Renal Sympathetic Denervation Induces Acute Myocardial Inflammation through Activation of Caspase-1 and Interleukin-1β
Dong Won Lee*, Il Young Kim and Ihm Soo Kwak
Division of Nephrology, Department of Internal Medicine, Pusan National University, School of Medicine, Yangsan 50612, Korea Received January 31, 2018 /Revised February 22, 2018 /Accepted February 22, 2018
Efferent and afferent sympathetic nerves are closely related to the development of hypertension and heart failure. Catheter-based renal sympathetic denervation (RDN) is implemented as a strategy to treat resistant hypertension. We investigated whether RDN procedure causes inflammatory damage on myocardium in the early phase of sympathetic denervation. Twenty-five female swine were divided into 3 groups: normal control (Normal, n=5), sham-operated control (Sham, n=5), and RDN groups (RDN, n=15). The RDN group was further subdivided into 3 subgroups according to the time of sacri- fice: immediately (RDN-0, n=5), 1 week (RDN-1, n=5), and 2 weeks (RDN-2, n=5) after RDN. There were no significant changes in the clinical parameters between the normal control and sham-operated group using contrast-media. In the myocardium, inflammatory cytokines, IL-1β and TNF-α increased at the first week, and then decreased at the second week after RDN. Anti-inflammatory cytokine, IL-10 increased immediately, and then decreased at the second week after RDN. Caspase-1 activity and apoptosis-associated speck-like protein containing a caspase recruitment domain (ASC) expression in- creased immediately after RDN until the second week. However, nucleotide-binding oligomerization domain, leucine rich repeat and pyrin domain containing protein 3 (NLRP3) expression did not show any significant differences among the groups. The RDN can cause acute myocardial inflammation through activation of caspase-1 and IL-1β. We should pay attention to protecting against early in- flammatory myocardial damage after RDN.
Key words : Cytokines, heart failure, inflammasomes, myocardium, sympathectomy
*Corresponding author
*Tel : +82-55-360-2359, Fax : +82-55-360-1605
*E-mail : [email protected]
This is an Open-Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Life Science 2018 Vol. 28. No. 2. 240~246 DOI : https://doi.org/10.5352/JLS.2018.28.2.240
Introduction
Treatment-resistant hypertension is defined as the failure to achieve target blood pressure (BP) despite the concomi- tant use of maximally tolerated doses of at least three differ- ent antihypertensive agents, including a diuretic [4, 18]. The percentage of patients achieving an adequate BP target re- mains low [5, 24], thus creating the need for alternative inter- ventional strategies. Recently, endovascular catheter-based radiofrequency renal sympathetic denervation (RDN) has been introduced to denervate efferent and afferent renal sympathetic nerve fibers selectively [13, 21, 22]. Renal func- tion, as assessed by serum creatinine (SCr), estimated glo- merular filtration rate (eGFR), and cystatin C concentration, was unchanged from baseline at 6 months after RDN, sug-
gesting that the procedure itself, and associated hemody- namic changes, have no adverse effects on the kidneys.
In the Renal Denervation for Hypertension (DENERHTN) trial, RDN plus standardized stepped-care antihypertensive treatment (SSAHT) showed more decreases in ambulatory BP compared with the same SSAHT alone at 6 months. This additional BP lowering effect might contribute to a reduction in cardiovascular morbidity if maintained in the long term after RDN [1, 20]. In experimentally induced heart failure, RDN has been associated with some improvements in renal and cardiac function. Those studies demonstrated reductions in left ventricular filling pressure, myocardial fibrosis and baroreceptor-mediated cardiac sympathetic nerve activity, and increased β-adrenergic receptor expression [3, 16, 23].
In the aspect of chronic safety, renal function was re- ported to be unchanged from baseline, however, there have been no reports about the short-term safety of myocardium following RDN procedure. The aim of this study was to in- vestigate whether RDN causes acute inflammatory damage on myocardium, using early inflammatory biomarkers such as IL-18, caspase-1, apoptosis-associated speck-like protein containing a caspase recruitment domain (ASC), and nucleo-
tide-binding oligomerization domain, leucine rich repeat and pyrin domain containing protein 3 (NLRP3) inflamma- some.
