40
•교신저자:김기호, 동국대학교 의과대학 비뇨기과학교실 경북 경주시 석장동 1090-1 우 780-350 Tel: 054-770-8265, Fax: 054-771-0769 E-mail: [email protected] Received: March 2, 2010
Accepted: March 26, 2010
클라미디아 감염 진료지침
동국대학교 의과대학 비뇨기과교실
김 기 호[Abstract]
Clinical Guideline of Chlamydia Trachomatis Infection Ki Ho Kim
From the Department of Urology, College of Medicine, Dongguk University, Gyeongju, Korea
Sexually transmitted diseases (STD) are a major public health problem because their incidence is increasing worldwide despite prevention campaigns and because they raise the risk of HIV infection. Chlamydia trachomatis is the most prevalent bacterial sexually transmitted infection. Several thousands of cases still remain undiagnosed. Chlamydia infections are most often asymptomatic and can cause pelvic inflammatory disease and infertility to women and epididymo-orchitis to men. At present, there is no guideline for management of chlamydia infection in our country so it will help the patients and physicians to treat chlamydia infection and to make the suitable guideline for our country that we know about recent trends of Chlamydia infection guideline.
The objective of this study is to know about recent trends of Chlamydia infection guideline focusing on Scottish Intercollegiate Guidelines Network (SIGN) guideline publicated at 2009 and Center for Disease Control and Prevention (CDC) and Canadian guideline publicated at 2006 and World Health Organization (WHO) guideline publicated at 2003. (Korean J UTII 2010;5:40-50)
Key Words: Chlamydia trachomatis, Management, Guideline
서 론
요로생식기내 클라미디아와 임균감염은 그 증상 이 비특이적이거나, 무증상 감염이 흔하며, 특히 클
라미디아의 경우 여성 감염자의 80%, 남성 감염자
의 50%가 무증상 감염자이다.
1이 경우 정확한 진
단 및 적절한 치료 없이 방치되는 경우가 대부분이
며, 치료의 지연은 심각한 후유증을 초래할 수 있
고 또한 성적 파트너에게 계속적인 전파가 이루어
질 수 있다. 그러나 클라미디아 감염에 대한 진료
지침은 우리나라에서는 아직 마련되지 않았으며
많은 나라에서도 자기나라 실정에 맞는 진료지침이
마련되지 못한 것이 현실이다. 현재까지 2006년
Center for Disease Control and Prevention (CDC)
guideline과 2003년 World Health Organization (WHO)
에서 나온 진료지침이 많은 나라에서 참고하고 있
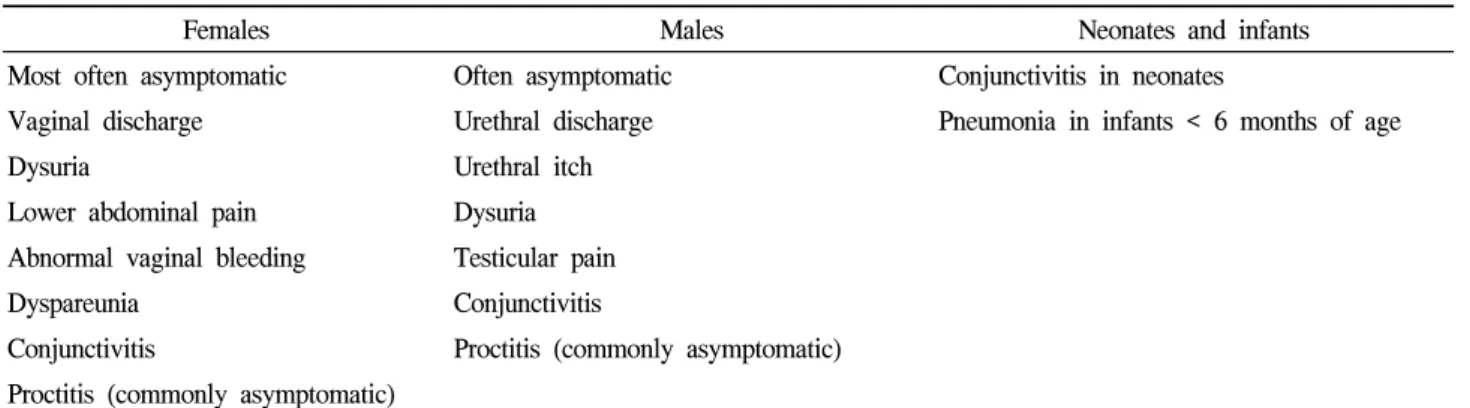
Table 1. Symptoms and sign
Females Males Neonates and infants
Most often asymptomatic Often asymptomatic Conjunctivitis in neonates
Vaginal discharge Urethral discharge Pneumonia in infants < 6 months of age
Dysuria Urethral itch
Lower abdominal pain Dysuria
Abnormal vaginal bleeding Testicular pain
Dyspareunia Conjunctivitis
Conjunctivitis Proctitis (commonly asymptomatic) Proctitis (commonly asymptomatic)
다. 2006년에 작성된 CDC와 캐나다 진료지침, 2009 년 Scottish Intercollegiate Guidelines Network (SIGN) 진료지침을 중심으로 최근 클라미디아 감염의 진료지 침의 최근 경향이 어떻게 되는지 알아보도록 하겠다.
본 론
병인이 되는 균은 Chlamydia trachomatis serovars D부터 K까지 이며, 전염병예방법 3군에 속하고 표 본감시대상 전염병으로 전국 보건소 및 300 여개 표본 의료기관을 중심으로 발생현황을 파악하고 있다. 2006년 이후 증가양상을 보이고 있으며 2007 년 3,196명, 2008년 3,501명으로 꾸준한 증가 추세 에 있다.
2,3남성의 경우 클라미디아에 대한 보균자 가 많지만 증상이 없어 선별검사로 관리하는 경우 는 드물다.
4-6노출에서 감염이 발생되기까지 잠복기 간은 보통 2∼3주이지만 6주까지 길어질 수 있다.
