Original Article
제2형 당뇨병 환자에서의 Liraglutide 투여와 급성 췌장염 발생의 연관성: 메타분석
이영훈a, 박정규b, 최혜덕a†
영남대학교 약학대학a, 영남대학교병원 약제부b
The Associations Between Liraglutide and Risk of Acute Pancreatitis in Patients with Type 2 Diabetes : A Meta-analysis
Young Hoon Leea, Jung Kyu Parkb and Hye Duck Choia,†
College of Pharmacy, Yeungnam University,
280 Daehak-ro, Gyeongsan, Gyeongsangbuk-do, 38541, Republic of Koreaa Department of Pharmacy, Yeungnam University Hospital
170 Hyeonchung-ro, Nam-gu, Daegu, 42415, Republic of Koreab
투고일자 2020.6.23; 심사완료일자 2020.7.21; 게재확정일자 2020.10.21
†교신저자 최혜덕 Tel: 053-810-2815 E-mail: [email protected]
Background : Acute pancreatitis is an important and serious disease even with a relatively low incidence. Also, previous studies suggest that the coexistence of Type 2 diabetes and acute pancreatitis is closely related to an increased risk of death. However, the risk of acute pancre- atitis in patients treated with liraglutide, a GLP-1 receptor agonist, has not been adequately evaluated.
Objective : This meta-analysis was conducted to investigate the association between the lira- glutide and acute pancreatitis in patients with Type 2 diabetes.
Methods : Forty-one studies were assessed, and the results of the included studies were quan- titatively integrated using the meta-analysis. The incidence of the liraglutide-related acute pancreatitis was estimated. As a sub-group analysis, four studies were assessed for comparing the liraglutide-treated groups and the control groups (placebo or other antidiabetic drugs ex- cept GLP-1 receptor agonists).
세계보건기구의 데이터에 의하면 당뇨병은 21세기 에 들어 현대인의 사망 10대 원인 중 하나이다.1) 특 히 대한당뇨학회의 데이터에 의하면 우리나라 성인의 당뇨병 유병률은 2010년 10.1%에서 2016년 14.4
%로 빠르게 증가하는 경향을 보였으며, 2016년 기 준으로 성인 7명 중 한 명이 당뇨병인 것으로 나타났 다.2) 공복혈당장애 유병률 또한 2011년 19.3%에서 2016년 25.3%로 증가하였고, 특히 성인 남성의 경 우 31.0%로 약 3명 중 1명이 잠재적 위험군인 것으 로 나타나, 당뇨병의 관리와 적합한 치료에 대한 관심 이 필요한 시점이다.2)
Liraglutide는 glucagon-like peptide-1 (GLP-1) 수용체 효능제 중 하나로, dipeptidyl peptidase-4 (DPP-4) 억제제와 함께 인크레틴 기 반 치료로 사용되고 있는 약물이다. Liraglutide는 다른 경구용 당뇨병 치료제에 비해 당화혈색소, 공복 혈당치 감소 능력이 뛰어나면서도 저혈당 부작용이 적다는 이점을 가지고 있어, 제2형 당뇨병 치료에 성 공적으로 사용되고 있을 뿐만 아니라, 체중감량의 부 가적인 이점이 있어 비만 치료를 위해서도 사용되고 있다.3),4)
제3상 임상시험에 의하면, liraglutide의 가장 흔 한 부작용은 오심, 설사, 변비, 구토 등의 위장관 관 련 증상으로 투여 받은 환자의 약 36%에서 관찰되었 다.5) 또한, 최근 연구에 따르면 낮은 빈도이긴 하나 급성 췌장염을 촉진시키거나 신생물을 포함한 만성 췌장염을 일으키는 등 췌장과 관련된 여러 가지 잠재 적인 위험을 가지고 있다는 문제가 보고되고 있다.6) Liraglutide의 급성 췌장염 발생 기전은 최근 연
구들을 통해 알려져 있다. GLP-1은 췌장의 내분비 를 담당하는 랑게르한스섬의 β세포를 자극하여 재생 을 촉진시킬 뿐만 아니라 외분비세포에도 직접적인 영향을 미친다. 특히, 췌장 도관 상피세포(pancre- atic ductal epithelium)의 증식 신호를 자극하여 도관을 증식 시키는 작용을 하며 이 과정에서 도관의 폐색을 유발한다. 도관 폐색은 역압을 유발하여 샘꽈 리 세포(acinar cells)에 스트레스를 주며, 그 결과 샘꽈리 세포가 과활성화 되어 소화효소의 과도한 분 비를 유도한다. 과도한 소화효소의 분비는 잘 알려진 췌장염의 발생 원인 중 하나이다.6)
급성 췌장염의 전체 사망률은 약 2~3%이며 환자의 15~20%는 췌장 괴사와 같은 심각한 질환으로 발전 할 수 있다.7),8) 뿐만 아니라, 제2형 당뇨병과 급성 췌 장염의 공존은 사망률 증가와 밀접한 관련이 있다.
Huh et al.의 연구에 의하면, 애틀랜타 분류(At- lanta classification)를 적용하여 분석한 결과 급 성 췌장염과 당뇨병을 동시에 지닌 환자의 경우 급성 췌장염만 지닌 환자에 비해 사망률이 증가하는 결과 를 보였다(OR=7.76; 95% CI: 1.26–47.63, p=
0.027).9) 따라서 당뇨병 환자에게 급성 췌장염은 중 대한 부작용 중 하나이다. 이와 관련하여 최근에는 여 러 당뇨병 치료제와 급성 췌장염의 연관성에 대한 연 구들이 진행되고 있다. 특히 Li L et al.의 연구에 의 하면 GLP-1 효능제나 DPP-4 억제제를 포함하는 인크레틴 기반 치료를 받은 환자들 사이에서 급성 췌 장염의 발생률이 낮고 위험을 증가시키지 않는다는 결론을 내렸지만, 확정적인 결론은 아니며 더 정교하 게 설계된 관찰 연구가 필요함을 강조했다.10) Results : The incidence of acute pancreatitis was 0.4% (95% confidence interval (CI) 0.3%-0.5%).
