Received: October 8 2018, Revised: October 12 2018, Accepted: October 12 2018
Corresponding author: Kyoung Hyo Choi, Department of Rehabilitation Medicine, Asan Medical Center, University of Ulsan College of Medicine, 88 Olympic-ro 43-gil, Seoul 05505, Korea
Tel: +82-2-3010-3800, Fax: +82-2-3010-6964 E-mail: [email protected]
Copyrights ⓒ The Korean Dysphagia Society, 2019.
Dysphagia in Patients with Tongue Cancer Treated with Surgery
Eun Jung Sung, M.D.1, Kyoung Hyo Choi, M.D., Ph.D.1, JaYoung Kim, M.D.1, Seoyon Yang, M.D., Ph.D.1, Jong-Lyel Roh, M.D.2, Seung-Ho Choi, M.D.2, Soon Yuhl Nam, M.D.2, Sang Yoon Kim, M.D.2
Departments of 1Rehabilitation Medicine and 2Otolaryngology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea
Objective: To evaluate the swallowing problems after a primary resection in patients with tongue cancer.
Methods: Thirty-eight patients with primary tongue cancer, who underwent a glossectomy and had undergone a Video Fluoroscopic Swallowing Study (VFSS) prior to surgery in a university hospital between January 2010 and May 2015, were included retrospectively. The clinical and swallowing features, including the VFSS parameters before and after surgery, were analyzed.
Results: Among the 38 patients, 33 patients were T1 and T2 stage. Thirty-one, six and one patient underwent a partial glossectomy, hemiglossectomy, and total glossectomy, respectively. More than ninety percent of the patients had a selective neck dissection. All the patients were on a regular diet before surgery and showed no penetration or aspiration on the VFSS. Immediately after surgery, 33 patients (87%) had to change to non-oral feeding. At dis- charge, 8 patients (21%) maintained non-oral feeding, and 30 patients ate a limited diet. In a telephone survey (mean 19 months after surgery), among the 25 survey participants, 24 patients (96%) reported no problems with their regular diet.
Conclusion: In tongue cancer patients with low Tumor-Node-Metastasis (TNM), American Joint Committee on Cancer (AJCC) stages, a primary resection of tongue cancer did not cause statistically significant dysphagia after surgery.
Although many patients had to change their diet to limited or non-oral feeding immediately after surgery, almost all patients improved and could eat a regular diet after the long term follow up. (JKDS 2019;9:1-9)
Keywords: Deglutition disorders, Head and neck neoplasms, Deglutition, Tongue neoplasms
INTRODUCTION
For patients undergoing treatment for head and neck cancer, the impact of malnutrition on outcomes can be severe. Studies have demonstrated that under-
nutrition in patients with head and neck cancer is associated with poor treatment outcomes, including morbidity, infections, cancer recurrence, mortality, and poor quality of life (QOL)1,2. For many head and neck cancer patients, the anatomic location of the
tumor restricts swallowing and leads to reduced caloric intake. Not only anatomic location, but also treatment related dysphagia and odynophagia are some of the most serious and persistent complications3-5.
There were numerous studies on dysphagia in patients with head and neck cancer6-11. But these studies had several limitations. First, majority of the studies involved patients with head and neck cancer regardless of precise anatomical location. There are several types of head and neck cancer including cancer of oral cavity, lip, oropharynx, hypopharynx, nasopharynx, glottis larynx, supraglottic larynx, maxil- lary sinus, and ethmoid sinus12. Even when we say oral cavity cancer, it involves cancer of buccal mucosa, floor of mouth, anterior tongue, alveolar ridge, retromolar trigone, and hard palate. Dysphagia after surgery for nasopharynx would be very different from dysphagia after surgery for anterior tongue. In other words, previous studies on dysphagia in head and neck cancer patients had too generalized inclusion criteria, so it would be very difficult to dissociate true effect of primary resection for the cancer of anterior tongue from other oral cavity cancer.