치료를 하지 않으면 감염은 수개월간 지속된다. N.
gonorrhoeae에 감염된 사람들은 종종 C. trachomatis 와 동시 감염된다.
5,6위험 인자는 클라미디아에 감 염된 사람과 성적 접촉을 한 경우, 지난 해에 새로 운 성파트너 또는 2명 이상의 성파트너와 접촉한 경우, 전에 성전파성 감염이 있었던 경우, 상처받기 쉬운 사람 (예; 마약중독자, 수감자, 성매매 종사자, 길거리의 젊은이) 등이 있다. 25세 이하의 성활동 성이 활발한 모든 여성은 선별검사를 받아야 하며 증상이 없는 젊은 남성에 대해서는 선별검사가 추 천되지 않는다.
5,7-16또한 모든 임산부 여성들은 산
전검사시 선별검사를 받아야 하며 재감염의 위험 성이 높거나 양성인 임산부는 임신 3기 동안 선별 검사를 받아야 한다.
17-231. 임상양상
50%에서 증상이 없으며 여성에서는 질분비물, 성 교통, 하복부통 및 배뇨통, 비정상적 질출혈 등이 있 을 수 있고 질검사시 자궁부속기 통증과 자궁경부에 분비물 등이 있을 수 있다.
24-40남성에서는 요도분비 물과 배뇨통이 있을 수 있고 부고환염 등으로 인한 고환통과 발적이 생길 수 있다
41-43(Table 1). 1% 미 만에서 반응성 관절염이 있을 수 있으며 드물게 직 장에 감염을 일으킬 수 있다. 또한 간주위염때문에 우측 갈비아래부위 통증이 생길 수 있다.
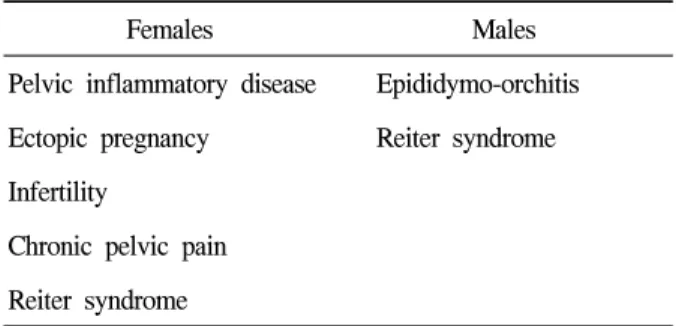
44-48주요 합병증으로 여성에서는 골반염, 자궁외 임신, 불임, 만성 골반통, 라이터 증후군 등이 있고 남성에서는 고환-부고환염, 라이터 증후군 등이 있다 (Table 2).
2. 선별검사
클라미디아에 대한 선별검사를 시행함으로써 생
식기계의 합병증으로의 이환율과 사망률를 줄일 수
있으며 질병의 빈도와 유병률을 줄일 수 있다. 16∼39
세에서의 클라미디아의 유병률은 남성에서 2.8%, 여
성에서 3.6%이며 25세 이하의 젊은 사람에서의 유병
률은 남성에서 5.1%, 여성에서 6.2%로 높다.
49클라미
디아에 양성인 사람의 성파트너는 검사를 꼭 받아
Table 2. Major sequelae
Females Males
Pelvic inflammatory disease Epididymo-orchitis Ectopic pregnancy Reiter syndrome Infertility
Chronic pelvic pain Reiter syndrome
야 하며 클라미디아가 의심되고 진단되어지지 않은 사람의 성파트너도 꼭 검사를 받아야 한다. 12개월 이내 클라미디아로 진단된 사람의 재감염률도 21∼
29배로 매우 높기 때문에 꼭 검사를 받아야 한다.
5015세 이상 25세 이하의 여성인 경우 그 보다 나이 가 많은 경우에 비해 클라미디아 감염이 더 흔하 다.
51또한 가임이 끝난 모든 여성도 클라미디아에 대한 검사를 시행 받아야 한다.
52-566개월 후 클라미 디아 감염이 있는 사람은 재감염을 예방하기 위해서 파트너는 평가, 검사, 치료 및 상담을 받을 필요가 있으며, 두 파트너의 치료가 끝날 때까지 환자 및 접촉한 사람들은 성관계를 금해야 한다.
18,57-603. 진단
NAATs (polymerase chain reaction [PCR], tran- scription-mediated amplification [TMA])는 배양, enzyme immunoassay (EIA) 그리고 direct fluorescent antibody assay (DFA) 보다 더 민감하고 특이적이다. Standard polymerase chain reaction (sPCR), real time polymerase chain reaction (rtPCR), strand displacement amplification (SDA), transcription mediated amplification (TMA), nu- cleic acid sequence based amplification (NASBA)의 5가 지 형태의 NAATs가 사용되어지고 있다. 클라미디아 감염을 진단하는데 있어 TMA와 SDA가 특이도와 민 감도가 높아서 추천되어지며 rtPCR은 TMA와 SDA을 사용할 수 없을 때 사용할 수 있다.
614. 검체수집
NAATs는 가능하다면 소변이나 요도, 자궁경부에 서부터 채취한 검체를 사용해야만 한다. 혈액과 점 액은 NAAT의 수행을 방해할 수 있으며 위음성의 결과를 보일 수 있어 배양이 권장된다. NAAT는 연 구 목적이 아닌 경우 질에서 채취한 검체는 사용할 수 없다. 목구멍과 직장에서 채취한 검체에서 NAAT를 적절하게 평가할 수 없기 때문에 배양이 추천된다. 사춘기나 그 이후의 여성에서는 자궁경부 에서 검체를 채취하고 수술적으로 자궁경부가 없다 면 소변이나 요도 swab, 직장 swab, 질 swab을 채취 하여 배양을 시행해야 한다. 남성인 경우 첫 소변이 가장 좋으며 사춘기 이전의 여성인 경우 소변이나 질, 직장 swab을 채취하여 배양을 시행한다.
10,626개 월 이하의 환아인 경우 코인두 흡입물에서 채취한 검체로 배양을 시행한다.