The risk of acute pancreatitis was not significantly different between the liraglutide-treated groups and the control groups (odds ratio=1.412; 95% CI 0.290-6.866).
Conclusion : The incidence of liraglutide-related acute pancreatitis was relatively low and not additionally increased compared to the other antidiabetic drugs. We suggest that this me- ta-analysis is meaningful as evidence for the clinical use of liraglutide.
[Key words] Liraglutide, Acute pancreatitis, Meta-analysis, Type 2 diabetes
Garber et al.의 LEAD-3 연구 결과를 보면, glimepiride 8 mg 투여군에서는 급성 췌장염이 관 찰되지 않은 반면, liraglutide 1.2 mg 투여군 251명 중 1명, liraglutide 1.8 mg 투여군 247명 중 1명으로, 총 2명의 급성 췌장염이 관찰되었다.11) 이는 발생빈도는 높지 않으나 liraglutide 투여와 급성 췌장염 발생 사이의 연관성을 배제할 수 없다는 것을 뒷받침한다. 그러나 Marso et al.의 연구에서 는 liraglutide 1.8 mg 투여군 4,668명 중 18명, 위약 투여군 4,672명 중 23명의 급성 췌장염이 관찰 되었고, liraglutide 투여군에서 위약 투여군보다 급성 췌장염의 발생률은 낮다는 결과가 나왔다.12) 위 와 같이 연구마다 그 결과가 상이하여 하나의 통합된 결론을 도출하는데 한계가 있다.
따라서, 본 연구는 제2형 당뇨병 환자를 대상으로 liraglutide 투여와 관련된 급성 췌장염 발생 정도를 평가하기 위해 메타분석을 실시하였다.
연구방법
1. 문헌 검색 및 선정(Search strategy and study selection)
검색에 포함된 데이터베이스는 Pubmed와 Coch- rane library이고 2019년 1월 31일에 검색을 완료 하였다. 검색어로는 ‘Liraglutide’, ‘Randomiz- ed controlled trial’를 적용하였다.
문헌 선정 과정에는 다음과 같은 기준을 적용하였 다.
(1) 연구의 설계형태(study design)는 제2형 당 뇨병 환자를 대상으로 liraglutide를 투여한 무작위 대조 시험을 포함하였음.
(2) 환자군은 만 18세 이상의 성인으로, 질환이나 성별에 제한 없이 liraglutide를 투여 받은 경 우를 포함하였음.
(3) 결과값은 liraglutide 투여에 따른 급성 췌장 염 발생 환자 수(N)를 관찰하는 문헌을 포함하 였음.
(4) 자료의 출판 형태는 전문(full-text)을 볼 수 있는 문헌을 선정하였고, 출판 언어는 한국어와 영어로 제한하였음.
2. 자료 추출 및 연구 질 평가(Data extraction and quality assessment)
최종적으로 선정된 문헌에서 연구설계, 대상집단, 약물 투여 기간 및 용량, 급성 췌장염 발생 환자 수 등 의 자료를 추출하였다.
연구 질 평가 단계에서는 자다드 질 평가척도(Ja- dad’s quality assessment scale)를 사용하여 평가하였다.13) 두 명의 연구자가 질 평가를 독립적으 로 수행하였고, 의견이 일치하지 않는 경우 논의를 거 쳐 최종적인 평가 결과를 도출하였다. 평가 척도는 무 작위화의 설명, 무작위화 방법의 적절성, 이중 맹검 의 설명, 이중 맹검 방법의 적절성, 중단 및 탈락에 대한 설명의 5가지 항목을 사용하여 평가하였다. 최 고 점수는 5점이며 3점보다 높은 경우 연구의 질이 상 대적으로 높은 것으로 간주하였다.
3. 정량적 합성 및 통계 분석(Quantitative syn- thesis and statistical analysis): 메타분석(Me- ta-analysis)
Liraglutide를 투여 받은 환자에서 급성 췌장염 발생 위험을 평가하기 위해 메타분석을 실시하였다.
추가적으로 liraglutide 투여군과 대조약물 투여군 의 급성 췌장염 발생 위험비교를 위한 메타분석도 실 시하였다. 메타분석에 사용된 프로그램은 Compre- hensive Meta-Analysis software (version 2;
CMA 26526; Biostat, Englewood, NJ, USA) 이다. 통계적 모델은 고정효과모형(fixed-effect model)과 무작위효과모형(random-effect mod- el)을 각각 적용한 후 비교하였다.14)
이질성(heterogeneity) 분석에서는 카이제곱검 정(Q statistics)과 Higgin’s I2 검정을 활용해 검 증하였다.15) 출판비뚤림(publication bias)을 측 정하기 위해 Begg의 순위상관검정(Begg’s rank correlation method)과 Egger의 선형회귀검정 (Egger’s regression method)을 활용했다.16),17) P<0.05인 경우, 통계적으로 유의한 결과로 판단하 였다.
민감도 분석(sensitivity analysis)은 각 연구를 차례로 배제한 후 메타 분석 추정치를 계산하는 방식
으로 수행되었다.
