82 접수일: 2010년 3월 25일, 게재결정: 2010년 6월 29일
*교신저자: 조장현, 540-719, 성가롤로병원 순환기내과, Phone: 061-720-2123, FAX: 061-720-2068, E-mail: [email protected] Vol. 46, No. 2, pp. 82∼87
DOI: 10.4068/cmj.2010.46.2.82
고령 환자에서 좌우측 요골동맥을 이용한 관상동맥조영술 및 중재술의 비교
성가롤로병원 순환기내과, 1전남대학교병원 순환기내과
이민근ㆍ조장현*ㆍ황영준ㆍ김우종ㆍ윤재성ㆍ김준영ㆍ김수현ㆍ정명호1
Comparison between the Left and Right Transradial Coronary Angiograms and Interventions in Elderly Patients
Min Geun Lee, Jang Hyun Cho*, Young Jun Hwang, Woo Jong Kim, Jae Sung Yoon, Jun Young Kim, Su Hyun Kim and Myung Ho Jeong1
Division of Cardiology, Department of Internal Medicine, St. Carollo Hospital, Sunchun,
1The Heart Center of Chonnam National University Hospital, Gwangju, Korea
The transradial approach for coronary angiography (CAG) is known to be associated with fewer vascular complications and shorter hospital stay than the transfemoral approach. In the transradial approach, the insertion of a guiding catheter can be affected by the shape and vascular tortuosity of the brachiocephalic and subclavian arteries. In this study, we compared the left transradial with the right transradial approach in elderly patients. From 1 July 2008 to 30 April 2009, we performed CAG and angioplasty in 143 cases via the left transradial approach (Group I) and in 219 cases via the right approach (Group II). Among elderly patients over the age of 65 years, Group I consisted of 63 cases (71.8±5.17 years, male: 55.6%) and Group II consisted of 97 cases (72.7±5.16 years, male: 52.6%). We evaluated the degree of axillary tortuosity, the angle of the aorta to the subclavian artery, the procedural success rate, the fluoroscopic times, the size of the radial artery, and the procedure-related complications of both groups. The degree of axillary artery tortuosity and the angle of the aorta to the subclavian artery increased with age. In elderly patients, the degree of axillary tortuosity in Group I tended to be less severe than that in Group II (good:
82% vs 67.7%, mild: 11.5% vs 17.2%, moderate: 3.3% vs 8.6%, severe: 3.3% vs 6.5%, p=0.059), and the angle of the aorta to the subclavian artery was smaller in Group I (small: 95.1% vs 83.9%, moderate: 3.3%
vs. 5.4%, severe: 1.6% vs 10.8%, p=0.024). There was no statistical difference in the procedural success rate (96.8% vs. 89.7%, p=0.094), but the fluoroscopy time was significantly shorter in Group I (Group I:
46.8±26.4 sec, Group II: 58.2±36.6 sec, p=0.037). In elderly patients, the angle of the aorta to the subclavian artery was smaller and the fluoroscopy time was shorter via the left transradial approach compared with the right approach. We conclude that the left transradial approach is more effective and acceptable for elderly patients than the right approach.
