이화여자대학교 의학전문대학원 내과학교실, 방사선과학교실, 병리학교실, 흉부외과학교실 심윤수1, 이진화1, 류연주1, 천은미1, 김유경2, 성순희3, 안재호4, 장중현1
A Case of Non-Specific Interstitial Pneumonia Associated with Primary Lung Adenocarcinoma
Yun Su Sim, M.D.1, Jin Hwa Lee, M.D.1, Yon Ju Ryu, M.D.1, Eun Mi Chun, M.D.1, Yoo Kyung Kim, M.D.2, Sun Hee Sung, M.D.3, Jae Ho Ahn, M.D.4, and Jung Hyun Chang, M.D.1
1Department of Internal Medicine, 2Radiology, 3Pathology, and 4Thoracic Surgery, Ewha Womans University School of Medicine, Seoul, Korea
Idiopathic pulmonary fibrosis (IPF) is strongly associated with lung cancer compared with the general population.
However, other types of idiopathic interstitial pneumonia (IIP) are rarely associated with lung cancer. We describe a case of a primary lung cancer associated with IIP other than IPF, which was considered to be nonspecific interstitial pneumonia (NSIP), and NSIP disappeared spontaneously after treating the primary lung cancer.
(Tuberc Respir Dis 2007; 63: 83-87)
Key Words: Interstitial lung diseases, Lung cancer, Adenocarcinoma.
Address for correspondence: Jin Hwa Lee, M.D.
Department of Internal Medicine, Ewha Womans University School of Medicine, 911-1 Mok-dong, Yancheon-gu, Seoul 158-710, Korea
Phone : +82-2-2650-6007, Fax : +82-2-2655-2076 E-mail : [email protected]
Received: May. 3. 2007 Accepted: Jun. 5. 2007
서 론
원발폐암과 특발성폐섬유화증(idiopathic pulmonary fibrosis, IPF)이 병발하는 경우는 비교적 흔하여, 폐 암의 발생률이 일반 인구보다 특발성폐섬유화증 환자 에서 더 높다고 알려져 있으나1-3, 비특이적간질성폐 렴(non-specific interstitial pneumonia, NSIP)이 원 발폐암과 병발한 경우는 매우 드물고, 그 발병기전이 폐암에 대한 인체 내 면역세포의 항체에 의한 면역반 응과 밀접한 관련이 있다는 보고가 있다4,5.
이에 저자 등은 우연히 발견된 원발폐암과 병발한 비특이적간질성폐렴 환자에서 원발폐암의 치료 후에 간질성폐렴이 자연 호전된 예를 경험하였기에 문헌 고찰과 함께 보고한다.
증 례 환 자: 49세, 여자
주 소: 단순흉부방사선촬영에서 발견된 폐결절 현병력: 특별한 증상이 없이 직장건강검진에서 시 행한 단순흉부방사선촬영에서 폐결절이 발견되어 본 원으로 의뢰되었다.
과거력: 특이사항 없음.
직업력: 8년 동안 고속도로통행료 징수원으로 근무함.
사회력: 흡연력 없음.
가족력: 특이사항 없음.
신체진찰 결과: 신체 활력 징후는 정상이었고, 목에 만져지는 종물은 없었으며, 심음과 호흡음은 정상이 었다.
검사실 결과: 말초혈액검사에서 혈색소는 13.2 g/dL, 백혈구는 4,700 /mm3이었고 호산구 비율은 2.1%로 정상 범위였다. 대기 중 동맥혈가스검사에서 PaCO2는 35.9 mmHg, PaO2는 112.0 mmHg, 산소포 화도는 98.3%였다. 류마티스 인자는 음성이었고, 형 광항핵항체는 약양성이었으며, 면역글로불린 중 IgG 는 1,640 mg/dL(참고치: 700-1,600 mg/dL)이었고, IgA와 IgM은 정상 범위였다. 종양표지물질 중 carcinoembryogenic antigen(CEA)과 neuron specific enolase(NSE)는 정상 범위였다.