5. 치료
검사의 결과를 기다릴 필요없이 증상이 있는 경 우 바로 치료를 시행해야 한다. 골반염이 있는 경우 불임의 위험성이 커지기 때문에 지체없이 치료를 시행해야 하며 파트너도 바로 치료해야 한다.
29,63클 라미디아 검사에서 양성, 클라미디아 감염에 적합한 증상이 있는 경우, 성파트너의 클라미디아 감염, 동 시감염의 가능성 (20∼42%) 때문에 N. gonorrhoeae 가 진단될 때 경험적 동시치료를 시행한다. 치료를 받은 사람은 재감염의 위험성을 최소화하기 위해 모 든 파트너가 치료될 때까지 금욕해야 하며 약물복용 이 끝난 시점에서 7일간 금욕해야 한다.
1개의 메타분석 연구에서 azithromycin 1g 한번 쓰는 것이 7일간의 doxycycline 100mg 하루 2회 사 용하는 만큼 높은 치료율을 보이고 효과적으로 치 료할 수 있으며 부작용에 있어서도 차이가 없다고
하였다.
64-73환자의 순응도가 떨어지는 경우 azi-
thromycin 1g 한번 쓰는 것으로 치료해야 한다.
Ofloxacin은 doxycycline 그리고 azithromycin과 비슷
한 효과를 보이지만 훨씬 비싸고 여러 번 사용해야
Table 3. Adults (non-pregnant and non-lactating): urethral, endocervical, rectal, conjunctival infection
Preferred Alternative
• Doxycycline 100mg PO bid for 7 days OR
• Ofloxacin 300mg PO bid for 7 days OR
• Azithromycin 1g PO in a single dose if poor compliance is expected*
• Erythromycin 2g/day PO in divided doses for 7 days+ OR
• Erythromycin 1g/day PO in divided doses for 14 days+
• Tetracyclin 500mg orally, 4 times a day for 7 days
• Amoxycillin 500mg orally, 3 times a day for 7 days
• Levofloxacin 500mg orally once daily for 7 days
*If vomiting occurs more than 1 hour post-administration, a repeat dose is not required.
+Erythromycin dosages refer to erythromycin base. Equivalent dosages of other formulations may be substituted (with the exception of the estolate formulation which is contraindicated in pregnancy). If erythromycin has been used for treatment, a test of cure should be performed 3∼4 weeks after completion of therapy.
한다.
74-82Erythromycin은 azithromycin이나 doxycy-
cline에 비해 효과적이지 않고 다른 약제에 비해 위 장관 장애가 높다.
82-86임신시 erythromycin을 사용한 다면 erythromycin base가 추천되며 estolate를 제외하 고 다른 약을 대체할 수 있다. 만약 erythromycin을 치료제로 사용한다면 치료 종결 후 3∼4주에 치료 에 대한 테스트를 시행해야 한다. 임산부에서의 azi- thromycin에 대한 한정된 자료가 있지만 많은 전문 가들은 안전한 것으로 생각한다.
87-92Doxycycline과 quinolone 제재는 임산부와 수유중인 산모에게는 금기이다. 약제내성은 드물지만 최근 이슈가 되고 있다.
93,94각각의 진료지침의 치료부분에서 많은 차이가 나 지는 않고 비슷한 치료약제와 복용방법을 보이지 만 다른 부분도 있다. 캐나다 및 WHO, CDC, European guideline에서는 성인 (임산부가 아니고 수 유하고 있지 않은 사람)의 요도, 자궁경내막, 직장, 결막 감염인 경우, doxycycline 100mg 하루 두 번 7 일간 사용 혹은 azithromycin 1g 경구 하루 한번 사 용을 모두 추천한다. 대체약제에서 약간의 차이가 있는데 공통적인 것은 ofloxacin 300mg 하루 2회 7 일간 경구 투여 혹은 erythromycin 2g을 7일간 경구 투여하는 것이며 차이점은 캐나다에서는 eryth- romycin 1g을 14일간 경구 투여를, WHO에서는
amoxicillin 500mg을 하루에 3번 7일간 사용 및 tet- racycline 500mg을 하루 4번 7일간 사용을, CDC에 서는 erythromycin ethylsuccinate 800mg을 하루 4번 7일간 혹은 levofloxacin 500mg을 하루 한번 7일간 사용을, 유럽에서는 ofloxacin 200mg 하루 2번 7일 간 혹은 roxithromycin 150mg 하루 두번 7일간 혹은 clarithromycin 250mg 하루 두 번 7일간 사용을 추 천하고 있다 (Table 3).
임산부와 모유수유 중인 엄마의 요도, 자궁경내
막, 직장 감염시 공통적으로 amoxicillin 500mg 하
루 세 번 7일간 경구 투여, erythromycin 2g 7일간
경구 투여, erythromycin 1g 14일간 경구 투여, azi-
thromycin 1g 하루 한번 경구 투여를 추천하였으며
WHO에서는 erythromycin 2g을 7일간 사용, amox-
icillin 500mg을 하루 세번 7일간 사용만 추천하고
있다. CDC에서는 amoxicillin 혹은 azithromycin의
사용을 추천하고 erythromycin ethylsuccinate 800mg
하루 네번 7일간 혹은 erythromycin ethylsuccinate
400mg 하루 네번 14일간 사용을 대체할 수 있다고
하였다. 유럽에서는 erythromycin base 2g을 7일간,
amoxicillin 500mg 하루 세번 7일간 및 josamycin
750mg을 하루 두번 7일간 사용을 추천하며 eryth-
romycin base 1g을 14일간 사용 및 erythromycin eth-
ylsuccinate 800mg을 하루 네번 7일간 혹은 eryth-
Table 4. Pregnant women and nursing mothers: urethral, endocervical, rectal infection
• Amoxicillin 500mg PO tid for 7 days OR*
• Erythromycin 2g/day PO in divided doses for 7 days OR*+
• Erythromycin 1g/day PO in divided doses for 14 days OR*+
• Azithromycin 1g PO in a single dose, if poor compliance is expected‡
• Erythromycin ethylsuccinate 800mg orally 4 times a day for 7 days
• Erythromycin ethylsuccinate 400mg orally 4 times a day for 14 days
*If erythromycin or amoxicillin has been used for treatment in nursing mothers, test of cure should be performed 3∼4 weeks after the completion of treatment.