Key Words: Coronary angiography; Radial artery; Aged
서 론
요골동맥(radial artery)을 이용한 관상동맥 조영술은 대 퇴동맥을 이용한 관상동맥 조영술에 비해 출혈 등의 혈관 부작용이 적으며 조기 보행이 가능하고 입원기간이 단축, 입 원비용 감소 등의 장점이 있어 현재 많이 이용되고 있다.1-4 또한 요골 동맥을 이용한 시술은 시술한 당일 퇴원이 가능 하며,5 급성 심근경색증 환자나 고령 환자에서도 성공적인 재관류를 이룰 수 있는 효과적이고 안전한 방법이라고 알려 져 있다.6,7 요골 동맥을 이용한 관상동맥 조영술은 시술자의 편의성때문에 대부분 우측 요골동맥을 이용하지만, 최근 들 어 우측 요골동맥과 좌측 요골동맥으로 접근하였을 경우의 차이와 효과적인 시술 방법에 대해 연구가 이루어지고 있 다.8-10 우측과 좌측의 요골동맥 주행이 해부학적으로도 정확 히 일치하지 않으며, 카테터의 주행이 요골동맥의 크기과 연 축, 완두동맥(brachiocephalic artery)과 쇄골하동맥(subcla- vian artery)의 모양과 혈관의 비틀림 정도(tortuosity) 등에 의해 영향을 받고, 고령, 여성, 저신장, 고혈압, 비흡연자, 비 만환자에서 혈관의 비틀림은 증가한다.11 좌측 요골동맥을 이용한 관상동맥 조영술이 우측 요골동맥을 이용한 시술보 다 총 시술 시간 단축 및 높은 성공률을 보이기 때문에 좌측 요골동맥을 이용한 시술이 더 효율적이라는 주장이 있으 나,12 나이가 증가함에 따라 혈관의 굴곡이 심화된다는 점과 좌측과 우측의 요골동맥 주행의 차이를 고려하여 볼 때 저 자 등은 65세 이상의 고령 환자에서 좌측 요골동맥과 우측 요골동맥을 이용한 관상동맥 조영술의 차이를 분석하여 더 효과적인 관상동맥 조영술의 접근 방법을 찾고자 하였다.
대상 및 방법
1. 대상
2008년 7월 1일부터 2009년 4월 30일까지 흉통이나 심 전도 변화, 심근 효소 이상을 주소로 본원에 내원한 환자 중 양측 모두 정상 Allen's test를 보이는 환자 362명을 대상으 로 하여 요골 동맥을 이용한 관상동맥 조영술을 시행하였다.
혈역학적으로 불안정한 환자, 요골동맥의 맥박이 만져지지 않은 환자, 말초혈관 질환을 가지고 있는 환자는 제외하였 고. 좌우 요골동맥의 선택은 무작위적으로 이루어졌다. 좌측 요골동맥을 이용한 환자 군이 143명(평균 61±11세, 남성 60.8%), 우측 요골동맥을 이용한 환자 군이 219명(평균
62±12세, 남성 60.3%)이었다. 그 중 65세 이상의 환자는 160명이었으며, 좌측 요골동맥을 이용한 환자는 63명(평균 72±5세, 남성 55.6%), 우측 요골동맥을 이용한 환자는 97 명(평균 73±5세, 남성 52.6%)이었다.
2. 방법
1) 시술 전 준비: 응급으로 관상동맥 조영술을 받은 환자 는 내원 시 응급실에서 aspirin 300 mg과 clopidogrel 600 mg 복용하였고, 예정된 관상동맥 조영술을 받은 환자는 첫 내원 시 aspirin 300 mg, clopidogrel 300 mg 복용 후 다음 날부터 aspirin 100 mg, clopidogrel 75 mg을 복용하였다.
Aspirin 100 mg과 clopidogrel 75 mg을 복용 중인 환자는 그대로 약물을 유지하였다. 관상동맥 중재술을 시행받은 환 자는 aspirin 100 mg, clopidogrel 75 mg, statin 등을 시술 후 지속적으로 복용하였다. 내원 시 모든 환자는 Allen's test를 받았고 시술 4∼6시간 전 리도카인 젤을 양 내측 손 목에 도포하였다. 환자와 보호자, 진료기록 등을 이용하여 과거력과 약물 복용력을 조사하였다.
2) 시술 방법: 모든 환자의 오른편에서 좌, 우 요골동맥을 이용한 시술이 이루어졌으며, 팔을 외전시키고 타월을 말아서 손목을 과신전시킨 상태에서 천자할 요골동맥의 위치에 리도 카인 피하 주사 후 18 G 바늘을 이용하여 천자하였다. 유도철 선을 진입시킨 후 fluoroscopy를 확인하면서 6∼7 Fr 카테터 를 삽입하였다. 요골동맥의 수축 시 nitroglycerin을 혈관 내 에 주사하였다. 시술 후 천자 부위는 Clo-Sur P.A.DTM (Scion Cadio-Vascular, Miami, FL)나 TR bandTM (Terumo Co., Tokyo, Japan)를 이용하여 지혈하였다.
