티볼론과 에스트라디올 기반 호르몬 치료가 골밀도와 혈중 지질에 미치는 영향
인천광역시의료원 산부인과1, 서울대학교 의과대학 산부인과학교실2,
서울대학교병원 의생명연구원3, 서울대학교 의학연구원 인구의학연구소4
김 훈1․구승엽2,3,4․김석현2,3,4․최영민2,3,4․김정구2,3․문신용2,3,4
The Effect of Tibolone and Estradiol-based Hormone Therapy on Bone Mineral Density and Serum Lipid Profiles
Hoon Kim1, Seung-Yup Ku2,3,4, Seok Hyun Kim2,3,4, Young Min Choi2,3,4, Jung Gu Kim2,3, Shin Yong Moon2,3,4
1Department of Obstetrics and Gynecology, Incheon Medical Center, Incheon,
2Department of Obstetrics and Gynecology, Seoul National University College of Medicine, Seoul,
3Clinical Research Institute, Seoul National University Hospital, Seoul,
4Institute of Reproductive Medicine and Population, Medical Research Center, Seoul National University, Seoul, Korea
Objectives: To investigate the differences between the effect of tibolone and estradiol (E2)-based hormone therapy (HT) on bone mineral density (BMD) and serum lipid profiles in postmenopausal Korean women.
Materials and Methods: A retrospective study was conducted with 65 postmenopausal women receiving tibolone or E2-based hormone therapy in university hospital. BMD at lumbar spine (LS) and proximal femur was measured before and after 1 year of therapy and serum total cholesterol, triglyceride (TG) and high-density lipoprotein (HDL) was determined by enzymatic methods.
Results: BMD at LS increased after 1 year of tibolone (mean change: 3.0%) or E2-based HT (mean change:
1.6%), and the changes were significant (P=0.002 and 0.04, respectively). In E2 group, serum total cholesterol has decreased significantly after 1 year of therapy (P=0.02). Moreover, the change of HDL level was statistically significant in tibolone group compared to E2 group (P=0.01). The changes of levels of total cholesterol, TG and HDL has demonstrated negative relationship of BMD changes at femur neck and trochanter in tibolone group, whereas only the HDL changes were significantly related to the change of trochanter BMD in E2 group.
Conclusions: Both tibolone and E2-based hormone therapy increased BMD at lumbar spine. The changes of serum lipid levels may be associated with the BMD changes in both groups although the relationships were different according to the regimen.
Key Words: Bone mineral density, Estradiol, Hormone therapy, Lipid, Tibolone
Received: March 19, 2012 Revised: March 20, 2012 Accepted: March 26, 2012
Corresponding Author: Seung-Yup Ku, Department of Obstetrics and Gynecology, Seoul National University College of Medicine, 28 Yeongeon-dong, Jongno-gu, Seoul 110-744, Korea
Tel: +82-2-2072-1971, Fax: +82-2-762-3599, E-mail: [email protected]
* 이 논문은 2012년도 서울대학교 의과대학 교육연구재단의 지원에 의하여 연구되었음.
선진국이 당면한 공통된 문제 중 하나는 고령화 사회로의 이행이다. 한국 역시 예외는 아니어서 고 령화 사회로 급격히 진행하고 있고 2030년이 되면 전체 여성 중 45세 이상이 62%에 달할 것으로 전망 되고 있다.1 이는 곧 폐경 여성들의 건강 문제가 사 회적으로도 매우 중요한 문제가 될 것임을 의미하는 데, 난소의 기능 상실로 인한 폐경은 열성 홍조와 같 은 혈관운동증상뿐만 아니라 심혈관질환, 골다공증 등의 만성 합병증을 초래할 수 있다. 따라서 이와 같 은 질환을 예방하기 위해 호르몬 치료가 효과적인지 에 대한 Women’s Health Initiative 연구가 진행되었 으나 유방암과 관련된 문제점이 과다하게 평가되면 서 조기 종료되었다.2 WHI 연구에는 접합마에스트 로겐(conjugated equine estrogen, CEE)이 사용되었는 데, CEE는 임신한 암말의 소변에서 추출한 에스트 로겐으로 약 10여 종에 달하는 다양한 종류의 에스 트로겐 연관 화합물의 조합이다. 이외에도 폐경 여 성의 증상 치료를 위해서 사용되는 제제에는 에스트 라디올(estradiol)을 기반으로 한 제제들이 있으며 티 볼론(tibolone) 역시 효과적으로 사용되는 약물이다.