Second, previous studies mostly concerned about dysphagia after organ preserving therapy (i.e.
radiation therapy (RT) or concurrent chemoradiotherapy) or at least, involved treatment group other than primary resection. Since 1980s, non-surgical treatment (RT or chemoradiotherapy) has been preferred to surgery because of its ability to spare the anatomy while ensuring a compare rate of loco-regional con- trol13,14. However, in turn, surgical techniques have improved markedly since the advent of reconstruction techniques using free micro-anastomosed flaps15. In National Comprehensive Cancer Network (NCCN) guidelines version 2.201312, most panel members prefer surgical therapy for resectable oral cavity tumors, and organ preservation using chemotherapy has received less attention for the initial management of patients with oral cavity cancers. The treatment protocols have different impacts on tissue which is important for optimal swallowing function11,16. And functional deficits encountered are related to the
specific anatomic or neurologic insult produced by the resection16.
To date, many other studies have investigated the swallowing dysfunction after treatment of head and neck cancer, but most of them included heterogenous groups in regards of anatomic site of tumor and treatment modalities, including radiation therapy. In Korea, during 1999-2010, oral cavity cancer occurred in 10,282 patients and the most common cancer site was the tongue (5,163 cases, 50.2%)17. From 1993 to 2010, overall cases of oral cavity cancer increased, including tongue cancer. During 1993-1995, total cases of tongue cancer was 617, but during 2006- 2010, total cases increased to 4,558. In spite of increasing cases of tongue cancer, the study that investigated dysphagia after primary resection for tongue cancer has been nearly nonexistent. In this study, we aimed to evaluate swallowing problems after primary resection in patients with tongue cancer.
MATERIALS AND METHODS 1. Subjects
The charts of 126 patients who newly diagnosed with tongue cancer and admitted at the Departement of Otolaryngology in a university hospital between January 2010 and May 2015 were reviewed retrospec- tively. Inclusion criteria included the followings: (1) patients with squamous cell carcinoma of tongue; (2) patients who treated with primary resection of cancer;
(3) patients who had VFSS preoperatively. Exclusion criteria included the followings: (1) patients with distant metastasis; (2) patients who had other cause of dysphagia before surgery; (3) patients with base of tongue cancer; (4) patients who treated with other modality except surgery (e.g. adjuvant chemo- radiotherapy or radiotherapy). Of one hundred and twenty-six patients, sixty-three patients who were treated with other modality except surgery and twenty patients who did not have baseline VFSS before surgery were excluded. A telephone survey was done to know diet of at long term after surgery. The five patients were excluded because they refused to
participate study. The remaining thirty-eight patients were included in this study. This study was approved by Institutional Review Board (IRB No. 2014-0675).
2. Variables
Demographic and clinical data were extracted from the electronic medical record. Data points included demographic characteristics, tumor staging according to tumor-lymph node-metastasis (TNM) classification, American Joint Committee on Cancer (AJCC 7th) stage, and surgical record. The surgical record included neck dissection (number of lymph node, type), nerve injury, reconstruction (type of flap), and size of resection. Records on the diet at admission, immediate after surgery, and at discharge were also reviewed.
The diet was categorized into non-oral, limited, or regular diet. To investigate the current status of the diet after the surgery, we did a telephone survey.
3. VFSS
A modified version of the protocol from the study of Logemann was used18. Initially, 3 mL of thick liquid was provided to the patients. And then, swallowing tests involving 3 mL of pureed, semi-solid, solid, and thin liquids were performed in this sequence and each test was performed three times. Swallowing images in the anteroposterior and lateral projection were acquired while the patients were seated. Two physiatrists with expertise in rehabilitation medicine analyzed the following findings: decrease in tongue control; the presence of vallecular pouch, or pyriform sinus residue; videofluoroscopic dysphagia Scale (VDS)19, penetration-aspiration scale (PAS)20, and American speech-language-hearing association national outcome measurement system (ASHA-NOMS) swal- lowing scale21. The VDS is a scale that was developed to quantify dysphagia severity and PAS evaluates airway invasion. The ASHA NOMS swallowing scale is a multi-dimensional tool designed to measure both the diet level and the supervision level required by assigning a single number between 1 and 7. A higher ASHA NOMS score indicates a better swallowing function, whereas higher VDS and PAS scores indicate
a poorer swallowing function.