+Erythromycin dosage refers to the use of erythromycin base. Equivalent dosages of other formulations may be substituted (with the exception of the estolate formulation, which is contraindicated in pregnancy). Gastrointestinal side effects are more severe with erythromycin than with amoxicillin.
‡If vomiting occurs more than 1 hour post-administration, a repeat dose is not required.
Note: Test of cure should be performed 3∼4 weeks after the completion of treatment in all pregnant women.
romycin ethylsuccinate 400mg을 하루 네번 14일간 사용, azithromycin 하루 한번 사용을 대체할 수 있 다고 하였다 (Table 4). Erythromycin estolate는 임신 시 금기이며 간손상을 일으킬 수 있다. 이렇듯 약 물치료에 있어 전체적인 추천약은 비슷하지만 각 각의 진료지침에 따라 추천약과 대체약에 있어 약 간의 차이는 있다.
소아에서는 각각의 진료지침에 따른 큰 차이는 보이지 않는다. 용량에 있어 약간의 차이가 날 뿐 약제에 대해서 비슷한 추천을 하고 있다. 결막염을 보이는 환아인 경우 클라미디아 감염뿐만 아니라 N. gonorrhoeae에 대해서 같이 치료를 시행해야 한 다. 25세 이하의 젊은 산모인 경우 매우 높은 감염 의 위험성을 지니고 있기 때문에 산전진찰을 시행 함으로써 클라미디아 감염을 예방할 수 있다. 신생 아 시기에 클라미디아 감염은 출생 후 5∼12일쯤 결막염 형태로 흔히 온다. 또한 1∼3개월 때 열이 없는 비급성 폐렴으로 올 수 있다. 결막염시 눈꺼 풀을 외번시켜서 dacron-tipped swab 또는 검체 kit 를 사용하여 얻어진 swab으로부터 검체를 얻어야 하며 폐렴인 경우 비인두에서 검체를 얻어야 한다.
Microimmunofluorescence test를 시행하기도 하지만
널리 사용되어지지 않으며 IgM 항원이 1:32 이상인 경우 클라미디아 폐렴을 강력히 시사한다. 45kg 미만 의 소아의 결막염과 폐렴인 경우 erythromycin 50mg/kg/day로 하루 네번 나누어 10∼14일간 복용한 다. 45kg 이상이고 8세 미만이거나 8세 이상인 소아 는 azithromycin과 같은 성인에서와 같은 약제와 복용 법을 사용한다. 6주 이내의 소아에게 erythromycin의 사용은 infantile hypertrophic pyloric stenosis (IHPS)을 일으킬 수 있다.
95-98다른 macrolide (azithromycin, clarithromycin)와 IHPS의 연관성은 알려져 있지 않지 만 erythromycin의 사용 후 득과 실에 대해서 보호자 에게 충분히 설명해야 한다. Erythromycin을 사용할 때 IHPS의 증상과 징후를 관찰하는 것이 중요하다.
국소 항생제만 사용하는 것은 클라미디아 감염 치료 에 추천되지 않으며 전신치료시 불필요하다. Silver nitrate와 같은 점안액을 신생아에게 쓰는 것은 엄마 로부터의 클라미디아 감염의 전파를 예방하지는 못 하지만 임질의 전파는 예방할 수 있다.
6. 배우자에게 보고
증상이 처음으로 나타나거나 증상은 없지만 진
단된 날짜로부터 60일 이내 성관계를 가졌던 모든 파트너는 검사 및 치료를 받아야 한다. 만약 이 기 간 동안 파트너가 없었다면 마지막 파트너가 검사 받고 치료받아야 한다. 증상이 있는 남성인 경우 증상이 처음으로 나타나기 이전 30일 이내 모든 파 트너는 검사 및 치료를 받아야 한다. 또한 여성이 거나 증상이 없는 남성은 최근에 만났던 성파트너 또는 최근 6개월 이내의 모든 파트너는 검사 및 치 료를 받아야 한다.
7. 추적관찰
적절한 치료를 받고 증상이나 징후가 없어지고 치료받지 않은 파트너에 재노출 되지 않았다면 클 라미디아에 대한 배양검사는 일반적으로 시행하지 않는다. 그러나 환자의 순응도가 떨어지거나 대안 의 치료요법을 사용하고 있거나 모든 사춘기 이전 의 어린이와 모든 임산부는 배양검사를 받아야 한 다. 죽은 미생물에 의한 위양성을 피하기 위해 치 료가 되었는지에 대한 검사는 효과적인 치료를 끝 내고 3∼4주 후에 시행한다. 배양, EIA/ELISA, DNA hybridization은 치료를 끝내고 2주 후에 시행 하며 클라미디아 감염이 있는 모든 사람들은 재감 염의 위험이 높기 때문에 치료 6개월 후 반복검사 를 받아야 한다. 적절한 치료 후에도 감염이 지속 되는 경우는 약물복용을 정확하게 하지 않았거나 끝내지 못한 경우, 치료받지 않은 파트너에게 재노 출된 경우, 새로운 파트너로부터의 감염, 위양성, 드물지만 약물저항 등을 고려해야 한다. 또한 지속 적인 증상을 보이는 경우 다른 병원균에 의한 감염 과 감염이 아닌 다른 원인을 생각해야 한다. 재감 염시 골반염과 다른 합병증이 발생할 위험이 크다.
치료완결에 대한 검사로써 PCR은 추천되지 않으며 3개월에 HIV, B형 간염, 매독에 대한 혈청학적 검 사를 시행해야 한다.