3) 결과 분석: 전 연령군과 65세 이상의 환자군 각각에서 좌측 요골 동맥을 이용한 관상동맥 조영술과 우측 요골동맥 을 이용한 관상동맥 조영술 간의 성공률과 fluoroscopy time, 입원기간과 심혈관 합병증을 비교하였으며, 요골동맥 의 크기, 요골동맥과, 액와동맥의 비틀림 정도, 쇄골하동맥 과 완두동맥이 만나는 각도를 비교 관찰하였다.
4) 용어 정의: 시술 성공(procedural success)은 처음 시 도했던 천자 부위를 이용하여 좌, 우 관상동맥으로 진입하여 관상동맥 조영술을 시행한 후 필요 시 풍선확장술이나 스텐 트 삽입을 한 경우로 하였으며, 주요한 출혈(major blee- ding)은 헤모글로빈이 2 mg/dL 이상 감소하거나 수혈을 필 요로 하는 출혈로 하였고, fluoroscopy time은 천자 후 천자 부위에서 카테터가 관상동맥의 입구에 진입하였을 때까지의 시간, 요골동맥 크기는 상완요골 관절에서 15 cm 내외의
Lt. radial approach n=143
Rt. radial approach n=219
p value
Age (years) 61.02±11.45 61.57±11.97 0.667
Male 87 (60.8%) 132 (60.3%) 0.914
Hypertension 60 (42.0%) 114 (52.1%) 0.060
Diabetes 31 (21.7%) 56 (25.6%) 0.397
Current smoking 42 (29.4%) 70 (32.0%) 0.602 LDL-cholesterol
(mg/dL)
109.85±43.09 112.12±37.97 0.606
Ankle brachial index 1.08±0.11 1.09±0.11 0.340
Pulse wave velocity 0.730
Normal 59 (45.7%) 88 (44.9%)
Hardish 37 (28.7%) 51 (26.0%)
Hard 33 (25.6%) 57 (29.1%)
Ejection fraction (%) 65.3±10.73 70.2±6.27 0.351
PCI 37 (26.1%) 86 (39.8%) 0.007
CAD lesion
LAD 26 (18.2%) 62 (28.3%) 0.028
LCx 16 (11.2%) 34 (15.5%) 0.242
RCA 17 (11.9%) 46 (21.0%) 0.025
Number of stent used 0.44±0.84 0.63±0.83 0.036 Clinical diagnosis
STEMI 11 (7.7%) 36 (16.4%) 0.008
Unstable angina 20 (14.0%) 35 (16.0%) 0.605 Stable angina 27 (18.9%) 44 (20.1%) 0.777 Variant angina 1 (0.7%) 1 (0.5%) 0.761 Other chest pain 84 (58.7%) 103 (47.0%) 0.040 Lt, left; Rt, right; LDL, low densily lipoprotein; CAD, coronary artery disease; LAD, left anterior descending artery; LCx, left circumflex artery; RCA, right coronary artery; PCI, percutaneous coronary inter- vention; STEMI, ST segment elevation myocardial infarction; other chest pain, no lesion on coronary angiography.