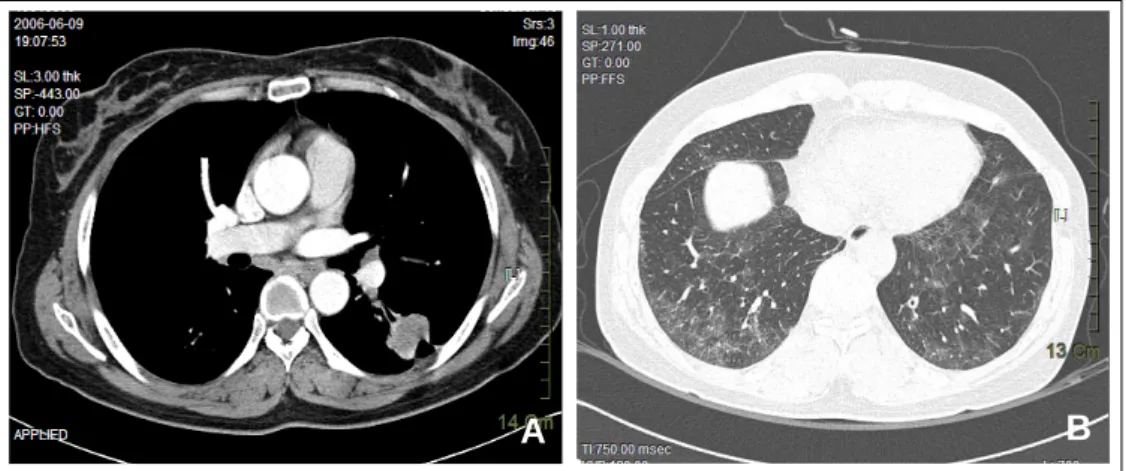
방사선촬영 결과: 단순흉부방사선촬영에서 좌하엽 에 종괴가 보였고(Figure 1), 흉부전산화단층촬영에 서 좌폐하엽에 장경이 3 cm인 종괴와(Figure 2A) 양
Figure 1. A 3-cm sized mass in the left lower lobe.
A B
Figure 2. (A) A 3-cm enhancing mass showing air bronchogram and speculated margin with pleural tag is noted in the superior segment of the left lower lobe. (B) Ill-defined ground-glass opacity is noted in both lower lobes, predominantly in peripheral and basal lungs.
리음영이 보였다(Figure 2B).
폐활량측정 결과: 노력성폐활량(FVC)이 2.92L로 정상예측치의 91%, 1초간 노력성호기량(FEV1)이 2.41 L로 98%, FEV1/FVC 83%, 폐확산능 80%로 정상이 었다.
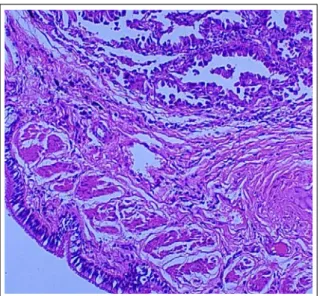
병리학적 소견: 수술 후 조직검사에서 중등도 이상 으로 분화된 입방형 세포들이 샘꽈리(aicini)를 이루 고 있었으며, 종괴의 중앙은 핵이 치우친 풍부한 호산 성 세포질을 가진 악성 세포들로 이루어져 있었고, 종
괴의 주변부는 기존의 폐포 구조 사이로 암세포들이 뻗어 있었다(Figure 3). 원발폐암의 크기는 3x3 cm로, 장측 흉막에 암세포침윤이 있었으며 림프절 전이는 없어서, 병리학적 폐암병기는 T2N0M0, IB이었다. 나 머지 좌폐하엽에서는 폐포벽으로 단핵구의 침윤을 동 반한 다발성이고 광범위하면서 성긴 간질성 섬유화가 있었고, 폐포벽은 균일하게 두꺼워져 있었으나, 폐실 질의 구조는 비교적 보존되어 있었다(Figure 4A). 다 발적으로 림프구의 침윤이 보였고 몇몇 다핵거대세포 와 콜레스테롤 틈새(cholesterol cleft)를 보이는 폐대 식세포들이 탈락되어 있었다(Figure 4B). 이상의 특 징은 병리학적으로 특발성간질성폐렴 중 비특이적간 질성폐렴에 가장 부합하였다.
치료 및 경과: 좌폐하엽 종괴에 대한 경피적세침생 검 결과 폐선암으로 진단한 후, FDG-PET 등 검사에 서 전이는 없다고 판단되어, 임상병기가 T1N0M0로, 좌폐하엽절제술을 시행하였으며, 수술 후 병리학적 병기는 T2N0M0, IB이었다.
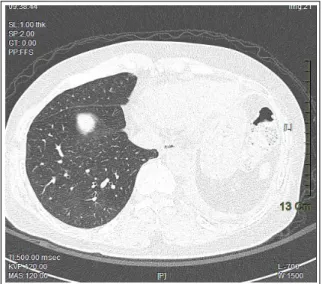
수술 4주 후에 시행한 흉부전산화단층촬영에서 수 술 전에 보였던 폐하엽의 간유리성 음영이(Figure 2B) 사라졌고(Figure 5), 수술 후 측정한 폐확산능도 정상예측치의 80%로 정상이었다. 환자는 Cisplatin과 paclitaxel로 보조항암요법을 4차례 받은 후, 현재 특 별한 증상 없이 외래에서 추적관찰 중이다.