결 론
클라미디아 감염은 최근 다른 성전파성 질환에 비해 증가하고 있는 추세이고 증상이 없어 진단 및
치료가 늦어져 불임과 같은 심한 합병증을 유발할 수 있기 때문에 적극적인 진단 및 치료가 시행되어 야 한다. 특히 임산부인 경우 출산 후 소아에게 감 염을 일으켜 결막염이나 폐렴을 일으킬 수 있으므 로 클라미디아 감염에 대한 좀 더 적극적인 환자교 육과 보건당국의 관심이 필요하며 의사 및 환자 또 한 클라미디아 감염에 대한 적극적인 진단 및 치료 가 필요하다. 최근에 발표된 클라미디아 감염에 대 한 진료지침은 클라미디아 감염에 대한 증상이 있 다면 실험실적 진단이 나오기 전에 적극적인 치료 를 할 것을 권고하고 있다. 성인인 경우 doxycy- cline이나 azithromycin 등을 사용하여 적극적인 치 료를 해야하며 임산부인 경우는 amoxillin 및 eryth- romycin과 같은 안전한 항생제를 사용하고 소아인 경우 erythromycin을 사용할 수 있으나 득과 실을 잘 생각하여 선택해야 한다.
REFEENCES
1. Stamm WE. Chlamydia trachomatis infections: progress and problems. J Infect Dis 1999;179:380-3
2. Korea Centers for Disease Control and Prevention. 2009 STD guidelines, 2009 (http://stat.cdc.go.kr/kcdchome/jsp/ob- servation/stat/sot/STATSOT0702List.jsp)
3. Lee JK. Report from a Korea Centers for Disease Control and Prevention 2007. KCDC, 2008;98:127-30 4. Chen MY, Donovan B. Screening for genital Chlamydia
trachomatis infection: are men the forgotten reservoir?
Med J Aust 2003;179:124-5
5. Andersen B, Olesen F, Moller JK, Ostergaard L.
Population-based strategies for outreach screening of urogenital Chlamydia trachomatis infections: a random- ized, controlled trial. J Infect Dis 2002;185:252-8 6. Ginocchio RH, Veenstra DL, Connell FA, Marrazzo
JM. The clinical and economic consequences of screen- ing young men for genital chlamydial infection. Sex Transm Dis 2003;30:99-106
7. Marrazzo JM, White CL, Krekeler B, Celum CL, Lafferty WE, Stamm WE, et al. Community-based urine screening for Chlamydia trachomatis with a ligase chain reaction assay. Ann Intern Med 1997;127:796-803 8. Marrazzo JM, Whittington WL, Celum CL, Handsfield
HH, Clark A, Cles L, et al. Urine-based screening for Chlamydia trachomatis in men attending sexually trans- mitted disease clinics. Sex Transm Dis 2001;28:219-25 9. Braverman PK, Biro FM, Brunner RL, Gilchrist MJ,
Rauh JL. Screening asymptomatic adolescent males for chlamydia. J Adolesc Health Care 1990;11:141-4 10. Chernesky MA, Jang D, Lee H, Burczak JD, Hu H,
Sellors J, et al. Diagnosis of Chlamydia trachomatis in- fections in men and women by testing first-void urine by ligase chain reaction. J Clin Microbiol 1994;32:2682-5 11. LaMontagne DS, Fine DN, Marrazzo JM. Chlamydia
trachomatis infection in asymptomatic men. Am J Prev Med 2003;24:36-42
12. Marrazzo JM, Celum CL, Hillis SD, Fine D, DeLisle S, Handsfi eld HH. Performance and cost-effectiveness of selective screening criteria for Chlamydia trachomatis in- fection in women. Implications for a national Chlamydia control strategy. Sex Transm Dis 1997;24:131-41 13. Moncada J, Schachter J, Shafer MA, Williams E,
Gourlay L, Lavin B, et al. Detection of Chlamydia tra- chomatis in first catch urine samples from symptomatic and asymptomatic males. Sex Transm Dis 1994;21:8-12 14. Domeika M, Bassiri M, Mardh PA. Diagnosis of geni-
tal Chlamydia trachomatis infections in asymptomatic males by testing urine by PCR. J Clin Microbiol 1994;
32:2350-2
15. Anestad G, Berdal BP, Scheel O, Mundal R, Odinsen O, Skaug K, et al. Screening urine samples by leuko- cyte esterase test and ligase chain reaction for chlamy- dial infections among asymptomatic men. J Clin Microbiol 1995;33:2483-4
16. Ciemins EL, Kent CK, Flood J, Klausner JD.
Evaluation of chlamydia and gonorrhea screening cri- teria: San Francisco sexually transmitted disease clinic:
1997 to 1998. Sex Transm Dis 2000;27:165-7
17. Davies HD, Wang EE. Periodic health examination, 1996 update: 2. Screening for chlamydial infections. Canadian Task Force on the Periodic Health Examination. CMAJ 1996;154:1631-44
18. Sexually transmitted diseases treatment guidelines 2002.
Centers for Disease Control and Prevention. MMWR Recomm Rep 2002;51(RR-6):1-78
19. Cohen I, Veille JC, Calkins B. Improved pregnancy outcome following successful treatment of chlamydial
infection. JAMA 1990;263:3160-3
20. Ryan GM Jr, Abdella TN, McNeeley SG, Baselski VS, Drummond DE. Chlamydia trachomatis infection in pregnancy and effect of treatment on outcome. Am J Obstet Gynecol 1990;162:34-9
21. Black-Payne C, Ahrabi MM, Bocchini JA Jr, Ridenour CR, Brouillette RM. Treatment of Chlamydia trachoma- tis identifi ed with Chlamydiazymeduring pregnancy.
Impact on perinatal complications and infants. J Reprod Med 1990;35:362-7
22. Schachter J, Sweet RL, Grossman M, Landers D, Robbie M, Bishop E. Experience with the routine use of erythromycin for chlamydial infections in pregnancy.