4. Statistical analysis
Data was analyzed using the Statistical Package for Social Sciences software package (SPSS ver. 20.0;
SPSS, Inc., IL). A Chi-square test, McNemar test, Wilcoxon-signed rank test were used to compare the swallowing function before and after surgery. The univariate and multivariate analysis was used to know factor which associated with non-oral feeding at discharge. Significance was accepted for P<0.05.
RESULTS
This study included 24 men and 14 women, and the mean patient age was 54 years (range, 49.1-59.1 years).(Table 1) Of these patients, 23 (60.5%) had T1 tumor, 10 (26.3%) had T2 tumor, and 5 (13.2%) had advanced T4 tumor; 36 (94.7%) had N0 tumor; and 32 (84.2%) had overall AJCC stage I and II disease.
Thirty-four patients (97.4%) had lymph node dissection.
Of these patients, mean number of dissected lymph node were 32.0 (range, 28.5-35.4). Thirty-four patients (91.9%) had selective neck dissection and 3 patients (8.1%) had modified radical neck dissection. Thirteen patients (34.2%) had reconstruction after glossectomy.
Of these 13 patients, 6 patients (46.2%) had local flap, 3 patients (23.1%) had radial free flap (RFFF), and 2 patients (15.4%) anterolateral thigh flap operation (ALTF). Thirty-one patients (81.6%) patients had partial glossectomy which resected less than 50 percent of tongue, 6 patients (15.8%) had hemiglossectomy, and 1 patient (2.6%) had total glossectomy.
1. Diet type
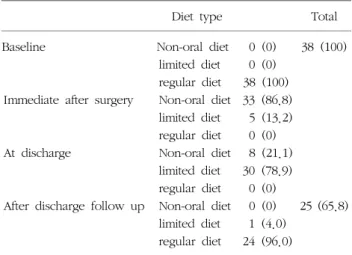
Before surgery, all thirty-eight patients had no problem in eating regular diet.(Table 2) Immediate after surgery, 33 patients (86.8%) changed to non-oral feeding, and five patients (13.2%) changed to limited diet. When patients came to discharge, eight patients (21.1%) had to discharge with non-oral feeding, whereas most patients (n=30, 78.9%) maintained limited diet.
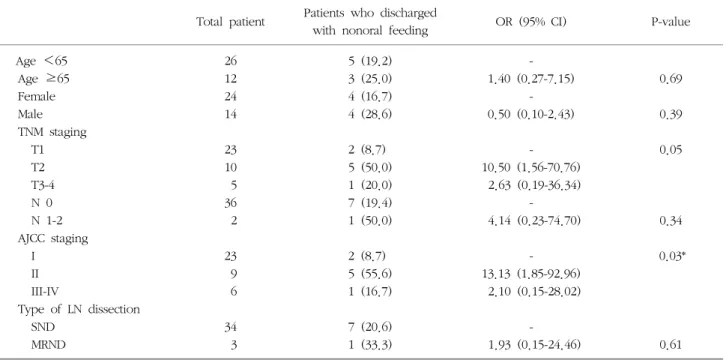
After multivariate analysis, AJCC staging was associated
Table 1. Baseline characteristics.
Variables Total Patients with post operation VFSS
Number of patients (n) 38 8
Age (yr) 54.2 (49.1-59.1) 58.5 (50.8-66.4) Gender (M:F) 24:14 (63.2:36.8) 3:5 (37.5:62.5) Tumor classification
T1 23 (60.5) 4 (50.0)
T2 10 (26.3) 4 (50.0)
T3 0 (0) 0 (0)
T4 5 (13.2) 0 (0)
Lymph node classification
N0 36 (94.7) 8 (100.0)
N1 1 (2.6) 0 (0)
N2 1 (2.6) 0 (0)
AJCC stage
I 23 (60.5) 4 (50.0)
II 9 (23.7) 4 (50.0)
III 1 (2.6) 0 (0)
IV 5 (13.2) 0 (0)
Patients with lymph node dissection
37 (97.4) 8 (100.0) Number of dissected
lymph nodes
32.0 (28.5-35.4) 29.8 (23.8-35.3) Type of lymph node
dissection
MRND:SND 3:34 (8.1:91.9) 0:8 (0:100.0)
Nerve injury 7 (18.4) 2 (25.0)
Reconstruction 13 (34.2) 4 (50.0)
RFFF 3 (23.1) 1 (25.0)
ALTF 2 (15.4) 0 (0)
Local flap 6 (46.2) 3 (75.0)
Other free flap 2 (15.4) 0 (0) Operation
Glossectomy (≤50%) 37 (97.4) 8 (100.0) Glossectomy (>50%) 1 (2.6) 0 (0)
Values are presented as the number of patient (%) or mean (95% confidence interval).