에스트라디올은 폐경 전 여성에서는 난소에서, 폐 경 여성에서는 말초 조직에서 안드로겐(androgen)의 방향화(aromatization)를 통해 생성되는 가장 강력한 생리적 에스트로겐으로3 주로 estradiol valerate, estra- diol hemihydrate의 형태로 제조된다.4 에스트라디올 은 다양한 용량에서 골소실을 방지한다고 보고되었 으며5,6 치료를 중단하면 CEE와 마찬가지로 골밀도 유지 효과는 사라진다.6
티볼론(tibolone)도 역시 폐경 증상의 치료와 골다 공증의 예방을 위해 사용되는 약물로7 골조직에서 에스트로겐 수용체에 결합하여8 골소실을 예방하고 골밀도를 증가시킨다.9-12 최근 보고된 LIFT 연구에 서는 위약군에 비해 척추 골절은 45%, 비척추 골절 은 26% 감소되었다고 보고하였다.7 그러나, 티볼론 은 혈중 지질에 미치는 영향이 다른 에스트로겐 제 제와는 다르게 나타나는데, 총콜레스테롤과 중성지 방을 감소시키지만 HDL 역시 감소시키는 결과가 보 고된 바 있다.10,13
한편 혈중 지질 농도는 골밀도와 관련이 있다고 보고되어 왔는데, 중성 지방(triglyceride, TG)은 골밀
도와 양의 상관관계가 있다고 보고되었고14,15 고지혈 증을 치료하기 위한 약제인 스타틴(statin) 사용이 골 절의 감소와 관련이 있다는 보고도 있어16,17 혈중 지 질 농도의 변화는 골밀도의 변화와 관련이 있을 가 능성이 있다. 티볼론과 에스트라디올을 사용하는 호 르몬 치료는 혈중 지질에 미치는 영향이 다르므로 골밀도에 미치는 영향이 다르게 나타날 수 있으나, 최근까지 보고된 국내 연구들은 대부분 티볼론과 CEE를 비교하거나18,19 또는 CEE와 에스트라디올을 구분하지 않고 비교한 바 있다.20
본 연구에서는 서울대병원 폐경클리닉을 방문한 여성 중 티볼론 또는 에스트라디올을 사용하는 호르 몬 치료를 시행한 여성을 대상으로 후향적으로 혈중 지질과 골밀도에 미치는 영향과 두 지표 변화 사이 의 관련성을 비교하고자 하였다.
대상 및 방법
1. 연구 대상
서울대학교병원의 폐경 클리닉을 방문한 폐경 여 성 중 티볼론(LivialⓇ, Merck, Whitehouse Station, NJ, USA), 혹은 에스트라디올을 기반으로 하는 호르몬 치료(ClimenⓇ, Bayer Schering Pharma, Seoul, Korea;
AngeliqⓇ, Bayer Schering Pharma; FemostonⓇ, Choong- wae Pharmaceutical, Seoul, Korea)를 1년 이상 시행한 여성 65명을 대상으로 하였다. 폐경은 자궁절제술 혹은 양측 난소절제술의 과거력 없이 마지막 생리 후 적어도 1년이 경과된 여성으로 연구대상자 중 고 지혈증, 당뇨병, 간질환, 신장질환 등 급 ․ 만성질환이 있거나 이전에 골대사(bone metabolism)에 영향을 줄 수 있는 약물인 에스트로겐, 비스포스포네이트, 스 타틴 등을 복용한 병력이 있는 여성은 제외하였다.
