Korean J Gastroenterol Vol. 71 No. 2, 103-106 https://doi.org/10.4166/kjg.2018.71.2.103 pISSN 1598-9992 eISSN 2233-6869
IMAGE OF THE MONTH
Korean J Gastroenterol, Vol. 71 No. 2, February 2018 www.kjg.or.kr
위장관을 침범한 외투세포림프종
소설, 이정훈
울산대학교 의과대학 서울아산병원 소화기내과
Mantle Cell Lymphoma Involving Gastrointestinal Tract
Seol So and Jeong Hoon Lee
Division of Gastroenterology, Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
CC This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/4.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2018. Korean Society of Gastroenterology.
교신저자: 이정훈, 05505, 서울시 송파구 올림픽로 43길 88, 울산대학교 의과대학 서울아산병원 소화기내과
Correspondence to: Jeong Hoon Lee, Division of Gastroenterology, Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Songpa-gu, Seoul 05505, Korea. Tel: +82-2-3010-5678, Fax: +82-2-476-0824, E-mail: [email protected]
Financial support: None. Conflict of interest: None.
A B
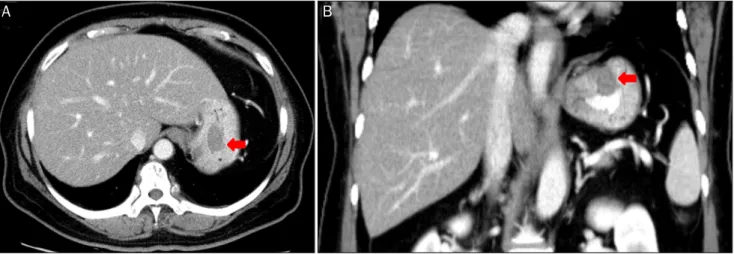
Fig. 1. Abdominal computed tomographic findings. (A, B) About 2.7 cm sized intraluminal polypoid mass at the gastric fundus (arrow).
증례: 59세 여자 환자가 복부 전산화단층촬영에서 발견된 위 강내 종괴로 내원하였다. 환자는 내원 5년 전 오른쪽 경부 림프 절 종대로 타원 조직생검에서 외투세포림프종(mantle cell lymphoma)으로 진단되었고, Ann Arbor 병기 IA로 확인되었 다. 본원에서 1차 항암 치료 후 부분 반응 소견을 보여 추가 방사 선 치료를 권유하였으나 추적 소실되었다. 내원 1년 전 양측 편 도 비대로 본원에 다시 내원하였고, 조직생검에서 재발된 외투 세포림프종, Ann Arbor 병기 IIIA로 확인되었다. 당시 상부위 장관 내시경은 경도의 위축성 위염 외에 이상 소견은 관찰되지
않았다. 2차 항암 치료 후 완전 관해로 확인되어 추적 관찰 중이 었다.
내원 당시 전신상태는 양호하였고, 활력징후는 정상이었다.
복부는 평탄하고 부드러웠으며 압통은 없었고, 간비종대 및 촉지되는 종괴는 없었다. 말초혈액 검사에서 백혈구 10,900/μL (참고치 4,000-10,000), 혈색소 13.1 g/dL (참고치 12.0-16.0), 혈소판 249,000/μL (참고치 150,000-350,000), 생화학 검사에 서 아스파르테이트아미노전달효소 44 IU/L (참고치 40 이하), 알라닌아미노전달효소 41 IU/L (참고치 40 이하), 젖산 탈수소효
104
소설, 이정훈. 위장관을 침범한 외투세포림프종The Korean Journal of Gastroenterology
A B
C D
Fig. 2. Esophagogastroduodenoscopic findings. (A) About 2.5 cm sized fusiform shaped hyperemic polypoid mass, at the gastric fundus. (B) Focal hyperemic erosion, at the gastric upper body, posterior wall side. (C) Increased size of gastric fundal mass after 1 year (D) Regression of previous mass and erosion after 3rd line chemotherapy.
소 188 IU/L (참고치 120-250)였다.
복부 전산화단층촬영에서 위저부에 약 2.7 cm 크기의 균 일한 조영을 보이는 종괴성 병변이 관찰되었으며(Fig. 1), 인 접한 위간인대를 따라서 커진 림프절들이 확인되었다. 경부 전산화단층촬영에서도 양측 level II 경부 림프절 종대가 새롭 게 확인되었다. 상부위장관 내시경에서 전정부와 체부에 경도 의 위축성 위염이 관찰되었고, 전반적인 발적을 동반한 점막 의 결절성 변화가 확인되었다. 또한 위저부에 2.5 cm 크기의 발적을 동반한 방추형의 용종성 병변이 관찰되었고(Fig. 2A), 상체부 후벽에서는 강한 발적을 동반한 국소적 미란이 확인되 었다(Fig. 2B).