Materials and Methods
Twenty-five juvenile female swine (aged 5±0.6 months, mean weight 36.5±1.8 kg) were used. The care of the animals complied with the Guides for the Care and Use of Laboratory Animals published by the United States National Institute of Health (publication No. 85-23, revised 1996). The experi- ment was performed at the Preclinical Trial and Training Center (Pusan National University Yangsan Hospital, Yang- san, Korea), and it was approved by the Ethics Committee of our institution, Pusan National University Yangsan Hospital. Midazolam 0.5 mg/kg and ketamine 15 mg/kg were administered intravenously and the trachea was intubated. Ventilation was performed and general anesthesia was maintained using 1~2% isoflurane and oxygen. An 8-French introducer sheath was inserted into the right femo- ral artery using modified Seldinger’s technique. Continuous electrocardiogram and blood pressure monitoring was performed. A heparin bolus of 100 U/kg was administered intravenously. An 8-French guiding catheter was inserted to engage each renal artery and both renal angiograms were obtained using non-ionic contrast media, iohexol (Omni- paqueTM, 300 mgI/ml, GE Healthcare, Fairfield, CT, USA, Little Chalfont, UK) 1 ml/kg (0.5 ml/kg each) for the con- firmation of normal renal arterial anatomy[27]. Normal con- trol group (Normal) was sacrificed without any procedure.
In sham operated group using contrast-media (Sham), renal denervation catheter was inserted into each renal artery without radiofrequency energy delivery, which was sacri- ficed immediately after renal angiogram. Actual RDN was performed in group RDN-0, RDN-1 and RDN-2 using the SymplicityTM Renal Denervation System (Medtronic, Santa Rosa, CA, USA). The RDN catheter was positioned proximal to the bifurcation of each renal artery and the impedance of each electrode was checked to identify wall attachment.
Radiofrequency ablation was applied consecutively and a number of either 5 or 6 ablation points were created at each renal arteries. The impedance, temperature and radio- frequency energy delivery were monitored and recorded during the procedure [27]. When the RDN procedure was completed, bilateral renal angiograms were obtained again and signs of renal artery irregularities, such as vasospasm,
stenosis or dissection, were checked.
Blood and urine samples were collected at the time of sacrifice by inferior vena cava puncture and urinary bladder puncture, respectively. We measured blood urea nitrogen (BUN), serum creatinine (Cr), lactate dehydrogenase (LDH), C-reactive protein (CRP), cystatin C and random spot urine protein/creatinine ratio (UPCR). Myocardium samples were harvested at the time of sacrifice, and stored at -80℃. Tissue samples were homogenized mechanically (TissueLyser, QAIGEN) in a PBS-based buffer containing proteinase in- hibitor and non-ionic detergent (Tween-20). Tissue extrac- tion was done from the supernatant with neutral buffer (PBS with 0.15% Tween-20). Interleukin (IL)-1α, -1β, -18, -6, -10, and tumor necrosis factor (TNF)-α were determined using tissue lysate by Porcine Cytokine Magnetic, 6 Plex Kit (Milliplex◯RMAP, catalog number PCYTMAG-23K-06) (Merck Millipore, Billerica, MA, USA). Caspase-1 activity was meas- ured by Pig caspase-1 ELISA kit (catalog number CSB- EL004543PI) (CUSABIO, Wuhan, China). ELISA was per- formed according to the manufacturer’s instructions. Protein samples were separated on either 8 or 15% SDS-PAGE gels.
Gels were transferred to nitrocellulose membranes and blocked with 5% milk protein. Membranes were incubated at 4℃ overnight with primary antibodies. Immunoblot anal- yses of ASC and NLRP3 were performed with the following primary antibodies: 1) a purified rabbit anti-ASC polyclonal antibody (1:1,000) (catalog number bs-6741R) (Bioss, Woburn, MA, USA), 2) a goat anti-human NLRP3 polyclonal antibody (1:200) (catalog number MBS241660) (MyBioSource, San Diego, CA, USA).