N Engl J Med 1986;314:276-9
23. McMillan JA, Weiner LB, Lamberson HV, Hagen JH, Aubry RH, Abdul-Karim RW, et al. Efficacy of mater- nal screening and therapy in the prevention of chlamy- dia infection of the newborn. Infection 1985;13:263-6 24. Cates W, Jr, Wasserheit JN. Genital chlamydial in-
fections; epidemiology and reproductive sequelae. Am J Obstet Gynecol 1991;164(6 Pt 2):1771-81
25. Addiss DG, Vaughn ML, Ludka D, Pfister J, Davis JP.
Decreased prevalence of Chlamydia trachomatis in- fection associated with a selective screening program in family planning clinics in Wisconsin. Sex Transm Dis 1993;20(1):28-35
26. Coste J, Laumon B, Brémond A, Collet P, Job-Spira N. Sexually transmitted diseases as major causes of ec- topic pregnancy: results from a large case-control study in France. Fertil Steril 1994;62(2):289-95
27. Cromer BA, Heald FP. Pelvic inflammatory disease asso- ciated with Neisseria gonorrhoeae and Chlamydia trachoma- tis: clinical correlates. Sex Transm Dis 1987;14(3):125-9 28. Garland SM, Johnson B. Chlamydia trachomatis in-
fections--the Royal Women's Hospital experience. Med J Aust 1989;150(4):174-7
29. Hillis SD, Joesoef R, Marchbanks PA, Wasserheit JN, Cates W Jr, Westrom L. Delayed care of pelvic in- flammatory disease as a risk factor for impaired fertility. Am J Obstet Gynecol 1993;168(5):1503-9 30. Horner PJ, Hay PE, Thomas BJ, Renton AM,
Taylor-Robinson D, May PE, et al. The role of Chlamydia trachomatis in urethritis and urethral symp- toms in women. Int J STD AIDS 1995;6(1):31-4
31. Humphreys JT, Henneberry JF, Rickard RS, Beebe JL.
Cost-benefit analysis of selective screening criteria for Chlamydia trachomatis infection in women attending Colorado family planning clinics. Sex Transm Dis 1992;19(1):47-53
32. Kamwendo F, Forslin L, Bodin L, Danielsson D.
Programmes to reduce pelvic inflammatory disease--the Swedish experience. Lancet 1998;351 Suppl 3:25-8 33. Krettek JE, Arkin SI, Chaisilwattana P, Monif GR.
Chlamydia trachomatis in patients who used oral con- traceptives and had intermenstrual spotting. Obstet Gynecol 1993;81:728-31
34. Lindner LE, Geerling S, Nettum JA, Miller SL, Altman KH. Clinical characteristics of women with chlamydial cervicitis. J Reprod Med 1988;33(8):684-90
35. Malotte CK, Wiesmeier E, Gelineau KJ. Screening for chlamydial cervicitis in a sexually active university population. Am J Public Health 1990;80(4):469-71 36. Oakeshott P, Chiverton S, Speight L, Bertrand J.
Testing for cervical Chlamydia trachomatis infection in an inner city practice. Fam Pract 1992;9(4):421-4 37. Padian NS, Washington AE. Pelvic inflammatory disease.
A brief overview. Ann Epidemiol 1994;4(2):128-32 38. Scott GR, Thompson C, Smith IW, Young H. Infection
with Chlamydia trachomatis and Neisseria gonorrhoeae in women with lower abdominal pain admitted to a gy- naecology unit. Br J Obstet Gynaecol 1989;96(4):473-7 39. Sellors JW, Pickard L, Gafni A, Goldsmith CH, Jang
D, Mahony JB, et al. Effectiveness and efficiency of selective vs universal screening for chlamydial infection in sexually active young women. Arch Intern Med 1992;152(9):1837-44
40. Weinstock HS, Bolan GA, Kohn R, Balladares C, Back A, Oliva G. Chlamydia trachomatis infection in wom- en: a need for universal screening in high prevalence populations? Am J Epidemiol 1992;135(1):41-7
41. Berger RE, Alexander ER, Harnisch JP, Paulsen CA, Monda GD, Ansell J, et al. Etiology, manifestations and therapy of acute epididymitis: prospective study of 50 cases. J Urol 1979;121(6):750-4
42. De Jong Z, Pontonnier F, Plante P, Gautier JR, Ioualalen A, Archambaud M, et al. The frequency of Chlamydia trachomatis in acute epididymitis. Br J Urol 1988;62(1):76-8
43. Eley A, Oxley KM, Spencer RC, Kinghorn GR, Ben-Ahmeida ET, Potter CW. Detection of Chlamydia trachomatis by the polymerase chain reaction in young patients with acute epididymitis. Eur J Clin Microbiol Infect Dis 1992;11(7):620-3
44. Keat AC, Thomas BJ, Taylor-Robinson D, Pegrum GD, Maini RN, Scott JT. Evidence of Chlamydia trachoma- tis infection in sexually acquired reactive arthritis. Ann Rheum Dis 1980;39(5):431-7
45. Silveira LH, Gutiérrez F, Scopelitis E, Cuéllar ML, Citera G, Espinoza LR. Chlamydia-induced reactive arthritis. Rheum Dis Clin North Am 1993;19(2):351-62 46. Taylor-Robinson D, Thomas BJ, Dixey J, Osborn MF,
Furr PM, Keat AC. Evidence that Chlamydia trachoma- tis causes seronegative arthritis in women. Ann Rheum Dis 1988;47(4):295-9
47. Jones RB, Rabinovitch RA, Katz BP, Batteiger BE, Quinn TS, Terho P, et al. Chlamydia trachomatis in the pharynx and rectum of heterosexual patients at risk for genital infection. Ann Intern Med 1985;102(6):757-62 48. Dalaker K, GjøciRnaess H, Kvile G, Urnes A, Anestad
G, Bergan T. Chlamydia trachomatis as a cause of acute perihepatitis associated with pelvic inflammatory disease. Br J Vener Dis 1981;57(1):41-3
49. Low N, McCarthy A, Macleod J, Salisbury C, Campbell R, Roberts TE, et al. Epidemiological, social, diagnostic and economic evaluation of population screening for genital chlamydial infection. Health Technol Assess 2007 Mar;11(8):iii-iv, ix-xii, 1-165. Review.