Table 1. Clinical and angiographic characteristics in all patients
Lt. radial approach
n=63
Rt. radial approach
n=97
p value
Age (years) 71.86±5.17 72.74±5.16 0.291
Male 35 (55.6%) 51 (52.6%) 0.712
Hypertension 35 (55.6%) 60 (61.9%) 0.428
Diabetes 17 (27.0%) 28 (28.9%) 0.796
Current smoking 10 (15.9%) 19 (19.6%) 0.551 LDL-cholesterol
(mg/dL)
97.05±41.05 107.03±38.59 0.137
Ankle brachial index 1.06±0.15 1.07±0.15 0.137
Pulse wave velocity 0.545
Normal 19 (35.2%) 35 (40.2%)
Hardish 16 (29.6%) 23 (26.4%)
Hard 19 (35.2%) 29 (33.3%)
Ejection fraction (%) 65.2±11.07 62.1±14.17 0.141
PCI 17 (27.0%) 43 (45.3%) 0.020
Lesion location
LAD 13 (20.6%) 31 (32.0%) 0.117
LCx 7 (11.1%) 18 (18.6%) 0.205
RCA 8 (12.7%) 26 (26.8%) 0.033
Number of stent used 0.43±0.82 0.77±0.92 0.017 Clinical diagnosis
STEMI 4 (6.3%) 17 (17.5%) 0.848
Unstable angina 8 (12.7%) 20 (20.6%) 0.734 Stable angina 15 (23.8%) 24 (24.7%) 0.939 Other chest pain 36 (57.1%) 36 (37.1%) 0.948 Lt, left; Rt, right; LDL, low densily lipoprotein; LAD, left anterior descending artery; LCx, left circumflex artery; RCA, right coronary artery; PCI, percutaneous coronary intervention; STEMI, ST-segment elevation myocardial infarction; other chest pain, no lesion on coronary angiography.
Table 2. Clinical and angiographic characteristics in patients over the age of 65 years
가장 좁아진 부위의 지름을 측정하였다. 그리고 요골동맥의 tortuosity는 요골동맥의 주행 중 가장 굴곡이 심했을 때의 각도를 측정하여 mild: <30o, moderate: 30∼60o, severe:
>60o로 분류하였고, 액와동맥의 tortuosity는 액와동맥의 주행 중 가장 굴곡이 심했을 때의 각도를 측정하여 good:
<30o, mild: 30∼60o, moderate: 60∼90o, severe: >90o, angle of aortoperipheral artery는 쇄골하동맥과 완두동맥이 이루는 각을 측정하여 small: <10o, moderate: 10∼30o, severe: >30o로 분류하였다. 급성 콩팥 손상(acute kidney injury)은 조영제 주입 후 48시간 이내 혈청 크레아틴 수치 가 기저 크레아틴의 25% 이상 또는 절대치 0.5 mg/dL 이 상 상승한 경우로 정의하였다.
5) 통계 분석: SPSS 17.0을 이용하여 통계 분석하였고 연 속형 변수는 student's t-test, 범주형 변수에 대해서는 Pearson 카이제곱, 순위 변수에 대해서는 선형 대 선형 결
합을 이용하였고 일부 평균 비교에서는 Kruskal-Wallis 검 정을 사용하였다. 그리고 p값이 0.05보다 작을 때 통계학적 으로 유의하다고 정의하였다.
결 과
1. 대상 환자의 임상적, 관상동맥 조영술 소견의 특징 전체 환자에서 임상적으로 좌측 요골동맥을 이용한 군과 우측 요골동맥을 이용한 군의 나이, 성별, 흡연 유무의 차이 는 보이지 않았고, 고혈압, 당뇨병, 고지혈증 등의 유병률 차이도 없었다. 또한 ankle brachial index, pulse wave velocity, 좌심실 구혈률의 차이는 보이지 않았다. 한편 관상 동맥 조영술에서 우측 요골동맥을 이용한 군에서 관상동맥 중재술의 빈도가 더 높았다(Table 1). 65세 이상의 환자만
Fig. 1. (A) Relation of degree of axillary artery tortuosity with age. (B) Relation of angle of subclavian artery to brachiocephalic artery with age.