2. 골밀도 측정
척추, 근위 대퇴부의 골밀도는 호르몬 치료 전과 치료 후 1년 시점에 측정하였으며 측정에 Lunar사 (Lunar PPX-L, Medison, Wisconsin, USA)의 이중에너 지 엑스레이 흡수계측기(dual energy X-ray absop- tiometry; DXA)를 이용하였다. 이 측정기의 골밀도 측정에서의 체내 변이계수(in vivo coefficient of
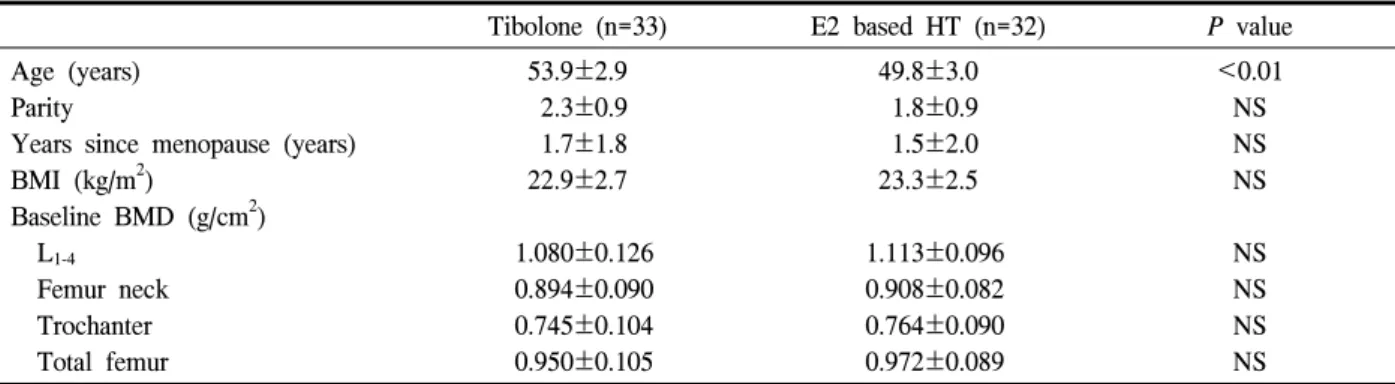
Table 1. Clinical characteristics of study population
Tibolone (n=33) E2 based HT (n=32) P value Age (years)
Parity
Years since menopause (years) BMI (kg/m2)
Baseline BMD (g/cm2) L1-4
Femur neck Trochanter Total femur
53.9±2.9 2.3±0.9 1.7±1.8 22.9±2.7
1.080±0.126 0.894±0.090 0.745±0.104 0.950±0.105
49.8±3.0 1.8±0.9 1.5±2.0 23.3±2.5
1.113±0.096 0.908±0.082 0.764±0.090 0.972±0.089
<0.01 NS NS NS
NS NS NS NS E2, estradiol; HT, hormone therapy; BMI, body mass index; BMD, bone mineral density
Data are presented as Mean±SD.
P value by Student’s t-test.
Fig. 1. 1-Yr change of BMD after tibolone and E2 based hormone therapy (HT)
variation)는 요추 1.4%, 대퇴골경부 2.1%, Ward 삼각 주 2.1%, 대퇴돌기 1.1%이었다.
3. 혈중 지질의 측정
혈중 지질 역시 호르몬 치료 전과 치료 후 1년 시 점에 측정하였으며 효소법(enzymatic method)을 이용 하여 Hitachi 7600 automatic analyzer (Hitachi Instru- ments Inc., Tokyo, Japan)에서 측정하였고 사용한 키 트는 총콜레스테롤은 T-Cho reagent (신양화학약품, 서울), TG는 AceChem TG kit (영동제약, 서울), HDL 은 Determiner-L HDL-C kit (Kyowa Kirin, Tokyo, Japan)을 사용하였다.