50. Scott Lamontagne D, Baster K, Emmett L, Nichols T, Randall S, McLean L, et al. Incidence and reinfection rates of genital chlamydial infection among women aged 16-24 years attending general practice, family planning and genitourinary medicine clinics in England: a pro- spective cohort study by the Chlamydia Recall Study Advisory Group. Sex Transm Infect 2007;83(4):292-303 51. Adams EJ, Charlett A, Edmunds WJ, Hughes G.
Chlamydia trachomatis in the United Kingdom: a sys- tematic review and analysis of prevalence studies. Sex Transm Infect 2004;80(5):354-62
52. Morton K, Regan L, Spring J, Houang E. A further look at infection at the time of therapeutic abortion.
Eur J Obstet Gynecol Reprod Biol 1990;37(3):231-6 53. Sørensen JL, Thranov I, Hoff G, Dirach J. Early- and
late-onset pelvic inflammatory disease among women with cervical Chlamydia trachomatis infection at the time of induced abortion-a follow-up study. Infection 1994;22(4):242-6
54. Skjeldestad FE, Tuveng J, Solberg AG, Molne K, Dalen A, Buhaug H. Induced abortion: Chlamydia tra- chomatis and postabortal complications. A cost benefit analysis. Acta Obstet Gynecol Scand 1988;67(6):525-9 55. Wein P, Kloss M, Garland SM. Postabortal pelvic sep-
sis in association with Chlamydia trachomatis. Aust N Z J Obstet Gynaecol 1990;30(4):347-50
56. Penney GC, Thomson M, Norman J, McKenzie H, Vale L, Smith R, et al. A randomised comparison of strat- egies for reducing infective complications of induced abortion. Br J Obstet Gynaecol 1998;105(6):599-604 57. Whittington WL, Kent C, Kissinger P, Oh MK,
Fortenberry JD, Hillis SE, et al. Determinants of per- sistent and recurrent Chlamydia trachomatis infection in young women: results of a multicenter cohort study.
Sex Transm Dis 2001;28:117-23
58. Schillinger JA, Kissinger P, Calvet H, Whittington WL, Ransom RL, Sternberg MR, et al. Patient-delivered part- ner treatment with azithromycin to prevent repeated Chlamydia trachomatis infection among women: a randomized, controlled trial. Sex Transm Dis 2003;30:
49-56
59. Gunn RA, Fitzgerald S, Aral SO. Sexually transmitted disease clinic clients at risk for subsequent gonorrhea and chlamydia infections: possible "core" transmitters.
Sex Transm Dis 2000;27:343-9
60. Rietmeijer CA, Van Bemmelen R, Judson FN, Douglas JM Jr. Incidence and repeat infection rates of Chlamydia trachomatis among male and female patients in an STD clinic: implications for screening and rescreening. Sex Transm Dis 2002;29:65-72
61. Cook RL, Hutchison SL, Østergaard L, Braithwaite RS, Ness RB. Systematic review: noninvasive testing for Chlamydia trachomatis and Neisseria gonorrhoeae. Ann Intern Med 2005;142(11):914-25
62. Quinn TC, Welsh L, Lentz A, Crotchfelt K, Zenilman J, Newhall J, et al. Diagnosis by AMPLICOR PCR of Chlamydia trachomatis infection in urine samples from women and men attending sexually transmitted disease clinics. J Clin Microbiol 1996;34(6):1401-6
63. Horner PJ, Caul EO. National guideline for the man- agement of Chlamydia trachomatis genital tract infection. Clinical Effectiveness Group (Association of Genitourinary Medicine and the Medical Society for the Study of Venereal Diseases). Sex Transm Infect 1999;75 Suppl 1:S4-8
64. Hillis SD, Coles FB, Litchfield B, Black CM, Mojica B, Schmitt K, et al. Doxycycline and azithromycin for prevention of chlamydial persistence or recurrence one month after treatment in women. A use-effectiveness study in public health settings. Sex Transm Dis 1998;
25:5-11
65. Hammerschlag MR, Golden NH, Oh MK, Gelling M, Sturdevant M, Brown PR, et al. Single dose of azi- thromycin for the treatment of genital chlamydial in- fections in adolescents. J Pediatr 1993;122:961-5 66. Johnson RB. The role of azalide antibiotics in the
treatment of Chlamydia. Am J Obstet Gynecol 1991;
164(6 Pt 2):1794-6
67. Marra F, Marra C, Patrick DM. Cost-effectiveness anal- ysis of azithromycin for Chlamydia trachomatis in- fection in women: a Canadian perspective. Can J Infect Dis 1997;8:202-8
68. Martin DH, Mroczkowski TF, Dalu ZA, McCarty J, Jones RB, Hopkins SJ, et al. A controlled trial of a single dose of azithromycin for the treatment of chla- mydial urethritis and cervicitis. The Azithromycin for Chlamydial Infections Study Group. N Engl J Med 1992;327:921-5
69. Nilsen A, Halsos A, Johansen A, Hansen E, Tøcifrud E, Moseng D, et al. A double blind study of single dose azithromycin and doxycycline in the treatment of chla- mydial urethritis inmales. Genitourin Med 1992;68:325-7 70. Nuovo J, Melnikow J, Paliescheskey M, King J, Mowers R. Cost-effectiveness analysis of five different antibiotic regimens for the treatment of uncomplicated Chlamydia trachomatis cervicitis. J Am Board Fam Pract 1995;8:7-16
71. Ossewaarde JM, Plantema FHF, Rieffe M, Nawrocki RP, De Vries A, van Loon AM. Efficacy of single-dose azithromycin versus doxycycline in the treatment of cer- vical infections caused by Chlamydia trachomatis. Eur J Clin Microbiol Infect Dis 1992;11:693-7
72. Thorpe EM Jr, Stamm WE, Hook EW 3rd, Gall SA,
Jones RB, Henry K, et al. Chlamydial cervicitis and urethritis: single dose treatment compared with doxycy- cline for seven days in community based practises.