연구결과
1. 연구의 특성 및 질 평가(Study quality and char- acteristics)
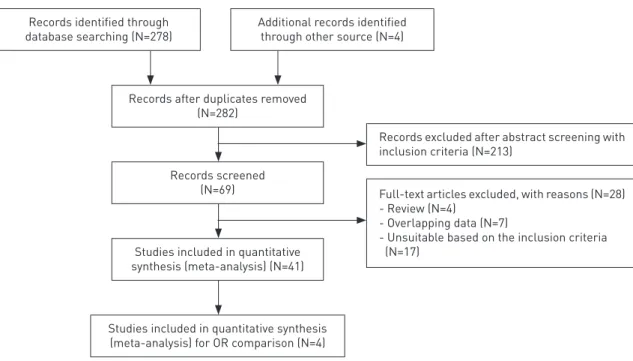
PubMed에서 278건, Cochrane Library에서 4건의 문헌들이 검색되었고, 최종적으로 41개의 논 문이 선정되었다(Fig. 1).
41개 논문의 데이터를 추출하여 분석한 결과 전체 연구에서 liraglutide를 투여 받은 환자는 총 13,878명 이었다(Table 1). 각 연구에서 대조군 의 치료약물로는 위약이나 경구용 혈당강하제 등이 투여 되었으며, GLP-1 receptor agonist 계열 (exenatide,23),27) semaglutide,46),56) dulaglu- tide,31),38) albiglutide,32) lixisenatide29),45))의 약물이 투여된 연구도 있었다. Liraglutide 투여군 에서 투여 용량은 최소 0.3 mg에서 최대 3.0 mg으 로 다양하게 나타났으며, 적정 기간을 두고 초기 0.6 mg에서 1.8 mg으로 증량하는 하는 방법의 연구도
있었다.33),50) 투여 기간은 최소 3주에서부터 최대
198주까지 투여하였으며, 평균 투여 기간은 약 34.8 주로 나타났다. 각 연구에 포함된 환자의 평균연령은 최소 51세에서 최대 68.3세로 연구 간 큰 차이는 없 었다. 자다드 질 평가 척도를 사용하여 질 평가한 결 과 평균 4.02로 전반적으로 높은 점수가 나왔다.
2. Liraglutide 투여군에서 급성 췌장염의 발생률 (The incidence of acute pancreatitis in lira- glutide treated group)
41개의 연구에 대하여 분석한 결과 liraglutide를 투여 받은 환자 13,878명 중 급성 췌장염 발생 환자 수는 25명이었다. 메타분석 결과에서 급성 췌장염의 발생률(event rate)과 95% 신뢰구간(confidence interval, CI)은 0.4%(0.3-0.5%)로 나왔으며, 따라서 liraglutide 투여 시 급성 췌장염의 발생률은 약 0.4%로 추정할 수 있다. 이질성 평가 결과 I2값이 0으로 나왔으므로 이질성이 없다고 판단하였고, 고 정효과모형과 무작위효과모형을 각각 적용하여 비교 한 결과에서도 유의한 차이가 없었다.
Records identified through
database searching (N=278) Additional records identified through other source (N=4)
Records after duplicates removed (N=282)
Records screened (N=69)
Studies included in quantitative synthesis (meta-analysis) (N=41)
Studies included in quantitative synthesis (meta-analysis) for OR comparison (N=4)
Records excluded after abstract screening with inclusion criteria (N=213)
Full-text articles excluded, with reasons (N=28) - Review (N=4)
- Overlapping data (N=7)
- Unsuitable based on the inclusion criteria (N=17)
Fig. 1 Flow of information from identification to inclusion of studies
Liraglutide 0.65 mg 40(67.5/32.5) Liraglutide 1.25 mg 42(55/45) Liraglutide 1.90 mg 41(73/27)
Placebo 40(47.5/52.5)
Liraglutide 1.2 mg 178(57/43) Liraglutide 1.8 mg 178(51/49)
Placebo 177(62/38)
Liraglutide 0.6 mg 233(54/46) Liraglutide 1.2 mg 228(45/55) Liraglutide 1.8 mg 234(53/47)
Placebo 114(47/53)
Rosiglitazone 232(47/53) Liraglutide 0.6 mg 242(62/38) Liraglutide 1.2 mg 240(54/46) Liraglutide 1.8 mg 242(59/41) Glimepiride 4 mg 242(57/43)
Placebo 121(60/40)
Liraglutide 1.8 mg 230(57/43) Insulin glargine 232(49/51)
Placebo 114(60/40)
Liraglutide 1.8 mg 233(49/51) Exenatide 10 μg 231(55/45) Liraglutide 0.6 mg 88(60/40) Liraglutide 0.9 mg 88(67/33)
Placebo 88(65/35)
Liraglutide 1.2 mg 225(52/48) Liraglutide 1.8 mg 221(52/48) Sitagliptin 100 mg 219(55/45) Liraglutide 0.6 mg 231(54.1/45.9) Liraglutide 1.2 mg 233(54.9/45.1) Liraglutide 1.8 mg 234(53.8/46.2) Glimepiride 4 mg 231(58.4/41.6) Liraglutide 1.2 mg 251(47/53) Liraglutide 1.8 mg 247(49/51) Vilsboll
(2007)18)
Zinman (2009)19)
Marre (2009)20)
Nauck (2009)21)
Russell-Jones (2009)22)
Kaku (2010)24) Buse (2009)23)
Garber (2011)11)
≥18 years
18–80 years
18–80 years
18–80 years
18–80 years
≥20 years 18–80 years
18–80 years 14
26
26
104
26
52 26
104
0 0 5
0 0 5
0 0 5
1 1 5
0 0 3
0 0 4
Pratley (2010)25) 18–80 years 52 0 0 4
Yang (2011)26) 18–80 years 16 0 0 5
0 0 3
2 0 5
Table 1 Characteristics of included studies for overall incidence of pancreatitis in liraglutide treated group
First
author Population Jadad
score No. of acute pancreatitis Treatment
Liraglutide Duration
(weeks) Regimen N(M%/F%) Controls
Glimepiride 8 mg 248(54/46) Liraglutide 1.8 mg 450(54/46) Exenatide 2 mg 461(55/45) Liraglutide 1.8 mg 20(55/45)
Placebo 20(55/45)
Lilaglutide 1.8 mg 71(70/30) Lixisenatide 77(64/36) Liraglutide 1.8 mg 327(55/45) Sitagliptin 100 mg 326(55/45) Liraglutide 1.8 mg 300(50/50) Dulaglutide 1.5 mg 299(46/54) Lilaglutide 1.8 mg 408(53/47)