Statistical analysis was performed using SPSS for Win- dows, version 21.0 (SPSS Inc., Chicago, IL, USA). Non-nor- mally distributed data were analyzed by the nonparametric Kruskal-Wallis test. Multiple group comparisons were per- formed using analysis of variance (ANOVA) with post-test according to Mann-Whitney U. A p-value of <0.05 was con- sidered statistically significant. Values were expressed as means ± SE.
Results and Discussion
Renal somatic afferent nerves to central sympathetic drive and efferent sympathetic signaling to the kidneys are closely related to the development of hypertension and heart failure [7, 12]. Renal sympathetic nerve activation enhances nora- drenaline production, while renal denervation results in a
Table 1. Clinical parameters in acute renal and myocardial injury after RDN
Normal Sham RDN-0 RDN-1 RDN-2
BUN (mg/dl) SCr (mg/dl) LDH (U/L) CRP (mg/L) CysC (mg/L) UPCR (mg/g)
6.4±0.4 0.9±0.1 745.3±24.1 0.09±0.04 0.00±0.00 154.5±16.7
7.1±1.7 0.9±0.0 796.3±46.1 0.02±0.00 0.00±0.00 153.8±1.5
9.0±0.5 1.1±0.0 1159.7±132.3*
0.09±0.01 0.17±0.09 188.8±9.7
6.6±0.7 1.3±0.0 1131.0±166.7*
0.02±0.00 0.27±0.03 150.4±22.8
8.9±1.1 1.2±0.0 836.0±18.9**
0.03±0.01 0.27±0.03 118.9±17.3 Normal normal control group, Sham sham-operated group using contrast-media, RDN-0 renal sympathetic denervation (RDN) group sacrificed immediately after RDN, RDN-1 RDN group sacrificed 1 week after RDN, RDN-2 RDN group sacrificed 2 weeks after RDN, Hb hemoglobin, BUN blood urea nitrogen, SCr serum creatinine, LDH lactate dehydrogenase, CRP C-reactive protein, CysC cystatin C, UPCR random spot urine protein/creatinine ratio, UACR random spot urine albumin/creatinine ratio. *p<0.05, vs. normal control group; **p<0.05, vs. RDN-1
Fig. 1. Clinical parameter. Serum LDH increased immediately after RDN (p<0.05, Normal vs. RDN-0 and RDN-1, re- spectively), and then decreased at the 2nd week (p<0.05, RDN-1 vs. RDN-2). Normal normal control group, Sham sham-operated group using contrast-media, RDN-0 re- nal sympathetic denervation (RDN) group sacrificed im- mediately after RDN, RDN-1 RDN group sacrificed 1 week after RDN, RDN-2 RDN group sacrificed 2 weeks after RDN.
marked decrease of noradrenaline by up to 95%[2, 6, 10, 11].
Experimental studies of heart failure have demonstrated some improvements in cardiac and renal function through ablation of sensory afferent and/or efferent sympathetic nerve fibers by RDN [3, 16, 23]. However, we hypothesized that RDN might cause acute subclinical inflammatory dam- age on myocardium, especially in the early phase of sym- pathetic denervation. BUN, serum Cr, cystatin C, CRP and UPCR showed no significant differences between the groups (Table 1). Serum LDH levels increased immediately after RDN until the 1st week (p<0.05, Normal vs. RDN-0 and RDN-1, respectively), and then decreased at the 2nd week (p<0.05, RDN-1 vs. RDN-2) (Fig. 1).