4. 통계분석
모든 통계 계산은 SPSS 12.0 통계 프로그램(SPSS inc., Chicago, Illinois)을 사용하였다. 티볼론 군과 에 스트라디올 군 간 환자군의 특성 및 기저 골밀도 비 교에는 Student’s t-test를 이용하였고, 치료 1년 경과 후 골밀도의 변화 정도는 paired t-test, 양 군간 비교 는 연령, 폐경 후 기간, 체질량지수를 보정하여 공분 산분석(analysis of covariance)을 이용하여 분석하였 다. 그리고 치료 전후 혈중 지질의 변화는 연령, 폐 경 후 기간, 체질량지수를 고려하여 반복공분산분석 (repeated measures analysis of covariance)을 사용하였 고, 혈중 지질의 변화와 골밀도의 변화 사이의 관련 성 분석을 위해서는 편상관분석(partial correlation analysis)을 시행하였다. 모든 통계학적 분석에서 P<
0.05인 경우만 유의하게 판정하였다.
결 과
본 연구에서 티볼론 및 에스트라디올 호르몬 치료 를 시행하고 1년 후 골밀도와 혈중 지질을 측정한 폐경 환자는 각각 33명, 32명이었다. 연령은 티볼론 군에서 평균 연령이 53.9세로 에스트라디올 군(평균 연령 49.8세)에 비해서 의미있게 높았으나(P<0.01) 출산 자녀의 수, 폐경 후 기간, 체질량 지수에는 차 이가 없었고, 기저 골밀도 역시 두 군 사이에 통계적 으로 의미있는 차이는 보이지 않았다(Table 1).
호르몬 치료 1년 경과 시점에서의 골밀도는 티볼 론 군에서 요추 골밀도가 3.0% 증가하였으며 에스
Table 2. 1-Yr change of serum lipid profiles after tibolone and E2 based hormone therapy Tibolone (n=33) E2 based HT (n=32)
Baseline After 1 yr P value Baseline After 1 yr P value P value*
Total cholesterol (mg/dL) 187.2±8.1 165.2±9.1 NS 196.4±7.5 186.2±8.4 0.02 NS Triglyceride (mg/dL) 117.9±17.5 91.5±14.4 NS 85.2±16.0 103.9±13.1 NS NS High-density lipoprotein (mg/dL) 54.7±3.8 47.9±4.1 NS 67.5±3.7 65.2±4.0 NS 0.01 E2, estradiol; HT, hormone therapy
Data are presented as mean±SE adjusting for age, years since menopause, body mass indexand baseline lipid profiles.
P value by paired t-test
P* value by RMANCOVA between tibolone and E2 based HT.
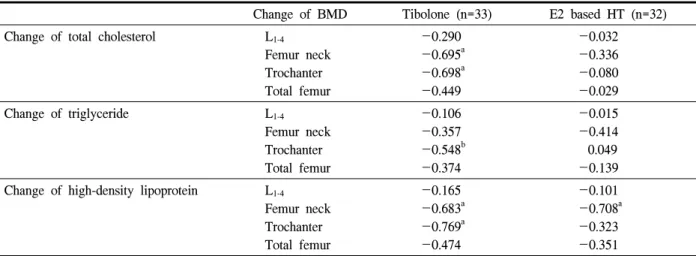
Table 3. Association between 1-yr change of bone mineral density (BMD) and 1-yr change of serum lipid profiles
Change of BMD Tibolone (n=33) E2 based HT (n=32) Change of total cholesterol L1-4
Femur neck Trochanter Total femur
-0.290 -0.695a -0.698a -0.449
-0.032 -0.336 -0.080 -0.029
Change of triglyceride L1-4
Femur neck Trochanter Total femur
-0.106 -0.357 -0.548b -0.374
-0.015 -0.414 0.049 -0.139 Change of high-density lipoprotein L1-4
Femur neck Trochanter Total femur
-0.165 -0.683a -0.769a -0.474
-0.101 -0.708a -0.323 -0.351 E2, estradiol; HT, hormone therapy
Data are presented as partial correlation coefficient.
P value by partial correlation analysis adjusting for age, years since menopause and body mass index.
a: P<0.01, b: P<0.05
트라디올 군은 1.6% 증가하여 양 군 모두 기저 요추 골밀도에 비해 유의한 증가율을 보였으나(P=0.002 and 0.04) 두 군 사이에 증가율의 차이는 없었다 (Fig. 1). 근위 대퇴부의 골밀도는 기저 골밀도에 비 해서 양 군 모두에서 차이가 없었고, 에스트라디올 군에서는 골밀도가 증가하는 양상이 관찰되었으나 통계적으로 의미는 없었고 또한 티볼론 군에 비해 유의한 차이는 관찰되지 않았다.