Albiglutide 404(47/53)
Liraglutide 0.6 to 1.8 mg 88(72/28)
Aspart 89(60/40)
Liraglutide 1.8 mg 26(61.5/38.5)
Placebo 25(64/36)
Liraglutide 1.8 mg 16(64/36)
Placebo 16(64/36)
Glimepiride 4 mg 17(65/35) Liraglutide 1.8 mg 225(53.3/46.7)
Placebo 225(60.4/39.6)
Lilaglutide 1.8 mg 64(62.5/37.5)
Placebo 60(66.7/33.3)
Liraglutide 0.9 mg 137(82/18) Dulaglutide 0.75 mg 280(81/19)
Placebo 70(NR/NR)
Liraglutide 1.8 mg 470(56/44) Insulin glargine 474(53/47) Liraglutide 3.0 mg 423(52/48) Liraglutide 1.8 mg 211(51/49)
Placebo 212(46/54)
Liraglutide 0.9 mg 22(60/40)
Metfomin 24(66.7/33.3)
18–80 years 104
Buse (2013)27) ≥18 years 26 0 1 3
Hermansen
(2013)28) 18–75 years 3 0 0 5
Kapitza
(2013)29) 37-74 years 4 0 0 2
Dungan
(2014)31) ≥18 years 26 0 0 3
Mathieu
(2014)33) ≥18 years 28 0 1 3
Ahmann
(2015)36) 18–80 years 26 0 0 5
Nandy (2014)35) 40–70 years 12 0 0 5
Odawara
(2015)38) ≥20 years 52 0 0 3
Davies (2015)40) ≥18 years 56 0 0 5
Tanaka (2015)41) 20–75 years 24 0 0 3
D’Alessio
(2015)39) 35–75 years 24 1 0 3
Lind (2015)37) 40–70 years 24 0 0 5
Charbonnel
(2013)30) 18–79 years 26 0 0 3
Pratley (2014)32) 18–79 years 32 2 1 3
Retnakaran
(2014)34) 30–75 years 48 0 0 4
2 0 5
First
author Population Jadad
score No. of acute pancreatitis Treatment
Liraglutide Duration
(weeks) Regimen N(M%/F%) Controls
Garber (2011)11)
Liraglutide 1.8 mg 4668(65/35)
Placebo 4672(64/36)
Liraglutide 0.9 mg 240(76/24)
Sitagliptin 100 mg 204(61/39)
≥50 years with at least one cardiovascular
coexisting condition or ≥60
years with at least one cardi-
ovascular risk factor
198 18 23 5
First
author Population Jadad
score No. of acute pancreatitis Treatment
Liraglutide Duration
(weeks) Regimen N(M%/F%) Controls
Marso (2016)12)
a-GI*
Glinide Metformin Thiazolidinedione
Liraglutide 0.6 mg to 1.8 mg
120(66.7/33.3)
202(58/42) Kaku
(2016)42) ≥20 years 52 0 0 3
Azar (2016)43) 18–80 years 33 0 0 3
Nauck
(2016)45) ≥18 years 26 0 0 3
Seino
(2016)47) ≥20 years 36 0 0 5
Zang
(2016)49) 18–80 years 26 0 0 3
Bailey
(2016)50) ≥18 years 26 0 0 5
Nauck
(2016)46) ≥18 years 12 0 0 3
Vanderheiden
(2016)48) ≥18 years 26 0 0 5
Davies
(2016)44) 18–80 years 26 0 0 5
Liraglutide 1.8 mg 171(50/50) Sulphonylurea 170(49/51) Liraglutide 1.8 mg 140(54/46)
Placebo 137(47/53)
Liraglutide 1.8 mg 202(65/35) Lixisenatide 20 μg 202(55/45) Liraglutide 1.2 mg 45(69/31) Liraglutide 1.8 mg 50(70/30) Semaglutide 0.1 mg 47(66/34) Semaglutide 0.2 mg 43(70/30) Semaglutide 0.4 mg 48(77/23) Semaglutide 0.8 mg 42(52/48) Semaglutide 0.8 mg E† 43(63/37) Semaglutide 1.6 mg E 47(55/45)
Placebo 46(61/39)
Liraglutide 0.9 mg 127(54/46)
Placebo 130(58/42)
Liraglutide 1.8 mg 35(34/66)
Placebo 36(39/61)
Liraglutide 1.8 mg 183(56/44) Sitagliptin 100 mg 184(64/36)
Liraglutide 1.8 mg 19(74/26) Sitagliptin 100 mg 19(84/16)
Placebo 17(76/24)
Liraglutide 0.9 mg 8(63/37)
Insulin 9(33/67)
Liraglutide 1.8 mg 35(48.6/51.4) NNC0090-2746¶ 1.8 mg 37(48.6/51.4)
Placebo 36(38.9/61.1)
Liraglutide 0.3 mg 64(45/55) Liraglutide 0.6 mg 64(50/50) Liraglutide 1.2 mg 64(53/47) Liraglutide 1.8 mg 65(51/49) Semaglutide 0.05 mg 64(52/48) Semaglutide 0.1 mg 63(56/44) Semaglutide 0.2 mg 65(66/34) Semaglutide 0.3 mg 63(51/49) Semaglutide flexible dose 64(56/44)
Placebo 129(56/44)
3. Liraglutide 투여군과 대조군 간의 비교(Com- parisons between liraglutide and compara- tor treated groups)
다른 경구용 당뇨병 치료제 투여군에 대한 급성 췌 장염 발생 위험을 비교하기 위한 메타분석을 실시하
였다. 41개의 연구 중 대조군이 위약이거나 GLP-1 receptor agonist 계열 약물인 연구를 제외하고 급 성 췌장염 발생 환자 수가 실험군과 대조군에서 모두 0인 연구를 배제한 후 총 4개의 연구가 포함되었다.