위저부와 상체부 후벽 조직생검의 병리 소견에서 모두 재
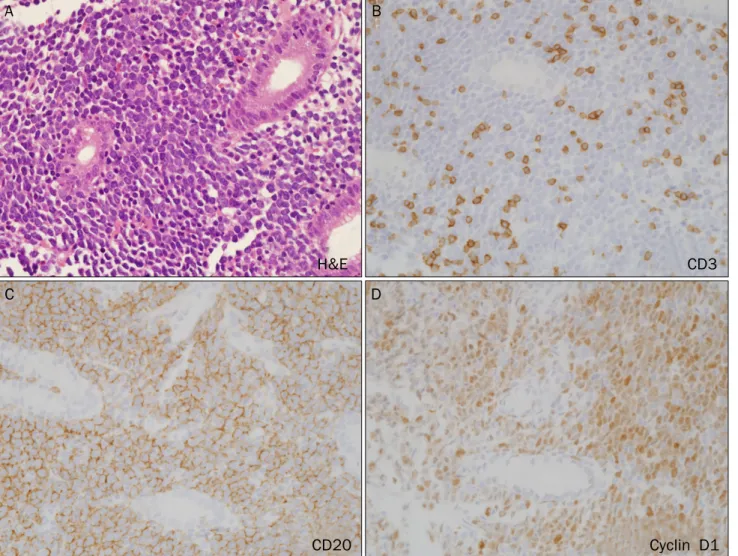
발한 외투세포림프종이 확인되었으며, 면역조직화학 검사에 서 CD20 양성, cyclin D1 양성, CD3 음성, CD5 음성이 확인 되었다(Fig. 3). 이를 바탕으로 환자는 위 침범을 동반하는 재 발된 외투세포림프종으로 확인되어 3차 항암 치료를 고려하 였으나 추적 소실되었다.
1년 후 상복부 통증과 구역, 구토로 재방문하여 시행한 상 부위장관 내시경에서 위저부 종괴는 현저한 크기 증가 소견을 보였으며(Fig. 2C), 양전자방출촬영에서도 전신 림프절 종대 소견이 확인되어 3차 항암 치료를 시행하였다. 1년 뒤 추적 내시경에서 위저부 및 상체부 후벽 병변 모두 호전되었고 (Fig. 2D), 조직생검에서 악성 세포는 관찰되지 않았다.
So S and Lee JH. Mantle Cell Lymphoma Involving Gastrointestinal Tract
105
Vol. 71 No. 2, February 2018
A B
C D
H&E CD3
CD20 Cyclin D1
Fig. 3. Gastric mucosal biopsy and immunohistochemistry from fundus and high body. Magnification ×400. (A) Tumor cells show diffuse infiltra- tion of gastric stroma. (B) Tumor cells are negative for CD3. (C, D) Tumor cells are diffusely and strongly positive for CD20 and Cyclin D1.
진단: 위의 외투세포림프종
외투세포림프종은 비교적 드문 악성 림프종으로, B세포형 림프종의 아형이며 비호지킨 림프종의 3-10%를 차지한다. 흔 히 처음 진단 시에 70% 정도에서 간비종대와 골수 및 말초혈 액 등의 전이 혹은 전신적인 림프절 종대가 있으며, 25%에서 Waldeyer’s ring, 위장관 등 여러 림프절외 병변을 보인다고 알려져 있다.1,2
외투세포림프종의 위장관 침범은 흔하여 15-30%의 환자에 서 나타나며, 흔히 위장관의 여러 부위에 다발성 용종의 형태 로 발현되어 림프종성 용종증(multiple lymphomatous poly- posis)이라는 진단명으로 불리기도 한다.3,4 위장관 침범과 연 관된 임상 증상은 복통, 구역, 구토, 설사, 혈변 등으로 다양하 게 나타난다고 알려져 있다.5위장관에 발생하는 경우 미만성 으로 침범하는 경향으로 수술적 치료는 어려운 경우가 많으 나,6일부에서는 공격적인 임상 양상을 보이지 않고 추가적인 치료를 하지 않아도 생존기간이 5-12년으로 긴 경우들도 보
고되었다.7,8
위장관 침범의 내시경 소견은 대개 무경성 혹은 유경성의 다발성 용종외에도 종양형, 결절형, 침윤형, 궤양형 등 다양한 병변으로 발현될 수 있으며, 점막의 미세한 변화만 발생하여 정상 점막과 구분되지 않고 조직생검으로만 진단된 경우들도 보고되고 있다.5,9 또한 다양한 형태의 병변이 동일한 환자의 소장 및 대장에서 동시에 관찰되기도 한다.10 특히 위의 원발 성 외투세포림프종은 몇몇의 경우에만 증례 보고가 될 정도로 드문 질환으로, 대개의 경우에도 전신 침범 또는 림프절 침범 과 동반되어 있다.11-13 Romaguera 등5의 연구에 따르면 58명 의 상부위장관 내시경을 받은 외투세포림프종 환자를 분석한 결과에서 22명(38%)은 정상 내시경 소견을 보였으며, 나머지 환자들은 결절, 염증, 용종, 궤양, 위벽의 비후, 종괴 등 다양 한 소견을 보였다. 이 중 가장 흔한 내시경적 이상 소견은 결 절(12명, 21%) 및 염증(11명, 19%)이었다. 이들 58명 중에서 28명(43%)이 조직학적으로 외투세포림프종로 확인되었고, 심
106
소설, 이정훈. 위장관을 침범한 외투세포림프종The Korean Journal of Gastroenterology
지어 22명의 정상 내시경 소견을 보인 환자 중에서도 10명 (45%)에서 림프종 침범이 확인되었다. 또한, 위장관 침범이 동반되더라도 대개의 경우 환자의 임상 경과에 유의한 영향을 미치지는 않았다.5
외투세포림프종의 진단은 병리조직 소견과 더불어 면역표현 형(immunophenotype) 검사가 필수적인데, CD5+, CD19+, CD20+, CD43+, CD10-, CD23-, sIg+와 같은 소견을 보이나 일부에서 CD5가 음성을 보일 수 있으며, 염색체 검사상 t(11;14)(q13;q32)가 진단에 도움을 주며,14 이는 cyclin D1의 과다발현을 통해 세포주기 조절을 억제하여 종양 발생에 기여한 다고 알려져 있다.15
외투세포림프종은 예후가 매우 나쁜 것으로 알려져 있으 며, 항암화학 요법에 관해율이 낮고, 완전 관해가 된다 하더라 도 관해 유지기간이 매우 짧아 2년 이내에 재발하는 것이 일 반적이며, 평균 생존 기간은 4-5년으로 알려져 있다. 따라서 최근에는 가능한 한 조기에 진단하여 위험도를 분류하고, 이 에 따른 고용량 항암 치료 또는 조혈모세포이식술을 시행하는 것을 권고하고 있다.16
REFERENCES