AJCC: American Joint Committee on Cancer, MRND: modified radical neck dissection, SND: selective neck dissection, RFFF:
radial free flap, ALTF: anterolateral thigh flap.
Table 2. Comparison of diet type in tongue cancer patients before surgery, immediate after surgery, at discharge, and after discharge follow up period.
Diet type Total
Baseline Non-oral diet 0 (0) 38 (100)
limited diet 0 (0) regular diet 38 (100) Immediate after surgery Non-oral diet 33 (86.8)
limited diet 5 (13.2) regular diet 0 (0) At discharge Non-oral diet 8 (21.1)
limited diet 30 (78.9) regular diet 0 (0)
After discharge follow up Non-oral diet 0 (0) 25 (65.8) limited diet 1 (4.0)
regular diet 24 (96.0) Values are presented as the number of patient (%).
with high risk of non-oral feeding at discharge (P=
0.03).(Table 3) In a telephone survey after surgery (mean 19.3 month), 25 patients responded to question.
Among patients who answered, 24 patients (96.0%) were having regular diet whereas only one patient were having a limited diet.
2. VFSS findings
The VFSS was performed on 38 patients before surgery and on 8 patients after surgery.(Table 4) Of the 8 patients who had VFSS postoperatively, patients did not have problem in tongue function, and there was no residue at vallecular pouch and piriform sinus before surgery. There was no airway penetration or aspiration of contrast material (PAS=1), and initial mean VDS was 0. After glossectomy, four patients (50.0%) showed impaired tongue function, and two patients (25.0%) showed contrast material in vallecular pouch. The mean VDS increased 0 to 4.88, but tongue function and VDS parameters failed to prove statistical significance (P=0.38, P=0.26, respectively).
After surgery, ASHA-NOMS score aggravated from 6-7 (i.e. normal diet) to level 1-2 level (nonoral nutrition necessary group) in one patient (12.5%).
DISCUSSION
In present study, we evaluated tongue cancer patients who were only treated with primary resection.
The results showed that aspiration, penetration did not increase after surgery in patients with low TNM, AJCC stage who treated with resection of tongue below 50% and neck dissection. Frequency of impair-
Table 3. Derivation set of patients with tongue cancer treated with surgery in relation to non-oral feeding at discharge.
Total patient Patients who discharged
with nonoral feeding OR (95% CI) P-value
Age <65 26 5 (19.2) -
Age ≥65 12 3 (25.0) 1.40 (0.27-7.15) 0.69
Female 24 4 (16.7) -
Male 14 4 (28.6) 0.50 (0.10-2.43) 0.39
TNM staging
T1 23 2 (8.7) - 0.05
T2 10 5 (50.0) 10.50 (1.56-70.76)
T3-4 5 1 (20.0) 2.63 (0.19-36.34)
N 0 36 7 (19.4) -
N 1-2 2 1 (50.0) 4.14 (0.23-74.70) 0.34
AJCC staging
I 23 2 (8.7) - 0.03*
II 9 5 (55.6) 13.13 (1.85-92.96)
III-IV 6 1 (16.7) 2.10 (0.15-28.02)
Type of LN dissection
SND 34 7 (20.6) -
MRND 3 1 (33.3) 1.93 (0.15-24.46) 0.61
Values are presented as the number of patient (%) or mean value (95% confidence interval).
TNM: Tumor Node Metastasis, AJCC: American Joint Committee on Cancer, LN: lymph node, SND: selective neck dissection, MRND:
modified radical neck dissection.