Lt. radial approach (n=143)
Rt. radial approach
(n=219)
p value
Angle of radial artery (o) 0.489
Mild 125 (92.6%) 193 (91.5%)
Moderate 7 (5.2%) 9 (4.3%)
Severe 3 (2.2%) 9 (4.3%)
Tortousity of axillary artery 0.023
Good 117 (86.0%) 164 (77.4%)
Mild 15 (11.0%) 29 (13.7%)
Moderate 2 (1.5%) 12 (5.7%)
Severe 2 (1.5%) 7 (3.3%)
Angle of aortoperipheral artery (o)
0.076
Small 126 (92.6%) 186 (87.7%)
Moderate 7 (5.1%) 12 (5.7%)
Severe 3 (2.2%) 14 (6.6%)
Table 3. Angiographic results in all patients
을 대상으로 하였을 경우에도 두 군 간의 관상동맥 중재술 의 빈도를 제외하고는 차이를 보이지 않았다(Table 2).
2. 동맥의 변형
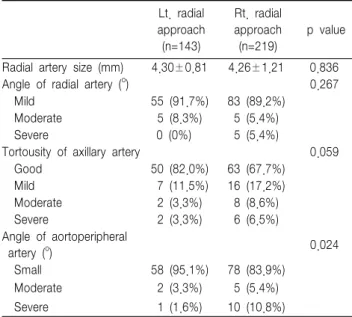
액와동맥의 비틀림과 쇄골하동맥과 완두동맥이 만나는 각 도는 고령일수록 증가하였다(Fig. 1). 전체 환자에서 좌측과 우측 요골동맥의 크기와 주행의 tortuosity는 차이를 보이지 않았다. 쇄골하동맥과 완두동맥이 만나는 각도는 좌측에서 완만한 경향을 보였지만, 통계학적으로는 차이를 보이지 못 하였으나(p=0.076), 액와동맥의 주행은 좌측에서 tortuo- sity가 의미 있게 적었다(p=0.023) (Table 3). 65세 이상의 환자 군에서도 요골동맥의 크기와 주행은 큰 차이를 보이지 못한 반면, 액와동맥의 tortuosity는 통계학적으로는 의미가 없었으나 좌측에서 더 적은 경향을 보였고(p=0.059), 쇄골 하동맥과 완두동맥이 만나는 각도는 의미있게 좌측에서 우 측보다 더 완만하였다(p=0.024) (Table 4).
3. 시술결과
65세 이상의 환자에서 시술 성공률은 좌측 요골동맥을 이 용한 군에서 96.%, 우측 요골동맥을 이용한 군에서 89.2%
로서 좌측 요골동맥을 이용한 군에서 더 높은 경향을 보였 지만 통계학적으로 의미는 보이지 않았다(p=0.094). Fluo- roscopy time은 좌측 요골동맥을 이용한 군에서 46.8±26.4 초, 우측 요골동맥을 이용한 군에서 58.2±36.6초로서 좌측 요골동맥을 이용한 군에서 의미 있게 더 짧았다(p=0.037).
입원 기간은 두 군 간의 유의한 차이는 보이지 않았다 (Group I: 6.8±12.11일, Group II: 7.2±5.18일, p= 0.789).
입원 기간 중 시술 관련 합병증은 심방 세동, 출혈, 천자 부위 감염, 뇌경색증, 급성 콩팥 손상 등이 발생하였으나, 두 군 간의 유의한 차이는 보이지 않았다(Table 5).