혈중 총 콜레스테롤은 에스트라디올 군에서 호르 몬 치료 후 의미있게 감소하였으나(P=0.02) 중성 지 방 및 고밀도 지단백의 혈중 농도는 차이가 없었다 (Table 2). 티볼론 군에서는 고밀도 지단백 농도가 54.7 mg/dL에서 47.9 mg/dL로 감소하여 에스트라디
올 군에 비해 의미있는 차이가 있었다(P=0.01).
혈중 지질의 변화와 골밀도 변화 사이의 관련성에 대해서 분석하였을 때 티볼론 군에서 대퇴돌기 (trochanter)의 골밀도 변화는 혈중 총콜레스테롤, 중 성 지방, 고밀도 지단백 변화와 유의한 음의 상관관 계가 관찰되었고, 대퇴 경부(femur neck) 골밀도 변 화는 중성 지방을 제외한 총콜레스테롤, 고밀도 지 단백 변화와 연관성이 있었다(Table 3). 에스트라디 올 군은 고밀도 지단백 변화만 대퇴 경부의 골밀도 변화와 음의 상관관계가 관찰되었으며 다른 부위에 서는 유의한 결과를 보이지 않았다.
고 찰
폐경 후 골소실의 가장 중요한 원인은 에스트로겐 의 결핍으로 에스트로겐은 조골세포(osteoblast)와 파 골세포(osteoclast) 활동의 균형을 맞추어 골소실을 방지하는 역할을 한다. 폐경 여성에서 다양한 목적 으로 사용하는 호르몬 치료는 골소실을 막고 골절을 방지할 수 있어2 골다공증의 예방 및 치료를 위해 사용하고 있으나 치료를 중단하게 되면 골밀도 유지 효과는 사라진다.21
티볼론은 구조적으로는 19-nortestosterone과 유사 하며 대사 과정을 거쳐 에스트로겐 작용제로 작용하 는 3α-수산화물(hydroxy metabolite), 3β-수산화물 (hydroxy metabolite), 프로게스토겐과 안드로겐의 성 격을 갖는 ∆-4 ketoisomer의 3가지 대사산물을 생성 한다. 이 대사산물이 조직마다 각각 다르게 작용하 는 STEAR (selective tissue estrogenic acitivity regu- lator)로22 자궁내막의 경우 ∆-4 ketoisomer가 주로 만 들어져 자궁내막 증식을 억제하는 방향으로 작용하
게 되며23,24 골조직에서는 에스트로겐과 유사하게 골
소실을 예방하고 골밀도를 증가시킨다.9-12
본 연구에서는 티볼론과 에스트라디올 호르몬 치 료를 시행하였을 때 두 군 모두에서 기저 골밀도에 비해 요추 골밀도의 의미 있는 증가가 관찰되었으며 제제에 따른 골밀도의 변화 정도에는 차이가 없었 다. 본 연구에서는 골밀도가 요추골에서만 의미 있 게 증가한 것은 폐경 여성에서의 에스트로겐 감소에 의해 특히 척추 골밀도가 먼저 감소하는 양상을 보 이는데25 치료 기간이 상대적으로 단기간이었기 때 문에 감소된 척추 골밀도가 먼저 증가하면서 본 연 구와 같은 현상을 보였을 가능성이 있다. 또한 대퇴 근위부 골밀도는 차이를 보이지 않았는데, Long- Term Intervention on Fractures with Tibolone (LIFT) 연구에서는 요추의 골밀도 증가에 비해 대퇴 근위부 의 골밀도 변화는 상대적으로 적었다고 보고한 바 있어,7 본 연구와 같은 1년의 단기간 치료에는 통계 적으로 의미있는 결과를 보이지 못했을 가능성이 있 다. Yang19은 CEE와의 비교 연구에서 1년 시점에서 두 군 모두 요추 골밀도가 증가하였으나 대퇴골 경 부의 골밀도에는 차이가 없었다고 하여 본 연구와
유사한 결과를 보고한 바 있는데, 치료를 2년 이상 지속하였던 연구에서는6,12 골밀도는 계속 증가 양상 을 보였던 바 만약 수년 동안 치료를 시행하고 후속 골밀도 측정 결과를 포함하여 분석한다면 대퇴 근위 부의 골밀도 역시 의미 있는 결과를 보였을 가능성 이 있다. 티볼론 군에서는 통계적으로 의미는 없으 나 대퇴 근위부의 골밀도가 감소하는 양상을 보였는 데, 이는 단기간 치료할 때에는 오히려 골밀도가 감 소하는 것처럼 보이나 2년 이상 치료를 지속할 때 골밀도가 증가하게 되는 평균 회귀 현상(regression to the mean)일 가능성이 있어26 최소한 2년 이상 치 료하면서 골밀도를 추적 관찰하여야 정확한 결과를 얻을 수 있을 것으로 보인다.