*P-value <0.05 by multivariate logistic regression analysis.
Table 4. Comparison of video fluoroscopic swallowing study findings before and after surgery in tongue cancer patients.
Baseline After
P n=8
Duration after op (mo) 4.34 (2.03-7.39)
Impaired tongue function 0 (0) 4 (50.0) 0.38 Vallecular residue 0 (0) 2 (25.0)
Piriform sinus residue 0 (0) 0 (0)
VDS 0 4.9 (0.60-10.88) 0.26
PAS
1 8 (100.0) 8 (100.0)
ASHA-NOMS
1-2 0 (0) 1 (12.5)
3-5 0 (0) 0 (0)
6-7 8 (100.0) 7 (87.5)
Values are presented as the number of patient (%) or mean value (95% confidence interval).
VDS: videofluoroscopic dysphagia scale, PAS: penetration aspiration scale, ASHA-NOMS: American speech-language-hearing association national outcome measurement system.
McNemar test for tongue function, residue of vallecular and piriform sinus comparison.
Wilcoxon-signed rank test for VDS comparison.
ment of tongue function, residue of vallecular sinus, VDS showed tendency to increase after surgery but these results were not statistically significant. Immedi- ately after surgery, patients had to change diet to nonoral or limited diet. When they came to discharge, many patients improved from immediate post operation state, but 20-30% of patients had to discharge with nonoral feeding. Nonetheless, after long term follow up, almost all of patients improved to eat regular diet except one patient who maintained limited diet.
Only few studies reported on the swallowing outcome after only primary resection of tongue cancer. Son et al.22 reported that abnormal tongue control, chewing abnormality, delay in oral transit time, aspiration or penetration, residue in vallecular, pyriform sinus residue, and inadequate laryngeal elevation developed after tongue cancer surgery. The male gender, extensive tumor resection, a higher nodal stage, and more ex- tensive lymph node dissection were major risk factor for aspiration in tongue cancer patients. However, this study had limitations of lack of time past surgery and
heterogenous treatment modalities among patients.
Lindsay et al.23 reported that in 15 patients who had 50-75% resection of tongue and radial free flap recon- struction, swallowing of liquid was significantly worse at postoperative 1 month due to premature spillage and laryngeal penetration and a higher number of swallowing attempts is required to clear bolus, but all VFSS parameters returned to preoperative level after 12 months.
Previously Hirano et al.24 had studied that two patients who had hemiglossectomy without recon- struction could eat normal food without aspiration within a week after operation, and eight patients who had undergone two-to three-quarter glossectomy for tongue cancer ate gruel with no or occasional liquid aspiration. Similar to our results, Hsiao et al.25 found that small number of patients who underwent hemi- glossectomy for anterior two thirds of the lateral tongue cancer and suffered decreased bolus volume and ingestion rate compared to the normal subject right after their operation, after 6 months, the majority (75.5%) of them managed to have unrestricted diet.
Uwiera et al.26 reported no significant differences in any of oral preparatory or oral phase swallowing parameters across any of the evaluation times in 11 patients treated for tongue cancer with hemiglos- sectomy and reconstruction with a bilobed RFFF. In accordance with these studies, we found that 96% of our 25 patients with low stages of TNM, AJCC stages, and had below 50% resection of tongue, had no problem in regular diet at mean 19 months after operation.
Previous studies on dysphagia of patients with tongue cancer did not distinguish treatment modalities, so results interpretation could be confusing to know pure effect of primary resection on dysphagia devel- opment.
The principal finding of this study was that patients who could treated with primary resection below 50%
resection of tongue had low risk of penetration or aspiration after operation, but risk of oral phase of dysphagia could be considered. Even all of patients failed to eat regular diet at discharge, but almost patients
improved so nearly all of them could eat regular diet after long term follow up. It is reported that in many other studies, swallow problems reported at frequencies of greater than fifty percent for patients treated with chemoradiotherapy to various sites in the head and neck27-34. These results suggest that primary resection below 50% of tongue may have a good prognosis in swallowing function than organ preservating therapy (e.g. radiotherapy).