고 찰
이 연구에서는 나이가 증가함에 따라 혈관의 굴곡이 심화 된다는 점과 좌측과 우측의 동맥 주행이 차이가 발생함을 착안하여 65세 이상의 고령 환자에서 좌측 요골동맥을 이용 한 관상동맥 조영술과 우측 요골동맥을 이용한 관상동맥 조 영술의 효율성을 비교하였으며, 좌측 요골동맥을 이용한 시
Lt. radial approach (n=63)
Rt. radial approach (n=97)
p value
Success rate 61 (96.8%) 87 (89.2%) 0.094
Fluoroscopy time (sec) 46.8±26.4 58.2±36.6 0.037 Number of catheter use 1.06±0.25 1.07±0.26 0.834 Hospital stay (days) 6.83±12.11 7.20±5.18 0.789
Complications 4 (6.6%) 12 (12.4%) 0.268
Atrial fibrillation 0 2 0.245
Cerebral infarction 1 1 0.771
Major bleeding 1 3 0.535
Cardiogenic shock 0 1 0.413
Infection 1 1 0.771
Acute kidney injury 1 4 0.354
Table 5. Clinical outcomes and procedure complications in patients older than 65 years
Lt. radial approach (n=143)
Rt. radial approach (n=219)
p value
Radial artery size (mm) 4.30±0.81 4.26±1.21 0.836
Angle of radial artery (o) 0.267
Mild 55 (91.7%) 83 (89.2%)
Moderate 5 (8.3%) 5 (5.4%)
Severe 0 (0%) 5 (5.4%)
Tortousity of axillary artery 0.059
Good 50 (82.0%) 63 (67.7%)
Mild 7 (11.5%) 16 (17.2%)
Moderate 2 (3.3%) 8 (8.6%)
Severe 2 (3.3%) 6 (6.5%)
Angle of aortoperipheral
artery (o) 0.024
Small 58 (95.1%) 78 (83.9%)
Moderate 2 (3.3%) 5 (5.4%)
Severe 1 (1.6%) 10 (10.8%)
Table 4. Angiograhic results in patients over the age of 65 years
술이 성공률에는 통계학적으로 의미있는 향상을 보이지 않 았지만, 요골 동맥 천자에서 관상동맥까지 진입하는 시간이 의미 있게 감소한 것으로 미루어 보아 고령의 환자에서 좌 측 요골동맥으로 접근하는 것이 임상적으로 효과적임을 알 수 있었다. 관상동맥 조영술의 실패의 원인은 천자의 실패와 요골동맥의 수축, 요골동맥의 작은 혈관직경, 요골동맥, 액 와동맥, 쇄골하동맥의 심한 굴곡 등이었다.
Yoo 등10의 요골동맥의 분지 변형 및 사행성에 관한 고찰 연구에서 요골동맥의 사행성이 있는 환자의 나이가 유의하 게 많았고 이는 시술시간의 지연이나 혈관 국소 합병증의 발생에 관련이 있다고 보고하였으나, 이 연구에서는 요골동 맥의 굴곡에 따른 나이의 차이를 보이지 않았다. 이는 Yoo 등10 의 연구에서는 사행성의 정의를 굴곡이 중증도에 해당하는 기준을 사용하여 본 연구의 기준과 차이가 있었다. 또 Santas 등13은 좌측 요골동맥, 우측 요골동맥, 대퇴동맥을 이용한 관상동맥 조영술을 각각 비교하여 좌측 요골동맥 이 용 군과 우측 요골동맥 이용 군이 성공률, 합병증, 시술 시 간의 차이가 없음을 보고하였고 좌측 요골동맥은 대퇴동맥 이나 우측 요골동맥의 대안이 될 수 있다고 주장하였다. 한 편, Kim 등12의 좌측과 우측의 요골동맥을 이용한 관상동맥 조영술 비교 연구에서 좌측 요골동맥을 이용한 관상동맥 조 영술 (좌측 군)의 성공률이 통계학적 차이를 보이지 않았지 만, 우측 군보다 더 높은 경향을 보였고 총 시술시간은 좌측 군에서 더 짧았고 다른 부위로 천자 부위를 바꾸는 경우도 좌측 군에서 통계학적으로 낮았다. 본 연구에서처럼 고령 환
자에서도 Kim 등12의 연구와 유사한 결과를 보였다. 향후 좀 더 많은 환자를 대상으로 연령에 따른 분석을 한다면 나 이에 따른 효과적인 접근 방법을 찾을 수 있을 것이라고 기 대된다.