Liraglutide 투여군은 총 1,502명, 대조군은 총 1,030명 이었다. 메타분석 결과 다른 경구용 당뇨병 First
author Population Jadad
score No. of acute pancreatitis Treatment
Liraglutide Duration
(weeks) Regimen N(M%/F%) Controls
Kumar- athurai (2016)52)
Patients with stable CAD§,
LVEF∥>40%
and newly diagnosed type 2 diabetes
12 Idorn
(2016)51)
18–85 years, Type 2 diabetes
with ESRD‡ 12 0 0 5
Smits
(2017)53) 35–75 years 12 0 0 5
Frias
(2017)55) 18–70 years 12 0 0 5
Lingvay
(2018)56) ≥18 years 26 0 2 4
Bouchi
(2017)54) ≥20 years 36 0 0 3
0 0 5
Liraglutide 1.8 mg (ESRD) 10(80/20) Liraglutide 1.8 mg 10(70/30) Placebo (ESRD) 10(90/10)
Placebo 10(80/20)
Liraglutide 1.8 mg 39(79/21)
Placebo 39(79/21)
*a-GI : Alpha-glucosidase inhibitor, †E : With dose escalation, ‡ESRD : End-stage renal disease,
§CAD : Coronary artery disease, ∥LVEF : Left ventricular ejection fraction, ¶NNC0090-2746 : Dual GIP/GLP-1 receptor agonist
치료제 투여군에 대한 liraglutide 투여군의 췌장염 발생 OR 결합 추정치 및 95% 신뢰구간은 1.412 (0.290–6.866)로 두 군 간에 유의성 있는 차이는 관 찰되지 않았다(Fig. 2).
4. 민감도 분석 및 출판 비뚤림 평가(Sensitiv- ity analyses and publication bias)
민감도 분석은 각 연구를 차례대로 배제 한 후 메타 분석 결과를 재계산하여 수행하였으며 유의한 값은 관찰되지 않았다.
출판 비뚤림 평가를 위해 4개의 연구들에 대해 수행 된 Begg의 순위상관검정법(Begg’s rank corre- lation method) 및 Egger의 선형회귀검정(Eg- ger’s regression method) 결과는 Table 2에 정 리하였다.
고찰
본 메타분석은 제2형 당뇨병 환자에서 liraglu- tide 투여와 관련된 급성 췌장염 발생 정도를 평가하 기 위해 실시되었다. 메타분석 결과 liraglutide 투 여 시 급성 췌장염 발생률은 0.4%(95% CI 0.3- 0.5)로 확인되었다. 기존의 LEADER 임상시험 결 과, liraglutide에 대한 급성 췌장염 발생률은 0.4%이며 위약에 대한 발생률은 0.5%였다.12) 이와 유사하게 Pratley et al.에 의해 수행된 제3상 임상 시험 연구 결과 liraglutide 투여군 284명 중 1명으 로 약 0.4%, 위약 투여군은 142명 중 1명으로 약 0.7%의 발생률을 나타냈다.57)
Liraglutide 투여군과 다른 당뇨병 치료제 투여군 에서 급성 췌장염의 발생 위험을 비교한 메타분석 결 과에서 통계적으로 유의한 차이는 관찰되지 않았다 (OR=1.412; 95% CI: 0.290–6.866)(Fig. 2).
Alves et al.에 의해 수행된 메타분석 연구에서 liraglutide와 exenatide을 투약한 환자군과 다 른 당뇨병 치료제 또는 위약 투여군을 비교한 결과 역시 유의한 차이를 찾을 수 없었으며, liraglu- Fig. 2 Forest plot of the difference between liraglutide versus comparator
41 24.98 0.97 0 - -
4 1.14 0.77 0 0.308 0.547
Table 2 Test of heterogeneity and publication bias
Test of heterogeneity Publication bias No. of study
Q P value /2 P value (Begg’s) P value (Egger’s)
tide 투여군을 대상으로 한 하위그룹 분석(sub- group analysis)에서도 대조군과의 유의한 차이 가 없었다(OR=0.97; 95% Cl: 0.21–4.39).58) Monami M et al.의 메타분석 연구에서는 GLP-1 agonist 투여군 중 albiglutide 투여군에서만 유의 미한 급성 췌장염의 발생률 증가가 관찰되었고 lira- glutide 투여군은 다른 당뇨병 치료제나 위약 투여 군에 비해 발생률이 감소하였으나 통계적 유의성은 관 찰되지 않았다(OR=0.87; 95% Cl: 0.51–1.51).59) 따라서 두 연구는 liraglutide 투여와 급성 췌장염에 는 뚜렷한 연관성이 없다고 결론지었고 이는 본 연구 의 결과와도 일치한다.