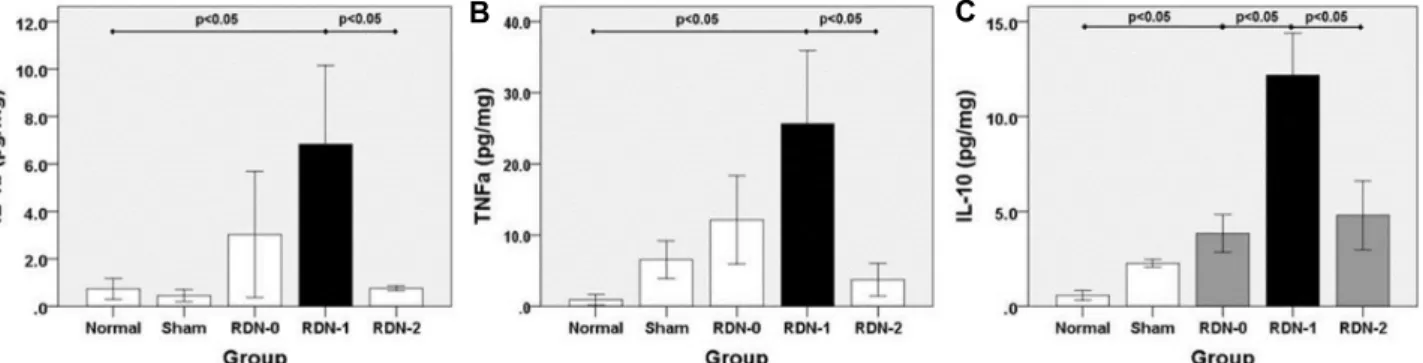
IL-1β and TNF-α levels were increased at the 1st week (p<0.05, Normal vs. RDN-1, respectively), and then decreased at the 2nd week after RDN (p<0.05, RDN-1 vs. RDN-2, re- spectively) (Fig. 2A, Fig. 2B). However, IL-1α, -18 and -6 lev- els showed no significant differences between the groups (p=NS, Normal vs. RDN-0 and RDN-1, respectively) (Fig. 3A, Fig. 3B, Fig. 3C). Anti-inflammatory IL-10 level increased im- mediately after RDN (p<0.05, Normal vs. RDN-0 and RDN-1, respectively), and then decreased at the 2nd week (p<0.05, RDN-1 vs. RDN-2) (Fig. 2C). Casapse-1 activity increased im- mediately and continuously until the 2nd week after RDN (p<0.05, Normal vs. Sham and RDN-0, and RDN-0 vs.
RDN-1, respectively), and showed a tendency to decrease at the 2nd week after RDN (p=NS, RDN-1 vs. RDN-2) (Fig.
4). Myocardial ASC expression increased immediately after RDN (p<0.05, Normal vs. RDN-0 and RDN-1, and RDN-0 vs. RDN-1, respectively), and then decreased at the 2nd week (p<0.05, RDN-1 vs. RDN-2). However, myocardial NLRP3 expression did not show any significant differences among the groups (p=NS, Normal vs. RDN-0, RDN-1 and RDN-2, respectively) (Fig. 5). The inflammasome is a molec- ular complex that contains NLRP proteins and an adaptor protein, ASC [15, 25]. The most fully characterized in- flammasome is the NLRP3 inflammasome which contains the NLRP3 protein [26]. Pro-inflammatory caspase-1, which is activated by inflammasome complexes in response to pathogen-associated molecular patterns (PAMPs) and dam- age-associated molecular patterns (DAMPs), converts IL-1β and -18 to their active forms [8, 14]. The inflammasome is activated mainly in inflammatory cells, where it plays an important role in the innate immune response, and causes tissue inflammation and apoptosis [25, 26]. Recent clinical studies showed that RDN significantly reduced cardiac sym-
A B C
Fig. 2. Pro-inflammatory and anti-inflammatory cytokines associated with myocardial damage after RDN. (A) IL-1β, and (B) TNF-α levels increased at the 1st week (p<0.05, Normal vs. RDN-1, respectively), and then decreased at the 2nd week after RDN (p<0.05, RDN-1 vs. RDN-2, respectively). (C) IL-10 levels increased immediately after RDN (p<0.05, Normal vs. RDN-0 and RDN-1, respectively), and then decreased at the 2nd week (p<0.05, RDN-1 vs. RDN-2).
A B C
Fig. 3. Pro-inflammatory and inflammatory cytokines associated with myocardial damage after RDN. (A) IL-1α, (C) IL-18, and (D) IL-6 showed no significant differences among the groups (p=NS, Normal vs. RDN-0 and RDN-1, respectively).