1년간 치료를 시행한 후 본 연구에서는 에스트라 디올 군에서 총 콜레스테롤이 의미 있는 감소를 보 였으며, 티볼론 군에서는 혈중 지질의 유의한 변화 가 없었으나 에스트라디올 군과 비교하였을 때에는 HDL이 감소하는 양상이 관찰되었다. 티볼론을 사용 하였을 때 HDL이 감소하는 것에 대해서는 여러 연 구에서 보고된 바 있는데10,13 LDL (low-density lipo- protein)의 산화를 방지하는 역할을 하는 HDL은 심 혈관 질환의 예방인자이므로 HDL의 감소는 심혈관 질환을 증가시킬 가능성이 있다. 그러나, 티볼론 사 용시 HDL의 감소는 LDL의 증가를 동반하지는 않으 며,27 본 연구에서도 Friedewald equation28을 이용한 LDL 농도는 차이를 보이지 않았다. 또한 Osteopo- rosis Prevention and Arterial effects of tiboLone (OPAL) study29에서는 티볼론과 CEE 모두 경동맥의 intima-media thickness를 증가시키고 그 정도에는 차 이가 없다고 보고하여 HDL 감소로 인한 심혈관 질 환의 위험도가 에스트로겐 치료에 비해 더 높지 않 을 것으로 보인다.
한편 고지혈증을 치료하기 위한 약제인 스타틴 (statin) 사용이 골절의 감소와 관련이 있다는 보고16,17 이후 혈중 지질 농도는 골밀도와 관련이 있을 가능 성이 있어 여러 연구가 보고되어 왔는데, 중성 지방 (triglyceride, TG)은 골밀도와 양의 상관관계가 있고, HDL은 음의 상관관계가 보고된 바 있다.14,15 본 연 구에서는 혈중 지질 농도의 감소는 골밀도의 증가와 관련이 있었으며, 특히 이와 같은 양상은 티볼론 군
에서 뚜렷하게 나타나 대퇴돌기 및 경부의 골밀도 변화가 혈중 총콜레스테롤, 고밀도 지단백 변화와 유의한 음의 상관관계가 관찰되었다. 에스트라디올 군에서는 다른 양상을 보이고 있어 혈중 지질 변화 가 골밀도에 미치는 기전이 두 군 간에 다를 가능성 이 있다.
국내에서도 티볼론의 골밀도와 지질에 미치는 영 향에 관한 보고가 있었는데, Park et al.30은 치료 1년 시점에서 평균 요추 골밀도가 6.6% 증가하였다고 하였고, Yang19은 CEE와의 비교 연구에서 요추 골밀 도의 증가를 보고하였으며 티볼론 군에서의 HDL 감 소를 보고하였다. 그러나 현재까지 국내에서의 보고 는 CEE 군과 비교하거나18,19 혹은 CEE와 에스트라 디올을 모두 합쳐서 비교한 연구였으며20 에스트라 디올 군과 비교한 보고는 현재까지 없었고, 티볼론 에 의한 지질의 변화와 골밀도 변화와의 관련성에 대해서는 본 연구가 첫 보고이다.