본 연구에서 liraglutide 외에 췌장염 발생과 연관 된 비만, 담석, 알코올 남용 등의 위험 요인들을 배제 할 수가 없었고 liraglutide 투여군과 대조군 간 비 교에 포함된 환자 수가 총 1,502명으로 다소 적은 수 라는 한계점이 있었다. 한편, 오심이나 구역, 복통은 liraglutide의 흔한 부작용들이고 급성 췌장염의 일 부 증상과도 일치하기 때문에 췌장염을 정확하게 분 별해내고 진단하기 어려웠을 가능성도 배제할 수 없 다.60)
그럼에도 본 메타분석 연구를 통해 제2형 당뇨병 환 자에서 liraglutide 투여 시 급성 췌장염 발생 위험 이 비교적 낮은편이고 대조군과 비교했을 때 추가적 인 위험 증가는 없다는 것을 확인하였다. 이는 제2형 당뇨병 환자에서 liraglutide의 안전한 사용을 위한 근거로서 임상적 의의를 가질 것이다.
감사의 말씀
이 연구는 2020년 (재)동일문화장학재단 학술연구 비 지원에 의해 수행되었음.
참고문헌
1) The top 10 causes of death [Internet].
Who.int. [cited 2019 Jan 30]. Available from: https://www.who.int/en/news- room/fact-sheets/detail/the-top-10- causes-of-death
2) Kim BY, Won JC, Lee JH et al. Diabetes
fact sheets in korea, 2018: An appraisal of current status. Diabetes Metab J.
2019;43(4):487-94.
3) Nuffer WA, Trujillo JM. Liraglutide: A new option for the treatment of obesity.
Pharmacotherapy. 2015;35(10):926-34.
4) Bode B. An overview of the pharmacoki- netics, efficacy and safety of liraglu- tide. Diabetes Res Clin Pract. 2012;
97(1):27-42.
5) Dungan KM, Povedano ST, Forst T et al.
Once-weekly dulaglutide versus once- daily liraglutide in metformin-treated patients with type 2 diabetes (AWARD-6):
A randomised, open-label, phase 3, non-inferiority trial. Lancet. 2014;384 (9951):1349-57.
6) Butler PC, Elashoff M, Elashoff R et al.
A critical analysis of the clinical use of incretin-based therapies: Are the GLP-1 therapies safe? Diabetes Care. 2013;36 (7):2118-25.
7) Forsmark CE, Baillie J, AGA Institute Clinical Practice and Economics Com- mittee et al. AGA institute technical re- view on acute pancreatitis. Gastroen- terology. 2007;132(5):2022-44.
8) Russo MW, Wei JT, Thiny MT et al. Di- gestive and liver diseases statistics, 2004. Gastroenterology. 2004;126(5):
1448-53.
9) Huh JH, Jeon H, Park SM et al. Diabetes mellitus is associated with mortality in acute pancreatitis. J Clin Gastroenterol.
2018;52(2):178-83.
10) Li L, Shen J, Bala MM et al. Incretin treatment and risk of pancreatitis in patients with type 2 diabetes mellitus:
Systematic review and meta-analysis of randomised and non-randomised studies. BMJ. 2014;348:2366.
11) Garber A, Henry RR, Ratner R et al. Li- raglutide, a once-daily human gluca- gon-like peptide 1 analogue, provides sustained improvements in glycaemic control and weight for 2 years as mono- therapy compared with glimepiride in patients with type 2 diabetes. Diabetes Obes Metab. 2011;13(4):348-56.
12) Marso SP, Daniels GH, Brown-Frand- sen K et al. Liraglutide and cardiovas- cular outcomes in type 2 diabetes. N Engl J Med. 2016;375(4):311-22.
13) Jadad AR, Moore RA, Carroll D et al.
Assessing the quality of reports of ran- domized clinical trials: is blinding nec- essary?. Control Clin Trials. 1996;17 (1):1-12.
14) Lee J. Meta-analysis. Journal of Kore- an Endocrine Society. 2008;23(6):361- 78.
15) Cochran WG. The combination of esti- mates from different experiments. Bi- ometrics. 1954;10(1):101-9.
16) Begg CB, Mazumdar M. Operating characteristics of a rank correlation test for publication bias. Biometrics.
1994;50(4):1088-101.
17) Egger M, Smith GD, Schneider M et al.
Bias in meta-analysis detected by a simple, graphical test. BMJ 1997;315 (7109):629-34.
18) Vilsboll T, Zdravkovic M, Le-Thi T et al. Liraglutide, a long-acting human glucagon-like peptide-1 analog, given as monotherapy significantly improves glycemic control and lowers body weight without risk of hypoglycemia in patients with type 2 diabetes. Diabetes Care. 2007;30(6):1608-10.
19) Zinman B, Gerich J, Buse JB et al. Ef- ficacy and safety of the human gluca-
gon-like peptide-1 analog liraglutide in combination with metformin and thi- azolidinedione in patients with type 2 diabetes (LEAD-4 Met+TZD). Diabetes Care. 2009;32(7):1224-30.
20) Marre M, Shaw J, Brandle M et al. Li- raglutide, a once-daily human GLP-1 analogue, added to a sulphonylurea over 26 weeks produces greater im- provements in glycaemic and weight control compared with adding rosiglita- zone or placebo in subjects with type 2 diabetes (LEAD-1 SU). Diabet Med.
2009;26(3):268-78.
21) Nauck M, Frid A, Hermansen K et al.