Fig. 4. Caspase-1 activity associated with myocardial damage after RDN. Caspase-1 activity increased immediately af- ter RDN (p<0.05, Normal vs. Sham and RDN-0, and RDN- 0 vs. RDN-1, respectively; p=NS, RDN-1 vs. RDN-2).
pathetic activity, independently from its BP effects, and were associated with lower atrial fibrillation recurrence and im- proved echocardiographic parameters [9, 19]. An animal
study showed that both cardiac sympathetic denervation and renal sympathetic denervation induced similar effects on ventricular electrophysiologic properties, thus signifi- cantly reducing the heart rate, prolonged QT interval, the ventricular effective refractory period, and the action poten- tial duration [17]. Another animal study demonstrated that RDN attenuated and stabilized left ventricular remodeling after myocardial infarction via the regulation of the matrix metalloproteinase (MMP)-9/tissue inhibitor of matrix metal- loproteinase (TIMP)-1 balance in the transforming growth factor (TGF)-β1 signaling pathway [28]. However, in our study, myocardial IL-1β, -10, TNF-α, ASC levels and cas- pase-1 activity increased after RDN procedure. This my- ocardial damage in the early phase of sympathetic denerva- tion is thought to be associated with the activation of cas- pase-1 and inflammatory cytokines, but not NLRP3 in- flammasome. We thought that other NLRP pathway such as NLRP1 can activate caspase cascade, and we need more experiments to evaluate the role of other inflammasomes in the experimentally induced heart failure model.
Fig. 5. ASC and NLRP3 expression associated with myocardial damage after RDN. Myocardial ASC (24 kDa) expression increased at the first week after RDN (p<0.05, Normal vs. RDN-1) and then decreased at the 2nd week (p<0.05, RDN-1 vs. RDN-2).
Myocardial NLRP3 (118 kDa) expression did not show any significant differences among the groups (p=NS, Normal vs.
RDN-0, RDN-1, and RDN-2, respectively). In the densitometric analysis of the immunoblots, data are presented as pro- tein/GAPDH ratios plotted on the y-axis. GAPDH was used as the loading control and did not vary among the groups.
Representative immunoblots of at least 3 separate experiments.
In conclusion, RDN could cause acute myocardial damage through activation of caspase-1 and IL-1β. The inflammatory damage was transient and reversible. However, we should pay attention to protecting against early inflammatory my- ocardial damage after RDN.
Acknowledgements
This work was supported by Research Institute for Convergence of Biomedical Science and Technology, and Preclinical Trial and Training Center, Pusan National University Yangsan Hospital.
References
1. Azizi, M., Sapoval, M., Gosse, P., Monge, M., Bobrie, G., Delsart, P., Midulla, M., Mounier-Véhier, C., Courand, P., Lantelme, P., Denolle, T., Dourmap-Collas, C., Trillaud, H., Pereira, H., Plouin, P. and Chatellier, G. Renal Denervation for Hypertension (DENERHTN) investigators. 2015. Opti- mum and stepped care standardised antihypertensive treat- ment with or without renal denervation for resistant hyper-
tension (DENERHTN): a multicentre, open-label, rando- mised controlled trial. Lancet 385, 1957-1965.
2. Barajas, L., Powers, K. and Wang, P. 1984. Innervation of the renal cortical tubules: a quantitative study. Am. J.
Physiol. 247, F50-F60.
3. Booth, L., Schlaich, M., Nishi, E., Yao, S., Xu, J., Ramchandra, R., Lambert, G. and May, C. 2015. Short-term effects of cath- eter-based renal denervation on cardiac sympathetic drive and cardiac baroreflex function in heart failure. Int. J.
Cardiol. 190, 220-226.
4. Chobanian, A., Bakris, G., Black, H., Cushman, W., Green, L., Izzo, J. L. Jr., Jones, D., Materson, B., Oparil, S., Wright, J. Jr. and Roccella, E. National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. 2003. The seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treat- ment of High Blood Pressure: the JNC 7 report. JAMA. 289, 2560-2572.
5. Cutler, J., Sorlie, P., Wolz, M., Thom, T., Fields, L. and Roccella, E. 2008. Trends in hypertension prevalence, aware- ness, treatment, and control rates in United States adults between 1988-1994 and 1999-2004. Hypertension 52, 818-827.
6. DiBona, G. and Kopp, U. 1997. Neural control of renal
function. Physiol. Rev. 77, 75-197.