Figure 3. The tumor lesion shows well-to-moderately differentiated neoplastic cells forming acini and tubules composed of cuboid cells, suggesting adenocarcinoma. (H&E stain, ×100)
A B
Figure 4. (A) Non-neoplastic lung parenchyma shows multifocal and diffuse loose interstitial fibrosis with mononuclear infiltration of alveolar walls. The alveolar wall is relatively uniformly thickened. However, the architecture of the lung parenchyma is relatively preserved. (B) Several multinucleated giant cells of undetermined significance, focal collection of desquamated alveolar macrophages with cholesterol clefts are noted. (H&E stain,
×100, A and B)
고 찰
비특이적간질성폐렴은 결체조직질환과 병발하는 경우가 많으며, 발생기전에서도 자가면역질환과 밀접 한 관련이 있는 것으로 알려져 있다6. 비특이적간질성 폐렴 환자 16명의 임상양상과 발생요인에 대해 살펴 본 한 연구에서는 15명이 흡연력이 있었으며, 5명이 비스테로이드성항염증약물을 장복하고 있었고, 9명이
화학약품을 다루거나 가구공장에서 일하고 있었던 것 으로 나타났다7. 본 증례의 환자는 비흡연자였으며, 고속도로통행료징수원으로 자동차 배기가스에 장시 간 노출되었을 가능성이 있으나, 배기가스가 비특이 적간질성폐렴의 발병에 미치는 영향에 대해서는 밝혀 진 바가 없다. 환자는 결체조직질환이나 자가면역과 관련된 혈청학적 검사 결과 이상이 없었고, 특이한 임 상증상이나 징후를 보이지 않았다.
폐암의 부종양증후군으로 경증의 피부질환이나 혈 액응고의 변화, 중증의 신경근육병증 등이 있을 수 있 으며, 간질성폐렴도 종종 동반되는 것으로 알려져 있 다8.
폐암이 특발성폐섬유화증에서 병발하는 경우는 부 검을 통한 연구에서는 48%까지 보고되었는데, 간질 성폐렴을 동반하지 않는 경우의 폐암과 비교하여 편 평상피세포암이 많고, 폐의 주변부에 있는 벌집 모양 병변에서 주로 발생하는 것으로 알려져 있다1-3. 특발 성폐섬유화증 환자의 경우 흡연자가 많기 때문에 흡 연이 폐암 발생에 기여하는 부분에 대한 확연한 구분 은 어렵지만, 만성적인 염증반응으로 인한 폐의 재형 성과정이 폐암을 발생시키는 것으로 생각하고 있다1,3. 반면에 본 증례와 같이 비특이적간질성폐렴과 폐암 이 병발한 예를 조사한 Yamadori 등4은 폐암세포의 항체로 알려져 있으면서 자가면역질환과 관계가 높은
Figure 5. There is left lower lobectomy state, and previous ground-glass opacity on figure 2B is not noted in the right lower lobe.
anti-cytokeratin 8과 anti-cytokeratin 19을 환자의 혈청과 폐암 조직에서 증명함으로써, 폐암에 대한 항 원-항체 반응의 결과로 면역복합체가 형성되어 폐상 피세포에 직접적인 손상을 가져오거나 국소적으로 대 식세포를 활성화시켜서 비특이적간질성폐렴이 발생 한 것이라고 설명하였다. 한편, Bandoh 등9이 폐암과 병발한 국소 림프구성간질성폐렴(lymphocytic inters- titial pneumonia)에 대해 보고한 증례에서도, 세포독 성T세포가 림프구성간질성폐렴 조직뿐 아니라 폐암 주위의 조직에 다수 침윤한 것을 관찰하여 원발폐암 에 대한 면역 반응이 국소 림프구성간질성폐렴을 일 으킨 것으로 추정하였다. 그 외 몇몇 연구에서도 폐암 과 암을 둘러싼 폐조직에서 면역세포의 침윤을 보고 하고 있으며, 대부분은 T세포와 자연살세포(NK cell) 를 포함한 림프구이다10-14. 한편, Watanabe 등15은 폐 선암에서는 림프구의 침윤이 많으며, 편평상피세포암 에서는 그 정도가 덜하고, 소세포폐암에서는 림프구 의 침윤이 거의 없다고 보고하였다.
