients 47 33 36 24
Bladder stone Accumulated
14 (29.8) 5 (15.2) 15 (41.7)* 5 (20.8) incidence (%)
Incidence
(episodes/100 2.003 0.891 5.065 1.716 person-years)
Renal stone Accumulated
6 (12.8) 3 (9.1) 4 (11.1) 8 (33.3)† incidence (%)
Incidence
(episodes/100 0.876 0.535 0.654 2.451 person-years)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
*p<0.05 in the CIC versus the SPC group by the chi-square test.
†p<0.05 in the SV versus the UC group, the CIC versus the UC group, and the SPC versus the UC group by the Fisher’s exact test. SV: spontaneous voiding, CIC: clean intermittent catheteri- zation, SPC: suprapubic cystostomy, UC: urethral catheterization
신결석 중 29%가 방광요관역류와 관련이 있다고 보고하였 고, Hall 등26도 이와 비슷한 결과를 보고를 하였다.
상치골방광루가 방광삼각근에 부종을 유발하고, 방광삼 각근의 부종은 방광역류를 발생한다고 알려져 있다. 그러 나 저자들의 경우 방광요관역류가 17명 (12.1%)에서 발생하 였고, 이 중 상치골방광루군에서는 22%에서 발생하였으나, 다른 배뇨방식군에 비해 신결석 형성은 통계학적으로 유의 한 차이를 보이지 않았다. Mitsui 등27도 상치골 방광루군과 간헐적 청결도뇨군 간 신결석의 발생은 유의한 차이가 없 다고 하였다.
손상의 특징과 결석의 연관성에 대한 연구도 보고되었
다.21,28,29 Favazza 등21은 방광결석이 있는 환자는 더 고령이
고, 결석이 없는 환자에 비해 완전 손상일 경우 결석 형성에 대한 위험이 증가한다고 하였다. DeVivo 등28,29은 신결석이 있는 환자의 경우는 연령이 높은 환자, 사지마비 및 방광결 석의 과거력이 있는 환자라고 하였다. Donnellan과 Bolton 등30도 완전손상, 방광결석의 과거력 및 방광요관역류가 있 는 환자군에서 신결석의 발생이 높음을 보고하였다.
요로결석은 척수손상에서 가장 흔한 합병증 중 하나이 다. 그러나 기존에 보고되었던 결과들은 수상 후 수년 이내 의 결과들이고 수상 후 장기간에 걸친 방광 및 신결석에 대한 분석은 아직 보고되지 않았다. 또한 대부분의 보고들 Table 3. Multivariate risk factors of bladder and renal stones
ꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚꠚ
Bladder stone Renal stone
Parameters ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Adjusted OR Adjusted OR
p p
(95% CI) (95% CI)
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Age at injury (yr)
<24 1.000 1.000
≥24 2.490 (1.092-5.677) 0.030 0.441 (0.132-1.477) 0.184
Duration of SCI (yr)
≥18 1.000 1.000
<18 2.108 (0.903-4.922) 0.085 0.874 (0.283-2.694) 0.814
Level of injury
Cervical 1.000 1.000
Thoracic 0.809 (0.311-2.102) 0.663 0.548 (0.152-1.971) 0.357
Lumbar 0.837 (0.234-2.996) 0.785 1.463 (0.325-6.594) 0.620
Completeness of injury
Incomplete 1.000 1.000
Complete 1.361 (0.558-3.319) 0.499 4.095 (1.295-12.944) 0.016
Mechanism of injury
Traffic accident 1.000 1.000
Fall 0.758 (0.288-1.993) 0.574 0.816 (0.221-3.007) 0.759
Gunshot wound 0.715 (0.221-2.317) 0.576 1.108 (0.263-4.663) 0.888
Others 1.049 (0.207-5.308) 0.954 0.372 (0.038-3.675) 0.397
Bladder management
SV 1.000 1.000
CIC 0.526 (0.157-1.769) 0.299 0.893 (0.172-4.637) 0.892
SPC 1.474 (0.560-3.874) 0.432 0.713 (0.159-3.191) 0.659
UC 0.891 (0.244-3.254) 0.861 5.668 (1.306-24.604) 0.021
Bladder stone
No 1.000
Yes 4.678 (1.447-15.126) 0.010
VUR
No 1.000
Yes 1.762 (0.307-10.099) 0.525
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ OR: odds ratio, CI: confidence interval, SCI: spinal cord injury, SV: spontaneous voiding, CIC: clean intermittent catheterization, SPC:
suprapubic cystostomy, UC: urethral catheterization
은 첫번째 결석 형성에만 초점을 두고 있어, 재발하는 결석 에 대한 위험요소 또한 아직 알려져 있지 않다.
본 연구는 척수손상 환자에서 결석 형성에 관한 위험도 를 관찰한 것으로서 척수손상 환자에 관한 연구 중 가장 오래 추적관찰한 연구이다. 그러나 본 연구는 후향적 연구 이기 때문에 다음과 같은 몇 가지 제한점이 있다. 첫째, 방 광의 특징 및 결석의 구성 등에 관한 자료를 포함하지 못하 였다. 둘째, 본 연구는 수상 이후 처음 사용한 배뇨방식의 영향을 배제하지 못하였다. 셋째, 요로감염에 대한 영향을 배제하지 못하였다. 그러나 대상군을 배뇨방식에 따라 구 별하였고, 배뇨방식은 요로감염에 중요한 위험인자로 알려 져 있으므로, 요로감염의 영향은 일정부분 보정이 되었다 고 생각한다.