Efficacy and safety comparison of lira- glutide, glimepiride, and placebo, all in combination with metformin, in type 2 diabetes: The LEAD (liraglutide effect and action in diabetes)-2 study. Diabe- tes Care. 2009;32(1):84-90.
22) Russell-Jones D, Vaag A, Schmitz O et al. Liraglutide vs insulin glargine and placebo in combination with metformin and sulfonylurea therapy in type 2 dia- betes mellitus (LEAD-5 met+SU): A randomised controlled trial. Diabetolo- gia. 2009;52(10):2046-55.
23) Buse JB, Rosenstock J, Sesti G et al.
Liraglutide once a day versus exenatide twice a day for type 2 diabetes: A 26- week randomised, parallel-group, mul- ti-national, open-label trial (LEAD-6).
Lancet. 2009;374(9683):39-47.
24) Kaku K, Rasmussen MF, Clauson P et al. Improved glycaemic control with minimal hypoglycaemia and no weight change with the once-daily human glucagon-like peptide-1 analogue lira- glutide as add-on to sulphonylurea in japanese patients with type 2 diabetes.
Diabetes Obes Metab. 2010;12(4):341- 7.
25) Pratley RE, Nauck M, Bailey T et al.
Liraglutide versus sitagliptin for pa- tients with type 2 diabetes who did not have adequate glycaemic control with metformin: A 26-week, randomised, parallel-group, open-label trial. Lan- cet. 2010;375(9724):1447-56.
26) Yang W, Chen L, Ji Q et al. Liraglutide provides similar glycaemic control as glimepiride (both in combination with metformin) and reduces body weight and systolic blood pressure in asian population with type 2 diabetes from china, south korea and india: A 16- week, randomized, double-blind, ac- tive control trial. Diabetes Obes Metab.
2011;13(1):81-8.
27) Buse JB, Nauck M, Forst T et al. Ex- enatide once weekly versus liraglutide once daily in patients with type 2 diabe- tes (DURATION-6): A randomised, open- label study. Lancet. 2013;381(9861):
117-24.
28) Hermansen K, Baekdal TA, During M et al. Liraglutide suppresses postprandial triglyceride and apolipoprotein B48 ele- vations after a fat-rich meal in patients with type 2 diabetes: A randomized, double-blind, placebo-controlled, cross- over trial. Diabetes Obes Metab. 2013;
15(11):1040-8.
29) Kapitza C, Forst T, Coester HV et al.
Pharmacodynamic characteristics of lixisenatide once daily versus liraglu- tide once daily in patients with type 2 diabetes insufficiently controlled on metformin. Diabetes Obes Metab. 2013;
15(7):642-9.
30) Charbonnel B, Steinberg H, Eymard E
et al. Efficacy and safety over 26 weeks of an oral treatment strategy including sitagliptin compared with an injectable treatment strategy with liraglutide in patients with type 2 diabetes mellitus inadequately controlled on metformin:
A randomised clinical trial. Diabetolo- gia. 2013;56(7):1503-11.
31) Dungan KM, Povedano ST, Forst T et al. Once-weekly dulaglutide versus once-daily liraglutide in metform- in-treated patients with type 2 diabetes (AWARD-6): A randomised, open-la- bel, phase 3, non-inferiority trial.
Lancet. 2014;384(9951):1349-57.
32) Pratley RE, Nauck MA, Barnett AH et al. Once-weekly albiglutide versus once-daily liraglutide in patients with type 2 diabetes inadequately controlled on oral drugs (HARMONY 7): A ran- domised, open-label, multicentre, non- inferiority phase 3 study. Lancet Dia- betes Endocrinol. 2014;2(4):289-97.
33) Mathieu C, Rodbard HW, Cariou B et al. A comparison of adding liraglutide versus a single daily dose of insulin as- part to insulin degludec in subjects with type 2 diabetes (BEGIN: VICTOZA ADD- ON). Diabetes Obes Metab. 2014;16 (7):636-44.
34) Retnakaran R, Kramer CK, Choi H et al. Liraglutide and the preservation of pancreatic beta-cell function in early type 2 diabetes: The LIBRA trial. Dia- betes Care. 2014;37(12):3270-8.
35) Nandy D, Johnson C, Basu R et al. The effect of liraglutide on endothelial function in patients with type 2 diabe- tes. Diab Vasc Dis Res. 2014;11(6):419- 30.
36) Ahmann A, Rodbard HW, Rosenstock J
et al. Efficacy and safety of liraglutide versus placebo added to basal insulin analogues (with or without metformin) in patients with type 2 diabetes: A ran- domized, placebo-controlled trial. Dia- betes Obes Metab. 2015;17(11):1056- 64.
37) Lind M, Hirsch IB, Tuomilehto J et al.
Liraglutide in people treated for type 2 diabetes with multiple daily insulin in- jections: Randomised clinical trial (MDI liraglutide trial). BMJ. 2015;351:h5364.
38) Odawara M, Miyagawa J, Iwamoto N et al. Once-weekly glucagon-like pep- tide-1 receptor agonist dulaglutide sig- nificantly decreases glycated haemo- globin compared with once-daily liraglutide in japanese patients with type 2 diabetes: 52 weeks of treatment in a randomized phase III study. Diabe- tes Obes Metab. 2016;18(3):249-57.
39) D’Alessio D, Haring HU, Charbonnel B et al. Comparison of insulin glargine and liraglutide added to oral agents in patients with poorly controlled type 2 diabetes. Diabetes Obes Metab. 2015;
17(2):170-8.
40) Davies MJ, Bergenstal R, Bode B et al.