Our explanation for the results could be that previous studies had heterogenous group of treatment, so other treatment (especially radiotherapy) might affect the dysphagia after surgery. Previous studies found that swallowing disorders in patients treated with chemoradiotherapy to head and neck cancer include reduced anterior-posterior tongue movement, reduced tongue strength, reduced tongue base retraction, increased oral residue, increased velopha- ryngeal closure duration, reduced epiglottic inversion, slowed or reduced laryngeal elevation, impaired pha- ryngeal constrictor motility, increased pharyngeal residue, delayed pharyngeal swallow, and delayed laryngeal vestibule closure27-34.
Post-radiotherapy swallowing disorders are due to primarily neuromuscular fibrosis and radiation-induced edema35,36. RT induces hyperactivation through hydroxyl radicals of transforming growth factor-β1 (TGF-β1) leads to fibrosis and the resulting abnormal motility of deglutition muscles as impaired pharyngeal contraction and laryngeal elevation responsible for dysphagia, aspiration, and stenosis37. Second, sensory changes in the oral cavity and the pharynx also play a role in post-RT swallowing disorders by changing the patients’ perception of swallowing37,38. There are hypotheses that chemoradiotherapy can have an adverse effect on innervation of the larynx and pharynx, causing loss of laryngeal sensation, motor function, and normal peristalsis39. Third, xerostomia after RT contributes to swallowing problems, associated with difficulties in mastication and delayed initiation of the swallowing reflex because of decreased bolus lubri- cation due to the lack of saliva38.
In present study, we excluded who treated with
radiotherapy and/or chemoradiotherapy, so we could interpret more specified results after surgery. Patients treated with primary resection could be free of RT induced fibrosis and edema, reducing risk of impaired pharyngeal, laryngeal contractility and motility. Most of the time, neck dissection is a process of primary resection. It is unclear that whether neck dissection is superior in preserving innervation of larynx and pharynx than RT, but if nerve is preserved while surgery process, sensory changes after neck dissection expected to be lower than after RT. Also, it is obvious that primary resection is much more superior than preventing treatment induced xerostomia than RT.
Present results that lesser degree of dysphagia than other previous studies and especially free of dysphagia of pharyngeal phase suggests that primary resection itself did not cause serious dysphagia after surgery.
Other explanation was that unlike previous studies, present study included patients with low TNM, AJCC stage, and all of patients treated with less than 50%
of glossectomy and nearly all of patients treated with selective lymph node dissection. Other previous studies included high grade of tumor and nodal stages, so resection boundaries might have to be larger than present study, resulting possible additional damage of pharyngeal structures other than limited resection of tongue and selective node dissection.
The VFSS finding of present study suggested that possible dysphagia of oral phase. Although statistical evaluation failed to prove the aggravated features, patients with impaired tongue function increased zero patient to four patients and two patients showed residue in vallecular pouch after surgery. Unlike PAS and ASHA-NOMS which mainly concerned about penetration or aspiration, VDS directly or indirectly reflects oral phase of dysphagia in question of bolus formation, mastication, apraxia, tongue to palate contact, premature bolus loss, oral transit time, and vallecular residue. In present study, VDS increased 0 to 4.9 after surgery. All of patients did not show aspir- ation or penetration, and only one patient scored ASHA-NOMS score 2 (nonoral feeding) because of
patient showed severe oral stage bolus retention and unable to clear. According to VFSS results, patients showed possibilities of oral phase dysphagia, but parameters of pharyngeal dysphagia showed no definite abnormalities.
In multivariate analysis, AJCC stage was associated with high risk of nonoral feeding at discharge. But we had to cautious about interpreting this result, because patients with AJCC stage II showed higher risk of nonoral feeding than patients with AJCC stage III or IV. It might from small number of patients. Statistical analysis with the more patients might show different result.
Our study had several limitations. First, the number of patients was small, even if it was comparable to that of most other studies on dysphagia of patients with tongue cancer; however, subtle differences before and after surgery might require larger studies to be detected. Second, there was a lack of long term follow up evaluation of VFSS. Although it seems that almost all patients could eat regular diet after long term follow up, it was not proven with VFSS. So we still do not know objective chronic features of dysphagia after primary resection of tongue.
