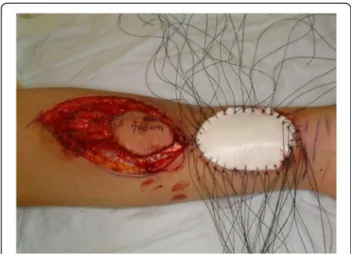
Double-layered collagen graft to the radial forearm free flap donor sites without skin graft
8
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
(8)
수치


+2

관련 문서
1 John Owen, Justification by Faith Alone, in The Works of John Owen, ed. John Bolt, trans. Scott Clark, "Do This and Live: Christ's Active Obedience as the
Purpose: This study was designed to evaluate the clinical characteristics and the treatment of colonoscopic perforation and the availability of
the Smart City Platform The City Integrated Operation Center.
Objective: The purpose of this study was to investigate the effect of clinical practice satisfaction on professional self-concept among dental hygiene students.. Methods:
From the results of this study, we concluded that two different sized graft materials have positive effects on new bone formation.. Additionally, smaller
success rates of dental implants placed at the time of or after alveolar ridge augmentation with an autogenous mandibular bone graft and titanium mesh: a 3-to
The purpose of this study was to investigate the lower extremity muscle strength and student health of male middle school students. Twenty middle school
The purpose of this study was to provide primary material in discussing methods to activate the treatment effects of diabetes and reduce the rate of