결 론
척수손상 환자에서 요로결석은 중요한 합병증 중 하나이 다. 손상 시 환자의 연령은 방광결석 형성에 영향을 주고, 손상의 정도는 신결석의 발생에 영향을 준다. 배뇨방식에 따라 방광결석 형성은 유의한 차이가 없지만, 요도유치카 테터는 신결석 발생에 유의한 위험인자이다. 그러므로 간 헐적 청결도뇨를 시행할 수 없거나, 자가 배뇨를 할 수 없는 환자에서는 요도유치카테터보다 상치골방광루가 신결석 형성의 위험도를 감소시킬 것으로 생각한다.
REFERENCES
1. Jackson AB, DeVivo M. Urological long-term follow-up in women with spinal cord injuries. Arch Phys Med Rehabil 1992;73:1029-35
2. Lee KY, Jung TY, Shim HB. Analysis of urological com- plications according to the voiding method for spinal cord injury patients. Korean J Urol 2004;45:1252-7
3. Lim SH, Park WH. Follow-up of renal function and compli- cation in spinal cord injuries. Korean J Urol 1987;28:895-900 4. Chen Y, DeVivo MJ, Roseman JM. Current trend and risk
factors for kidney stones in persons with spinal cord injury:
a longitudinal study. Spinal Cord 2000;38:346-53
5. DeVivo MJ, Fine PR, Cutter GR, Maetz HM. The risk of bladder calculi in patients with spinal cord injuries. Arch Intern Med 1985;145:428-30
6. Chen Y, DeVivo MJ, Stover SL, Lloyd LK. Recurrent kidney stone: a 25-year follow-up study in persons with spinal cord injury. Urology 2002;60:228-32
7. Chen Y, DeVivo MJ, Lloyd LK. Bladder stone incidence in persons with spinal cord injury: determinants and trends, 1973-1996. Urology 2001;58:665-70
8. So JG, Oh DJ, Lim YS, Park WH, Shim HB. Urologic complications and management in 337 spinal cord injured patients. Korean J Urol 1997;38:1075-80
9. Seo BW, Kim CI, Lee SC. An objective score to predict upper tract deterioration in spinal cord injury patient. Korean J Urol 1992;33:532-6
10. Park JS, Park WH. The Analysis of risk factors for upper urinary tract disease in spinal cord injured patients: including video urodynamic findings. Korean J Urol 2005;46:943-9 11. Song BJ, Park WH. Risk factors of bladder stone formation
in spinal cord injuries. Korean J Urol 1990;31:550-5 12. Weld KJ, Dmochowski RR. Effect of bladder management on
urological complications in spinal cord injured patients. J Urol 2000;163:768-72
13. Esclarin De Ruz A, Garcia Leoni E, Herruzo Cabrera R.
Epidemiology and risk factors for urinary tract infection in patients with spinal cord injury. J Urol 2000;164:1285-9 14. The prevention and management of urinary tract infections
among people with spinal cord injuries. National Institute on Disability and Rehabilitation Research Consensus Statement.
January 27-29, 1992. J Am Paraplegia Soc 1992;15:194-204 15. Cook JB, Smith PH. Long-term urethral catheterisation after
spinal injury. Paraplegia 1968;6:11-6
16. McGuire EJ, Savastano J. Comparative urological outcome in women with spinal cord injury. J Urol 1986;135:730-1 17. Ruutu M, Lehtonen T. Urinary tract complications in spinal
cord injury patients. Ann Chir Gynaecol 1984;73:325-30 18. Bennett CJ, Young MN, Adkins RH, Diaz F. Comparison of
bladder management complication outcomes in female spinal cord injury patients. J Urol 1995;153:1458-60
19. Ord J, Lunn D, Reynard J. Bladder management and risk of bladder stone formation in spinal cord injured patients. J Urol 2003;170:1734-7
20. Larsen LD, Chamberlin DA, Khonsari F, Ahlering TE.
Retrospective analysis of urologic complications in male patients with spinal cord injury managed with and without indwelling urinary catheters. Urology 1997;50:418-22 21. Favazza T, Midha M, Martin J, Grob BM. Factors influencing
bladder stone formation in patients with spinal cord injury. J Spinal Cord Med 2004;27:252-4
22. Burr RG. Urinary calculi composition in patients with spinal cord lesions. Arch Phys Med Rehabil 1978;59:84-8 23. Dewire DM, Owens RS, Anderson GA, Gottlieb MS, Lepor
H. A comparison of the urological complications associated with long-term management of quadriplegics with and without chronic indwelling urinary catheters. J Urol 1992;147:1069-71 24. Chisolm GD, Fair WR. Scientific foundations of urology.
Chicago: Year Book Medical; 1990;286-99
25. Comarr AE, Kawaichi GK, Bors E. Renal calculus of patients with traumatic cord lesions. J Urol 1962;87:647-56
26. Hall MK, Hackler RH, Zampieri TA, Zampieri JB. Renal calculi in spinal cord-injured patient: association with reflux,
bladder stones, and foley catheter drainage. Urology 1989;34:
126-8
27. Mitsui T, Minami K, Furuno T, Morita H, Koyanagi T. Is suprapubic cystostomy an optimal urinary management in high quadriplegics? A comparative study of suprapubic cystostomy and clean intermittent catheterization. Eur Urol 2000;38:434-8 28. DeVivo MJ, Fine PR, Cutter GR, Maetz HM. The risk of renal
calculi in spinal cord injury patients. J Urol 1984;131:857-60 29. DeVivo MJ, Fine PR. Predicting renal calculus occurrence in
spinal cord injury patients. Arch Phys Med Rehabil 1986;67:
722-5
30. Donnellan SM, Bolton DM. The impact of contemporary bladder management techniques on struvite calculi associated with spinal cord injury. BJU Int 1999;84:280-5