CONCLUSION
In tongue cancer patients with low TNM, AJCC stages, below 50% primary resection of tongue cancer did not cause statistically significant dysphagia after surgery. Even many patients had to eat limited or nonoral feeding immediate after surgery, nearly all the patients improved and could eat regular diet after long term follow up. But we still could not rule out the possibilities of aggravation of oral phase dysphagia. Hence, future systemic research with large sample size is required to clarify the long-term result of primary resection of tongue cancer.
REFERENCES
1. van Bokhorst-de van der, S., et al., The impact of nutri- tional status on the prognoses of patients with advanced
head and neck cancer. Cancer, 1999;86(3):519-27.
2. Brookes, G.B. and P. Clifford, Nutritional status and general immune competence in patients with head and neck cancer. J R Soc Med, 1981;74(2):132-9.
3. Hillman, R.E., et al., Functional outcomes following treatment for advanced laryngeal cancer. Part I--Voice preservation in advanced laryngeal cancer. Part II-- Laryngectomy rehabilitation: the state of the art in the VA System. Research Speech-Language Pathologists.
Department of Veterans Affairs Laryngeal Cancer Study Group. Ann Otol Rhinol Laryngol Suppl, 1998;172:1-27.
4. Pauloski, B.R., et al., Biomechanical analysis of the pharyngeal swallow in postsurgical patients with anterior tongue and floor of mouth resection and distal flap reconstruction. J Speech Hear Res, 1995;38(1):110-23.
5. Henk, J.M., Controlled trials of synchronous chemo- therapy with radiotherapy in head and neck cancer:
overview of radiation morbidity. Clin Oncol (R Coll Radiol), 1997;9(5):308-12.
6. Pauloski, B.R., et al., Comparison of swallowing func- tion after intensity-modulated radiation therapy and con- ventional radiotherapy for head and neck cancer. Head Neck, 2015;37(11):1575-82.
7. Starmer, H.M., et al., Swallowing outcomes in patients with oropharyngeal cancer undergoing organ-preserva- tion treatment. Head Neck, 2014;36(10):1392-7.
8. Lam, L. and N. Samman, Speech and swallowing fol- lowing tongue cancer surgery and free flap re- construction--a systematic review. Oral Oncol, 2013;
49(6):507-24.
9. Dziegielewski, P.T., et al., Total glossectomy with lar- yngeal preservation and free flap reconstruction: ob- jective functional outcomes and systematic review of the literature. Laryngoscope, 2013;123(1):140-5.
10. Wall, L.R., et al., Physiological changes to the swallow- ing mechanism following (chemo)radiotherapy for head and neck cancer: a systematic review. Dysphagia, 2013;
28(4):481-493.
11. Platteaux, N., et al., Dysphagia in head and neck cancer patients treated with chemoradiotherapy. Dysphagia, 2010;25(2):139-52.
12. National Comprehensive Cancer Network. Head Neck Cancers. Version 2. 2013.
13. Calais, G., et al., Randomized trial of radiation therapy versus concomitant chemotherapy and radiation therapy for advanced-stage oropharynx carcinoma. J Natl Cancer Inst, 1999;91(24):2081-6.
14. Nguyen, N.P., et al., Analysis of factors influencing aspi- ration risk following chemoradiation for oropharyngeal cancer. Br J Radiol, 2009;82(980):675-80.
15. Markkanen-Leppanen, M., et al., Swallowing after free- flap reconstruction in patients with oral and pharyngeal cancer. Oral Oncol, 2006;42(5):501-9.
16. Kronenberger, M.B. and A.D. Meyers, Dysphagia fol- lowing head and neck cancer surgery. Dysphagia, 1994;
9(4):236-44.
17. Choi, S.W., et al., Trends in the incidence of and sur- vival rates for oral cavity cancer in the Korean population.
Oral Dis, 2014;20(8):773-9.
18. A., L.J., Manual for the videofluorographic study of swallowing. 2nd ed: Pro-Ed; 1993.
19. Han, T.R., N.J. Paik, and J.W. Park, Quantifying swal- lowing function after stroke: A functional dysphagia scale based on videofluoroscopic studies. Arch Phys Med Rehabil, 2001;82(5):677-82.