일반적으로 요골 동맥을 이용한 관상동맥 조영술은 시술 자의 대부분이 오른손잡이여서 카테터 등의 조작이 쉬운 환 자의 오른편에서 이루어지며 시술자와 가까운 우측 요골동 맥을 가장 먼저 이용하게 된다. 그러나 우측 요골동맥을 이 용하는 경우 환자의 우측에서 쉽고 익숙하게 도관을 조작할 수 있으나 완두동맥의 굴곡과 동맥 경화에 의해 실패율이 증가한다는 지적이 있으며, 좌측 쇄골하동맥은 심한 사행성 의 빈도가 적어 좌측 요골동맥을 이용하는 경우 시술에 이 점을 가진다는 주장이 있다.14,15 이 연구에서도 65세 이상의 환자에서 우측 요골동맥을 이용한 시술이 좌측 요골동맥을 이용한 시술에 비해 더 나은 점은 보이지 않았고 좌측 동맥 의 굴곡이 우측보다 더 적어 관상 동맥까지 접근하는 시간 이 단축되었다. 또한 관상동맥 우회수술이 필요한 경우 시행 되는 좌측 속가슴동맥(internal thoracic artery) 조영 시에 좌측 요골동맥으로 접근하는 것이 필수적이어서 우측 요골 동맥으로 시행 시 좌측 요골동맥 접근이 더 필요하게 된다.
또한 한국 사람은 오른손잡이가 많으므로 좌측 요골동맥으 로 하였을 경우에 시술 후 일상생활이 더 용이하다고 할 수 있다.
시술 후 출혈은 주로 천자 부위에서 발생하고 이는 사망 률에 영향을 끼치고 재원기간을 연장시키며 항혈소판제 등 의 사용을 제한시켜 예후에 영향을 준다. 많은 연구에서 대 퇴 동맥을 이용한 관상동맥 조영술에서 요골동맥을 이용한
시술보다 출혈 부작용이 더 많이 발생된다고 알려져 있으며, 요골동맥을 이용한 시술이 천자 부위의 출혈을 줄이는 대안 으로 제시되고 있다.19,20 좌측과 우측 요골동맥을 이용한 관 상 동맥 조영술의 혈관 부작용의 차이는 Kim 등12의 연구와 Santas 등13 연구 등에서 보이지 않았으며, 본 연구에서 마 찬가지로 고령 환자에서도 유의한 차이를 보이지 않았다.
본 연구의 제한점으로는 동맥의 굴곡 정도를 분류하는 통 용되는 기준이 존재하지 않아 본원에서 임의로 분류하였고 그 분류에 따른 각 기준들이 관상동맥 조영술에 어떤 영향 을 끼치는 지는 연구되지 못하였다는 것이다.
결론적으로 본 연구를 통하여 65세 이상의 고령 환자에서 요골동맥, 액와동맥, 쇄골하동맥, 완두동맥의 우측과 좌측의 주행에 있어서 차이점이 있었고, 그에 따른 관상동맥 조영술 의 효율은 좌측 요골동맥을 이용함이 우측 요골동맥보다 더 좋았다는 것을 알 수 있었다.
References
1. Louvard Y, Benamer H, Garot P, Hildick-Smith D, Loubeyre C, Rigattieri S, et al. Comparison of transradial and transfemoral approaches for coronary angiography and angioplasty in octogenarians (the OCTOPLUS Study).
Am J Cardiol 2004;94:1177-80.
2. Archbold RA, Robinson NM, Schilling RJ. Radial artery access for coronary angiography and percutaneous coronary intervention. BMJ 2004;329:443-6.
3. Agostoni P, Biondi-Zoccai GG, de Benedictis ML, Rigattieri S, Turri M, Anselmi M, et al. Radial versus femoral approach for percutaneous coronary diagnostic and interventional procedures; systematic overview and meta-analysis of randomized trials. J Am Coll Cardiol 2004;44:349-56.
4. Brueck M, Bandorski D, Kramer W, Wieczorek M, Höltgen R, Tillmanns H. A randomized comparison of transradial versus transfemoral approach for coronary angiography and angioplasty. JACC Cardiovasc Interv 2009;2:1047-54.