본 증례에서 환자는 폐암 수술 전 흉부전산화단층 촬영에서 폐하엽의 주변부에 경계가 불분명한 미만성 간유리성 음영이 보였고, 수술 후 폐조직에서 비특이 적간질성폐렴으로 진단되었으나, 수술 4주 후에 간질 성폐렴에 대한 치료 없이 추적 촬영한 흉부전산화단
층촬영에서는 간유리성음영이 사라졌다. 본 증례에서 폐암과 암을 둘러싼 간질성폐렴 조직에서 폐암 항체 나 면역복합체를 증명한 것은 아니지만, 폐암을 제거 하면서 원발폐암에 대한 면역반응으로 발생하였을지 모르는 간질성폐렴이 치료 없이 자연 호전되었을 가 능성이 있다. 또는, 본 증례의 비특이적간질성폐렴이 폐암에 대한 면역반응으로 생긴 부종양증후군이었을 가능성도 있다. 다른 연구에서 면역학적 염색과 면역 점적방법을 통해 암세포에 대한 면역반응으로 인한 비특이적간질성폐렴의 발생 가능성을 제시한 보고는 있었으나4,5, 폐암 치료 후 비특이적간질성폐렴이 저절 로 호전되었다는 보고는 없었다.
이에 저자 등은 원발폐암과 병발한 비특이적간질성 폐렴 환자에서 원발폐암의 치료 후에 비특이적간질성 폐렴이 자연 호전된 예를 경험하여 보고한다.
요 약
원발폐암과 특발성폐섬유화증(idiopathic pulmonary fibrosis)이 병발하는 경우는 비교적 흔하여, 폐암의 발생률이 일반 인구보다 특발성폐섬유화증 환자에서 더 높다고 알려져 있으나, 비특이적간질성폐렴(non- specific interstitial pneumonia)이 원발폐암과 병발한 경우는 매우 드물다. 이에 저자 등은 최근에 우연히 발견된 원발폐암과 병발한 비특이적간질성폐렴 환자 에서 원발폐암의 치료 후에 비특이적간질성폐렴이 저 절로 호전된 예를 경험하였기에 보고하는 바이다.
참 고 문 헌
1. Matsushita H, Tanaka S, Saiki Y, Hara M, Nakata K, Tanimura S, et al. Lung cancer associated with usual interstitial pneumonia. Pathol Int 1995;45:925-32.
2. Park J, Kim DS, Shim TS, Lim CM, Koh Y, Lee SD, et al. Lung cancer in patients with idiopathic pulmonary fibrosis. Eur Respir J 2001;17:1216-9.
3. Daniels CE, Jett JR. Does interstitial lung disease predispose to lung cancer? Curr Opin Pulm Med 2005;11:431-7.
4. Yamadori I, Sato T, Fujita J, Dobashi N, Ohtsuki Y, Takahara J. A case of non-specific interstitial
pneumonia associated with primary lung cancer:
possible role of antibodies to lung cancer cells in the pathogenesis of non-specific interstitial pneumonia.
Respir Med 1999;93:754-6.
5. Sato T, Yamadori I, Fujita J, Hamada N, Yonei T, Bandoh S, et al. Three cases of non-specific interstitial pneumonia associated with primary lung cancer. Intern Med 2004;43:721-6.
6. Katzenstein AL, Fiorelli RF. Nonspecific interstitial pneumonia/fibrosis. Histologic features and clinical significance. Am J Surg Pathol 1994;18:136-47.
7. Reyes LJ, Morell F, Xaubet A, Ramirez J, Majo J.
Nonspecific interstitial pneumonia: epidemiologic and clinical characteristics. Med Clin 2006;126:47-52.
8. Patel AM, Davila DG, Peters SG. Paraneoplastic syndromes associated with lung cancer. Mayo Clin Proc 1993;68:278-87.
9. Bandoh S, Fujita J, Haba R, Tojo Y, Horiike A, Okamoto T, et al. Lung cancer with focal lymphocytic interstitial pneumonia. Intern Med 2002;41:997-1001.
10. Takanami I, Takeuchi K, Giga M. The prognostic value of natural killer cell infiltration in resected
pulmonary adenocarcinoma. J Thorac Cardiovasc Surg 2001;121:1058-63.
11. Lee TK, Horner RD, Silverman JF, Chen YH, Jenny C, Scarantino CW. Morphometric and morphologic evaluations in stage III non-small cell lung cancers.
Prognostic significance of quantitative assessment of infiltrating lymphoid cells. Cancer 1989;63:309-16.
12. Lipford EH 3rd, Eggleston JC, Lillemoe KD, Sears DL, Moore GW, Baker RR. Prognostic factors in surgically resected limited-stage, nonsmall cell carci- noma of the lung. Am J Surg Pathol 1984;8:357-65.
13. Brittenden J, Heys SD, Ross J, Eremin O. Natural killer cells and cancer. Cancer 1996;77:1226-43.
14. Johnson SK, Kerr KM, Chapman AD, Kennedy MM, King G, Cockburn JS, et al. Immune cell infiltrates and prognosis in primary carcinoma of the lung. Lung Cancer 2000;27:27-35.
15. Watanabe S, Sato Y, Kodama T, Shimosato Y.
Immunohistochemical study with monoclonal antibo- dies on immune response in human lung cancers.
Cancer Res 1983;43:5883-9.