7. DiBona, G. 2005. Physiology in perspective: the wisdom of the body. Neural control of the kidney. Am. J. Physiol. Regul.
Integr. Comp. Physiol. 289, R633-R641.
8. Dinarello, C. 1996. Biologic basis for interleukin-1 in disease.
Blood 87, 2095-2147.
9. Donazzan, L., Mahfoud, F., Ewen, S., Ukena, C., Cremers, B., Kirsch, C., Hellwig, D., Eweiwi, T., Ezziddin, S., Esler, M. and Böhm, M. 2016.ellH Effects of catheter-based renal denervation on cardiac sympathetic activity and innervation in patients with resistant hypertension. Clin. Res. Cardiol. 105, 364-371.
10. Esler, M. 2000. The sympathetic system and hypertension.
Am. J. Hypertens. 13, S99-S105.
11. Elser, M., Rumantir, M., Kaye, D., Jennings, G., Hastings, J., Socratous, F. and Lambert, G. 2001. Sympathetic nerve biology in essential hypertension. Clin. Exp. Pharmacol.
Physiol. 28, 986-989.
12. Esler, M. 2010. The 2009 Carl Ludwig Lecture: pathophysiol- ogy of the human sympathetic nervous system in cardiovas- cular diseases: the transition from mechanism to medical management. J. Appl. Physiol. 108, 227-237.
13. Esler, M., Krum, H., Sobotka, P., Schlaich, M., Schmieder, R. and Böhm, M. 2010. Renal sympathetic denervation in patients with treatment-resistant hypertension (the Symplic- ity HTN-2 Trial): a randomized controlled trial. Lancet 376, 1903-1909.
14. Fantuzzi, G., Puren, A., Harding, M., Livingston, D. and Dinarello, C. 1998. Interleukin-18 regulation of interferon gamma production and cell proliferation as shown in inter- leukin-1 beta-converting enzyme (caspase-1)-deficient mice.
Blood 91, 2118-2125.
15. Franchi, L., Eigenbrod, T., Muñoz-Planillo, R. and Nuñez, G. 2009. The inflammasome: a caspase-1-activation paltform that regulates immune responses and disease pathogenesis.
Nat. Immunol. 10, 241-247.
16. Hu, J., Li, Y., Cheng, W., Yang, Z., Wang, F., Lv, P., Niu, C., Hou, Y., Yan, Y. and Ge, J. 2014. A comparison of the efficacy of surgical renal denervation and pharmacologic therapies in post-myocardial infarction heart failure. PLoS One 9, e96996.
17. Huang, B., Yu, L., He, B., Wang, S., Lu, Z., Liao, K., Wang, Z., Zhou, X., He, W. and Jiang, H. 2015. Sympathetic de- nervation of heart and kidney induces similar effects on ventricular electrophysiological properties. EuroIntervention 11, 598-604.
18. James, P., Oparil, S., Carter, B., Cushman, W., Dennison-
Himmelfarb, C., Handler, J., Lackland, D., LeFevre, M., MacKenzie, T., Ogedegbe, O., Smith, S. Jr., Svetkey, L., Taler, S., Townsend, R., Wright, J. Jr., Narva, A. and Ortiz, E.. 2014. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 311, 507-520.
19. Kiuchi, M. G., Chen, S., E. Silva, G. R., Paz, L. M., Kiuchi, T., de Paula Filho, A. G. and Souto, G. L. 2016. Pulmonary vein isolation alone and combined with renal sympathetic denervation in chronic kidney disease patients with re- fractory atrial fibrillation. Kidney Res. Clin. Pract. 35, 237-244.
20. Kjeldsen, S., Fadl Elmula, F. and Persu, A. 2015. The setback of renal denervation should not backfire on sympathetic overactivity in hypertension. J. Am. Coll. Cardiol. 65, 1322- 1323.
21. Krum, H., Schlaich, M., Whitbourn, R., Sobotka, P., Sadowski, J., Bartus, K., Kapelak, B., Walton, A., Sievert, H., Thambar, S., Abraham, W. T. and Esler, M. 2009. Catheter-based renal sympathetic denervation for resistant hypertension: multi- centre safety and proof-of-principle cohort study. Lancet 373, 1275-1281.
