212
Case Report
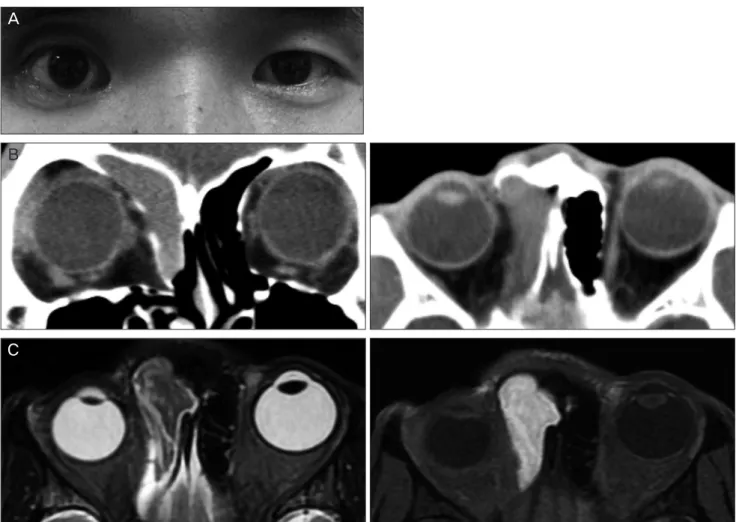
Frontoethmoidal Mucocele Presenting as Progressive Enophthalmos
Ji-Sun Paik
1, Su-Whan Kim 2, Suk-Woo Yang
1
1
Department of Ophthalmology and Visual Science, Seoul St. Mary’s Hospital, The Catholic University of Korea College of Medicine, Seoul, Korea
2