Effect of Diet on the Gut Microbiota Associated with Obesity
Bohkyung Kim
1, Ha-Neul Choi
2, Jung-Eun Yim
2,*
1
Department of Food Science and Nutrition, Pusan National University, Busan;
2Department of Food and Nutrition, Changwon National University, Changwon, Korea
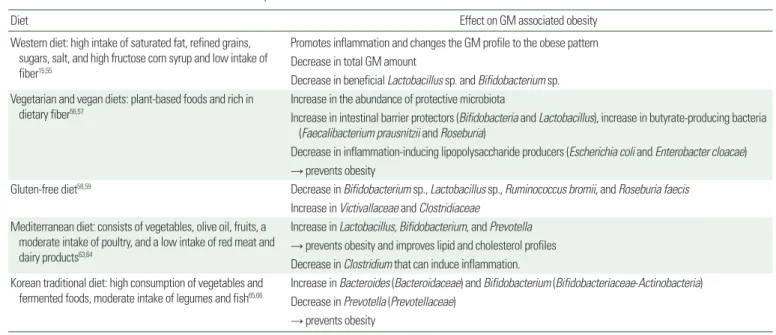
Obesity is abnormal or excessive fat accumulation that is associated with progression of metabolic diseases in- cluding type 2 diabetes mellitus, cardiovascular disease, nonalcoholic fatty liver disease, and cancer. Gut micro- biota (GM) have received much attention as essential factors in development and progression of obesity. The di- versity, composition, and metabolic activity of GM are closely associated with nutrient intake and dietary pat- tern. Scientific evidence supports the idea that dietary pattern directly changes the GM profile; therefore, diet is a crucial component related to interactions between GM and obesity progression. A literature review showed that dietary factors such as probiotics, prebiotics, fat, fatty acids, and fiber dramatically alter the GM profile relat- ed to obesity. Furthermore, different dietary patterns result in different GM composition and activity that can contribute to amelioration of obesity.
Key words: Diet, Prebiotics, Probiotics, Gastrointestinal microbiome, Obesity
Received July 31, 2019 Reviewed August 24, 2019 Accepted November 13, 2019
* Corresponding author Jung-Eun Yim
https://orcid.org/0000-0001-8344-1386 Department of Food and Nutrition, Changwon National University, 20 Changwondaehak-ro, Uichang-gu, Changwon 51140, Korea
Tel: +82-55-213-3517 Fax: +82-55-281-7480 E-mail: [email protected]
INTRODUCTION
Overweight and obesity have nearly tripled in the population since 1975. According to the World Health Organization (WHO), over 1.9 billion adults were considered overweight in 2014, repre- senting 39% of the world’s population. Over 340 million children and adolescents aged 5–19 years were also overweight or obese in 2016. Finkelstein et al.
1estimated an increase of 3.3 billion people with a body mass index (BMI) ≥ 25.0 kg/m
2, corresponding to 57.8% of the adults worldwide by 2030. Obesity is described as an accumulation of excessive fat mass concomitant with low-grade chronic systemic inflammation.
2Obesity has commonly been asso- ciated with development of other metabolic disorders such as type 2 diabetes mellitus (T2DM), cardiovascular disease (CVD), and some types of cancer.
3,4The gastrointestinal tract contains at least 10
14bacteria, with the most abundant numbers in the large intestine.
5The number of genes in the intestinal microbiome is 150- to 500-fold greater than in human DNA.
6The collected gut microbiota (GM) are described as a “forgotten organ” that is sensitive to dietary, environmental, and host factors with function complicatedly intertwined with host me- tabolism.
7Both endogenous and exogeneous factors such as auto- immune disease, chronic disease, medications, antibiotics, smoking, stress level, and diet affect the diversity and composition of GM.
Each individual has a unique GM composition and profile that may affect nutrient metabolism. Recent evidence has suggested that GM is a contributing factor in the progression of obesity.
6,8,9The GM is capable of modulating host metabolism through energy balance, chronic low-grade inflammation, and intestinal barrier function.
6Furthermore, the composition and diversity of GM are different
Copyright © 2019 Korean Society for the Study of Obesity
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
2017-03-16 https://crossmark-cdn.crossref.org/widget/v2.0/logos/CROSSMARK_Color_square.svg
Effect of Diet on the Gut Microbiota Associated with Obesity
Bohkyung Kim
1, Ha-Neul Choi
2, Jung-Eun Yim
2,*
1