5. Oh HL, Gwon HC, Lee SM, Kim YH, Cheon IS, Cheon WJ, et al.
Safety of one-day admission transradial coronary intervention. Korean Circ J 2004;34:647-54.
6. Park SJ, Park JH, Lee JH, No SP, Park HS, Park YK, et al. The clinical feasibility of transradial primary percutaneous coronary intervention with an ST elevation acute myocardial infarction. Korean Circ J 2007;37:72-7.
7. Chun KJ, Kim JH, Hong TJ, Chun TH, Shin YW. The safety and
feasibility of transradial coronary angiography over 70-year-old patients.
Korean Circ J 2004;34:376-80.
8. Kawashima O, Endoh N, Terashima M, Ito Y, Abe S, Ootomo T, et al. Effectiveness of right or left radial approach for coronary angiography.
Catheter Cardiovasc Interv 2004;61:333-7.
9. Yoo BS, Lee HH, Yoon J, Lee SH, Kim JY, Lee BK, et al. The study of branching anomaly and tortuosity of radial artery for trans-radial coronary procedure. Korean Circ J 2000;30:82-9.
10. Yoo BS, Yoon JH, Ko JY, Kim JY, Lee SH, Hwang SO, et al. Anatomical consideration of the radial artery for transradial coronary procedures:
arterial diameter, branching anomaly and vessel tortuosity. Int J Cardiol 2005;101:421-7.
11. Cha KS, Kim MH, Kim HJ. Prevalence and clinical predictors of severe tortuosity of right subclavian artery in patients undergoing transradial coronary angiography. Am J Cardiol 2003;92:1220-2.
12. Kim JY, Yoon J, Jung IH, Wang HS, Jung HS, Yoo BS, et al. Transradial coronary intervention: comparison of the left and right radial artery approach. Korean Cir J 2006;36:780-5.
13. Santas E, Bodi V, Sanchis J, Núñez J, Mainar L, Miñana G, et al.
The left radial approach in daily practice. A randomized study comparing femoral and right and left radial approaches. Rev Esp Cardiol 2009;62:
482-90.
14. Fernández-Portales J, Valdesuso R, Carreras R, Jiménez-Candil J, Serrador A, Romaní S. Right versus left radial artery approach for coronary angiography. Difference observed and the learning curve. Rev Esp Cardiol 2006;59:1071-4.
15. Wu CJ, Lo PH, Chang KC, Fu M, Lau KW, Hung JS. Transradial coronary angiography and angioplasty in Chinese patients. Catherter Cardiovasc Diagn 1997;40:159-63.
16. Vavalle JP, Rao SV. The association between the transradial approach for percutaneous coronary interventions and bleeding. J Invasive Cardiol 2009;21(8 Suppl A):21A-4A.
17. Hamon M, Coutance G. Transradial intervention for minimizing bleeding complications in percutaneous coronary intervention. Am J Cardiol 2009;104(5 Suppl):55C-9C.
18. Rao SV, Ou FS, Wang TY, Roe MT, Brindis R, Rumsfeld JS, et al.
Trends in the prevalence and outcomes of radial and femoral approaches to percutaneous coronary intervention: a report from the National Cardiovascular Data Registry. JACC Cardiovasc Interv 2008;1:379-86.
19. De Carlo M, Borelli G, Gistri R, Ciabatti N, Mazzoni A, Arena M, et al. effectiveness of the transradial approach to reduce bleedings in patients undergoing urgent coronary angioplasty with GPIIb/IIIa inhibitors for acute coronary syndromes. Catheter Cardiovasc Interv 2009;74:408-15.
20. Eichhöfer J, Horlick E, Ivanov J, Seidelin PH, Ross JR, Ing D, et al.
Decreased complication rates using the transradial comprared to the transfemoral approach in percutaneous coronary intervention in the era of routine stenting and glycoprotein platelet IIb/IIIa inhibitor use: a large single-center experience. Am Heart J 2008;156:864-70.