Genitourin Med 1996;72:93-7
73. Lau CY, Qureshi AK. Azithromycin versus doxycycline for genital chlamydial infections: a meta-analysis of random- ized clinical trials. Sex Transm Dis 2002;29:497-502 74. Judson FN, Beals BS, Tack KJ. Clinical experience
with ofloxacin in sexually transmitted disease. Infection 1986;14(suppl 4):S309-S10
75. Fransen L, Avonts D, Piot P. Treatment of genital chla- mydial infection with ofloxacin. Infection 1986;14(suppl 4):S318-S20
76. Batteiger BE, Jones RB, White A. Efficacy and safety of ofloxacin in the treatment of nongonococcal sexually transmitted disease. Am J Med 1989;87(6C):75S-7S 77. Nayagam AT, Ridgway GL, Oriel JD. Efficacy of
ofloxacin in the treatment of non-gonococcal urethritis in men and genital infections caused by Chlamydia tra- chomatis in men and women. J Antimicrob Chemother 1988;22(suppl C):155-8
78. Maiti H, Chowdhury FH, Richmond SJ, Stirland RM, Tooth JA, Bhattacharyya MN, et al. Ofloxacin in the treatment of uncomplicated gonorrhea and chlamydial genital infection. Clin Ther 1991;13:441-7
79. Faro S, Martens MG, Maccato M, Hammill HA, Roberts S, Riddle G. Effectiveness of ofloxacin in the treatment of Chlamydia trachomatis and Neisseria gon- orrhoeae cervical infection. Am J Obstet Gynecol 1991;
164(5 Pt 2):1380-3
80. Hooton TM, Batteiger BE, Judson FN, Spruance SL, Stamm WE. Ofloxacin versus doxycycline for treatment of cervical infection with Chlamydia trachomatis.
Antimicrob Agents Chemother 1992;36:1144-6
81. Kitchen VS, Donegan C, Ward H, Thomas B, Harris JR, Taylor-Robinson D. Comparison of ofloxacin with doxycycline inthe treatment of non-gonococcal urethritis and cervical chlamydial infection. J Antimicrob Chemother 1990;26(suppl D):99-105
82. Mogabgab WJ, Holmes B, Murray M, Beville R, Lutz FB, Tack KJ. Randomized comparison of ofloxacin and doxycycline for chlamydia and ureaplasma urethritis and cervicitis. Chemotherapy 1990;36:70-6
83. Linnemann CC Jr, Heaton CL, Ritchey M. Treatment
of Chlamydia trachomatis infections: comparison of 1- and 2-g doses of erythromycin daily for seven days.
Sex Transm Dis 1987;14:102-6
84. Cramers M, Kaspersen P, From E, Moller BR.
Pivampicillin compared with erythromycin for treating women with genital Chlamydia trachomatis infection.
Genitourin Med 1988;64:247-8
85. Scheibel JH, Kristensen JK, Hentzer B, Secher L, Ullman S, Verdich J, et al. Treatment of chlamydial urethritis in men and Chlamydia trachomatis-positive female partners: comparison of erythromycin and tetra- cycline in treatment courses of one week. Sex Transm Dis 1982;9:128-31
86. Bowie WR, Manzon LM, Borrie-Hume CJ, Fawcett A, Jones HD. Efficacy of treatment regimens for lower ur- ogenital Chlamydia trachomatis infection in women.
Am J Obstet Gynecol 1982;142:125-9
87. Kacmar J, Cheh E, Montagno A, Peipert JF. A randomized trial of azithromycin versus amoxicillin for the treatment of Chlamydia trachomatis in pregnancy.
Infect Dis Obstet Gynecol 2001;9:197-202
88. Wehbeh HA, Ruggeirio RM, Shahem S, Lopez G, Ali Y. Single-dose azithromycin for Chlamydia in pregnant women. J Reprod Med 1998;43:509-14
89. Adair CD, Gunter M, Stovall TG, McElroy G, Veille JC, Ernest JM. Chlamydia in pregnancy: a randomized trial of azithromycin and erythromycin. Obstet Gynecol 1998;91:165-8
90. Bush MR, Rosa C. Azithromycin and erythromycin in the treatment of cervical chlamydial infection during pregnancy. Obstet Gynecol 1994;84:61-3
91. Genc MR. Treatment of genital Chlamydia trachomatis infection in pregnancy. Best Pract Res Clin Obstet Gynaecol 2002;16:913-22
92. Jacobson GF, Autry AM, Kirby RS, Liverman EM, Motley RU. A randomized controlled trial comparing amoxicillin and azithromycin for the treatment of Chlamydia trachomatis in pregnancy. Am J Obstet Gynecol 2001;184:1352-4
93. Somani J, Bhullar VB, Workowski KA, Farshy CE, Black CM. Multiple drugresistant Chlamydia trachoma- tis associated with clinical treatment failure. J Infect Dis 2000;181:1421-7
94. Misyurina OY, Chipitsyna EV, Finashutina YP, Lazarev
VN, Akopian TA, Savicheva AM, et al. Mutations in a 23S rRNA gene of Chlamydia trachomatis associated with resistance to macrolides. Antimicrob Agents Chemother 2004;48:1347-9
95. Sorensen HT, Skriver MV, Pedersen L, Larsen H, Ebbesen F, Schonheyder HC. Risk of infantile hyper- trophic pyloric stenosis after maternal postnatal use of macrolides. Scand J Infect Dis 2003;35:104-6
96. Cooper WO, Griffi n MR, Arbogast P, Hickson GB, Gautam S, Ray WA. Very early exposure to eryth-
romycin and infantile hypertrophic pyloric stenosis.
Arch Pediatr Adolesc Med 2002;156:647-50
97. Mahon BE, Rosenman MB, Kleiman MB. Maternal and infant use of erythromycin and other macrolide anti- biotics as risk factors for infantile hypertrophic pyloric stenosis. J Pediatr 2001;139:380-4
98. Honein MA, Paulozzi LJ, Himelright IM, Lee B, Cragan JD, Patterson L, et al. Infantile hypertrophic pyloric stenosis after pertussis prophylaxis with erythromcyin: a case review and cohort study. Lancet 1999;354:2101-5