20. Pietila, S., et al., Neurological outcome of childhood brain tumor survivors. J Neurooncol, 2012;108(1):153-61.
21. O'Neil, K.H., et al., The Dysphagia Outcome and Severity Scale. Dysphagia, 1999;14(3):139-45.
22. Son, Y.R., K.H. Choi, and T.G. Kim, Dysphagia in tongue cancer patients. Ann Rehabil Med, 2015;39(2):
210-7.
23. Brown, L., et al., A longitudinal study of functional out- comes after surgical resection and microvascular re- construction for oral cancer: tongue mobility and swal- lowing function. J Oral Maxillofac Surg, 2010;68(11):
2690-700.
24. Hirano, M., et al., Dysphagia following various degrees of surgical resection for oral cancer. Ann Otol Rhinol Laryngol, 1992;101(2 Pt 1):138-41.
25. Hsiao, H.T., Y.S. Leu, and C.C. Lin, Primary closure versus radial forearm flap reconstruction after hemi- glossectomy: functional assessment of swallowing and speech. Ann Plast Surg, 2002;49(6):612-6.
26. Uwiera, T., et al., Functional outcomes after hemi- glossectomy and reconstruction with a bilobed radial forearm free flap. J Otolaryngol, 2004;33(6):356-9.
27. Eisbruch, A., et al., Objective assessment of swallowing dysfunction and aspiration after radiation concurrent with chemotherapy for head-and-neck cancer. Int J Radiat Oncol Biol Phys, 2002;53(1):23-8.
28. Graner, D.E., et al., Swallow function in patients before and after intra-arterial chemoradiation. Laryngoscope, 2003;113(3):573-9.
29. Kotz, T., et al., Pharyngeal transport dysfunction con- sequent to an organ-sparing protocol. Arch Otolaryngol Head Neck Surg, 1999;125(4):410-3.
30. Lazarus, C.L., et al., Swallowing disorders in head and neck cancer patients treated with radiotherapy and ad- juvant chemotherapy. Laryngoscope, 1996;106(9 Pt 1):
1157-66.
31. Kotz, T., et al., Swallowing dysfunction after chemo- radiation for advanced squamous cell carcinoma of the head and neck. Head Neck, 2004;26(4):365-72.
32. Logemann, J.A., et al., Site of disease and treatment protocol as correlates of swallowing function in patients with head and neck cancer treated with chemoradiation.
Head Neck, 2006;28(1):64-73.
33. Logemann, J.A., et al., Swallowing disorders in the first year after radiation and chemoradiation. Head Neck,
2008;30(2):148-58.
34. Sullivan, C.A., et al., Endoscopic management of hypo- pharyngeal stenosis after organ sparing therapy for head and neck cancer. Laryngoscope, 2004;114(11):1924-31.
35. Teguh, D.N., et al., Treatment techniques and site con- siderations regarding dysphagia-related quality of life in cancer of the oropharynx and nasopharynx. Int J Radiat Oncol Biol Phys, 2008;72(4):1119-27.
36. Smith, R.V., et al., Long-term swallowing problems after organ preservation therapy with concomitant radiation therapy and intravenous hydroxyurea: initial results.
Arch Otolaryngol Head Neck Surg, 2000;126(3):384-9.
37. Logemann, J.A., et al., Xerostomia: 12-month changes in
saliva production and its relationship to perception and performance of swallow function, oral intake, and diet after chemoradiation. Head Neck, 2003;25(6):432-7.
38. Mittal, B.B., et al., Swallowing dysfunction--preventative and rehabilitation strategies in patients with head-and- neck cancers treated with surgery, radiotherapy, and chemotherapy: a critical review. Int J Radiat Oncol Biol Phys, 2003;57(5):1219-30.
39. Rosenthal, D.I., J.S. Lewin, and A. Eisbruch, Prevention and treatment of dysphagia and aspiration after chemo- radiation for head and neck cancer. J Clin Oncol, 2006;
24(17):2636-43.