Efficacy of liraglutide for weight loss among patients with type 2 diabetes:
The SCALE diabetes randomized clini- cal trial. JAMA. 2015;314(7):687-99.
41) Tanaka K, Saisho Y, Kawai T et al. Ef- ficacy and safety of liraglutide mono- therapy compared with metformin in japanese overweight/obese patients with type 2 diabetes. Endocr J. 2015;
62(5):399-409.
42) Kaku K, Kiyosue A, Ono Y et al. Lira- glutide is effective and well tolerated in combination with an oral antidia-
betic drug in japanese patients with type 2 diabetes: A randomized, 52- week, open-label, parallel-group trial.
J Diabetes Investig. 2016;7(1):76-84.
43) Azar ST, Echtay A, Wan Bebakar WM et al. Efficacy and safety of liraglutide compared to sulphonylurea during ramadan in patients with type 2 diabe- tes (LIRA-ramadan): A randomized tri- al. Diabetes Obes Metab. 2016;18(10):
1025-33.
44) Davies MJ, Bain SC, Atkin SL et al. Ef- ficacy and safety of liraglutide versus placebo as add-on to glucose-lowering therapy in patients with type 2 diabetes and moderate renal impairment (LI- RA-RENAL): A randomized clinical tri- al. Diabetes Care. 2016;39(2):222-30.
45) Nauck M, Rizzo M, Johnson A et al.
Once-daily liraglutide versus lix- isenatide as add-on to metformin in type 2 diabetes: A 26-week randomized controlled clinical trial. Diabetes Care.
2016;39(9):1501-9.
46) Nauck MA, Petrie JR, Sesti G et al. A phase 2, randomized, dose-finding study of the novel once-weekly human GLP-1 analog, semaglutide, compared with placebo and open-label liraglutide in patients with type 2 diabetes. Diabe- tes Care. 2016;39(2):231-41.
47) Seino Y, Kaneko S, Fukuda S et al.
Combination therapy with liraglutide and insulin in japanese patients with type 2 diabetes: A 36-week, rand- omized, double-blind, parallel-group trial. J Diabetes Investig. 2016;7(4):
565-73.
48) Vanderheiden A, Harrison L, Warshau- er J et al. Effect of adding liraglutide vs placebo to a high-dose lnsulin regimen
in patients with type 2 diabetes: A ran- domized clinical trial. JAMA Intern Med. 2016;176(7):939-47.
49) Zang L, Liu Y, Geng J et al. Efficacy and safety of liraglutide versus sitag- liptin, both in combination with met- formin, in chinese patients with type 2 diabetes: A 26-week, open-label, ran- domized, active comparator clinical trial. Diabetes Obes Metab. 2016;18(8):
803-11.
50) Bailey TS, Takacs R, Tinahones FJ et al. Efficacy and safety of switching from sitagliptin to liraglutide in sub- jects with type 2 diabetes (LIRA- SWITCH): A randomized, double-blind, double-dummy, active-controlled 26- week trial. Diabetes Obes Metab. 2016;
18(12):1191-8.
51) Idorn T, Knop FK, Jorgensen MB et al.
Safety and efficacy of liraglutide in pa- tients with type 2 diabetes and end- stage renal disease: An investigator- initiated, placebo-controlled, double- blind, parallel-group, randomized tri- al. Diabetes Care. 2016;39(2):206-13.
52) Kumarathurai P, Anholm C, Nielsen OW et al. Effects of the glucagon-like peptide-1 receptor agonist liraglutide on systolic function in patients with coronary artery disease and type 2 dia- betes: A randomized double-blind pla- cebo-controlled crossover study. Car- diovasc Diabetol. 2016;15(1):105.
53) Smits MM, Tonneijck L, Muskiet MH et al. Pancreatic effects of liraglutide or sitagliptin in overweight patients with type 2 diabetes: A 12-week randomized, placebo-controlled trial. Diabetes Care.
2017;40(3):301-8.
54) Bouchi R, Nakano Y, Fukuda T et al.
Reduction of visceral fat by liraglutide is associated with ameliorations of he- patic steatosis, albuminuria, and mi- cro-inflammation in type 2 diabetic pa- tients with insulin treatment: A randomized control trial. Endocr J.
2017;64(3):269-81.
55) Frias JP, Bastyr EJ, Vignati L et al.
The sustained effects of a dual GIP/
GLP-1 receptor agonist, NNC0090- 2746, in patients with type 2 diabetes.
Cell Metab. 2017;26(2):343-52.
56) Lingvay I, Desouza CV, Lalic KS et al. A 26-week randomized controlled trial of semaglutide once daily versus liraglu- tide and placebo in patients with type 2 diabetes suboptimally controlled on diet and exercise with or without metform- in. Diabetes Care. 2018;41(9): 1926-37.
57) Pratley R, Amod A, Hoff ST et al. Oral semaglutide versus subcutaneous lira- glutide and placebo in type 2 diabetes (PIONEER 4): A randomised, double- blind, phase 3a trial. Lancet. 2019;394 (10192):39-50.
58) Alves C, Batel-Marques F, Macedo AF et al. A meta-analysis of serious ad- verse events reported with exenatide and liraglutide: Acute pancreatitis and cancer. Diabetes Res Clin Pract. 2012;
98(2):271-84.
59) Monami M, Nreu B, Scatena A et al.
Safety issues with glucagon-like pep- tide-1 receptor agonists (pancreatitis, pancreatic cancer and cholelithiasis):
Data from randomized controlled tri- als. Diabetes Obes Metab. 2017;19(9):
1233-41.
60) Lankisch PG, Apte M, Banks PA et al.
Acute pancreatitis. Lancet. 2015;386 (9988):85-96.