1. Argatoff LH, Connors JM, Klasa RJ, Horsman DE, Gascoyne RD.
Mantle cell lymphoma: a clinicopathologic study of 80 cases.
Blood 1997;89:2067-2078.
2. Norton AJ, Matthews J, Pappa V, et al. Mantle cell lymphoma: natu- ral history defined in a serially biopsied population over a 20-year period. Ann Oncol 1995;6:249-256.
3. Cornes JS. Multiple lymphomatous polyposis of the gastro- intestinal tract. Cancer 1961;14:249-257.
4. Meral M, Demirpençe M, Gönen C, et al. Diffuse gastrointestinal involvement of mantle cell lymphoma. Turk J Gastroenterol 2008;19:117-120.
5. Romaguera JE, Medeiros LJ, Hagemeister FB, et al. Frequency of gastrointestinal involvement and its clinical significance in man- tle cell lymphoma. Cancer 2003;97:586-591.
6. Chung HH, Kim YH, Kim JH, et al. Imaging findings of mantle cell lymphoma involving gastrointestinal tract. Yonsei Med J 2003;
44:49-57.
7. Nodit L, Bahler DW, Jacobs SA, Locker J, Swerdlow SH. Indolent mantle cell lymphoma with nodal involvement and mutated im- munoglobulin heavy chain genes. Hum Pathol 2003;34:1030- 1034.
8. Orchard J, Garand R, Davis Z, et al. A subset of t(11;14) lymphoma with mantle cell features displays mutated IgVH genes and in- cludes patients with good prognosis, nonnodal disease. Blood 2003;101:4975-4981.
9. Tamura S, Ohkawauchi K, Yokoyama Y, et al. Non-multiple lym- phomatous polyposis form of mantle cell lymphoma in the gastro- intestinal tract. J Gastroenterol 2004;39:995-1000.
10. Hotta K, Oyama T, Kitamura Y, Tomori A, Miyata Y, Mitsuishi T.
Mantle cell lymphoma presenting as multiple lymphomatous poly- posis spreading widely to the small intestine and diagnosed by dou- ble-balloon endoscopy. Endoscopy 2007;39 Suppl 1:E347-E348.
11. Kikuchi T, Asano N, Noguchi T, et al. A case of primary gastric man- tle cell lymphoma. Nihon Shokakibyo Gakkai Zasshi 2009;106:
1168-1176.
12. Pitigoi D, Stoica V, Stoia R, Dobrea C, Becheanu G, Diculescu M.
Gastric and colonic mantle cell lymphoma - incidental discovery.
J Gastrointestin Liver Dis 2009;18:85-88.
13. Kim CH, Chun HJ, Kim TH, et al. Solitary primary gastric mantle cell lymphoma. Gut Liver 2011;5:527-531.
14. Weisenburger DD, Armitage JO. Mantle cell lymphoma-- an entity comes of age. Blood 1996;87:4483-4494.
15. Garcia-Conde J, Cabanillas F. Mantle cell lymphoma: a lympho- proliferative disorder associated with aberrant function of the cell cycle. Leukemia 1996;10 Suppl 2:s78-s83.
16. Vose JM. Mantle cell lymphoma: 2017 update on diagnosis, risk-stratification, and clinical management. Am J Hematol 2017;
92:806-813.