22. Krum, H., Sobotka, P., Mahfoud, F., Böhm, M., Esler, M.
and Schlaich, M. 2011. Device-based antihypertensive ther- apy: therapeutic modulation of the autonomic nervous system. Circulation 123, 209-215.
23. Li, Z., Jiang, H., Chen, D., Liu, Q., Geng, J., Guo, J., Sun, R., Zhu, G. and Shan, Q. 2015. Renal sympathetic denerva- tion improves cardiac dysfunction in rats with chronic pres- sure overload. Physiol. Res. 64, 653-662.
24. Sarafidis, P. and Bakris, G. 2008. Resistant hypertension, An overview of evaluation and treatment. J. Am. Coll. Cardiol.
52, 1749-1757.
25. Schroder, K. and Tschopp, J. 2010. The inflammasomes. Cell 140, 821-832.
26. Schroder, K., Zhou, R. and Tschopp, J. 2010. The NLRP3 inflammasome: a sensor for metabolic danger? Science 327, 296-300.
27. Tsioufis, C., Papademetriou, V., Dimitriadis, K., Tsiachris, D., Thomopoulos, C., Park, E., Hata, C., Papalois, A. and Stefanadis, C. 2013. Catheter-based renal sympathetic de- nervation exerts acute and chronic effects on renal hemody- namics in swine. Int. J. Cardiol. 168, 987-992.
28. Zheng, X., Li, X., Lyu, Y., He, Y., Wan, W., Zhu, H. and Jiang, X. 2016. Possible mechanism by which renal sym- pathetic denervation improves left ventricular remodeling after myocardial infarction. Exp. Physiol. 101, 260-271.
초록:교감신경절제술(RDN) 후 caspase-1과 interleukin-1β 활성화로 인해 유발된 염증성 급성심 근손상
이동원*․김일영․곽임수
(부산대학교 의과대학 내과학교실, 신장내과)
원심성, 구심성 교감신경 신호는 고혈압 및 심부전의 발생과 밀접한 관련이 있다. 혈관 내 카테터를 이용한 교 감신경절제술(RDM)은 난치성 고혈압의 대체치료로 시행되어 왔다. 시술과 관련하여 장기간 신장의 안정성에 대 해서는 보고가 있었으나 단기간 심근의 안정성에 대한 연구 결과는 없었다. 저자들은 RDN 시술로 인한 교감신경 차단 후 염증성 심근손상이 발생할 수 있음을 가정하여 실험으로 검증하고자 하였다. 25마리의 암컷돼지를 3군으 로 나누고–정상대조군(n=5), Sham군(n=5), RDN 시술군(n=15)–RDN 시술군을 시술 후 sacrifice 시기에 따라 다 시 세분하였다–시술 후 즉시 sacrifice한 RDN-0 (n=5), 시술 1주 후 sacrifice한 RDN-1 (n=5), 시술 2주 후 sacrifice 한 RDN-2 (n=5). 조영제의 영향을 배제하기 위해 설정했던 Sham군과 정상대조군 간에는 의미있는 차이를 보이 지 않았다. IL-1β, TNF-α 등의 염증 싸이토카인은 시술 1주 후 증가하여 2주째 감소하였다. 항염증 싸이토카인 IL-10은 시술 직후부터 증가하여 2주째 감소하였다. Inflammasome에 의해 위험신호(danger signal)를 전달받고 활성화되는 Caspase-1 및 inflammasome을 매개하는 도메인 ASC는 시술 직후 활성화되어 발현이 증가하였고 2 주까지 지속되었다. 그러나 caspase-1을 매개할 것으로 추정되었던 NLRP3 inflammasome의 발현은 의미있는 차 이를 보이지 않았다. RDN 시술에 의한 교감신경차단은 caspase-1, IL-1β 등의 활성화에 의해 염증성 심근손상을 초래할 수 있으며 RDN 시술 후에는 그 위험성을 고려해야 하겠다. NLRP3 외에 다른 NLRP inflammasome path- way의 관련성에 대한 추가연구가 필요하다.