본 연구에는 몇 가지 제한점이 있는데, 첫째 폐경 클리닉을 방문한 여성을 대상으로 한 소규모 연구이 므로 선택 비뚤림(selection bias)의 가능성이 있다. 또 한 비교적 단기간에 걸친 연구였기 때문에 유의한 결과를 도출하지 못하였을 가능성이 있으며 에스트 라디올 군의 경우 투여한 에스트라디올의 종류가 estradiol valerate과 estradiol hemihydrate 2가지였으며 그 용량이 1~2 mg으로 다양하였다는 문제점이 있 다. 또한 자궁내막 보호를 위해 병합 투여한 프로게 스토겐에 의해서도 골밀도에 영향을 미칠 가능성이 있다. 마지막으로 골밀도에 크게 영향을 미치는 연 령, 폐경 후 기간, 체질량 지수 등은 보정을 하였으 나 또 다른 영향 인자인 흡연, 음주, 운동, 칼슘 섭취 량 등에 대해서는 조사하지 않아 보정할 수 없었다 는 문제점이 있다.
결론적으로 한국 폐경 여성에서 티볼론과 에스트 라디올 호르몬 치료는 요추 골밀도를 증가시켰으며 대퇴 근위부 골밀도의 변화는 혈중 지질 농도의 변 화와 연관성이 있었으나 제제에 따른 차이가 관찰되 었다. 상술한 제한점을 고려하여 향후 더 많은 여성 을 대상으로 한 비교 연구가 필요할 것으로 사료된 다.
Conflict of interest statement: None 참 고 문 헌
1. Korean National Statistical Office. Statistics on the aged. 2006.
2. Rossouw JE, Anderson GL, Prentice RL, LaCroix AZ, Kooperberg C, Stefanick ML, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results From the Women's Health Initiative randomized controlled trial. JAMA 2002;288:321-33.
3. Wood CE, Clarkson TB, Chen H, Veenstra TD, Xu X, Scott L, et al. Comparative effects of oral conjugated equine estrogens and micronized 17beta- estradiol on breast proliferation: a retrospective analysis. Menopause 2008;15:890-8.
4. Sneader W. The discovery of oestrogenic hormones.
Menopause Int 2000;6:129-33.
5. Gräser T, Römer T, Wiedey KD, Janaud A.
Climodien (estradiol valerate 2 mg plus dienogest 2 mg) is safe and effective in the treatment of postmenopausal complaints. Climacteric 2001;4:
332-42.
6. Heikkinen J, Vaheri R, Haapalahti J, Timonen U.
A 10-year follow-up of the effect of continuous- combined hormone replacement therapy and its discontinuation on bone in postmenopausal women.
Menopause Int 2008;14:70-7.
7. Cummings SR, Ettinger B, Delmas PD, Kenemans P, Stathopoulos V, Verweij P, et al. The effects of tibolone in older postmenopausal women. N Engl J Med 2008;359:697-708.
8. Ederveen AG, Kloosterboer HJ. Tibolone exerts its protective effect on trabecular bone loss through the estrogen receptor. J Bone Miner Res 2001;16:
1651-7.
9. Berning B, Kuijk CV, Kuiper JW, Bennink HJ, Kicovic PM, Fauser BC. Effects of two doses of tibolone on trabecular and cortical bone loss in
early postmenopausal women: a two-year rando- mized, placebo-controlled study. Bone 1996;19:
395-9.
10. Gallagher JC, Baylink DJ, Freeman R, McClung M. Prevention of bone loss with tibolone in post- menopausal women: results of two randomized, double-blind, placebo-controlled, dose-finding studies.
J Clin Endocrinol Metab 2001;86:4717-26.
11. Lippuner K, Haenggi W, Birkhaeuser MH, Casez JP, Jaeger P. Prevention of postmenopausal bone loss using tibolone or conventional peroral or transdermal hormone replacement therapy with 17beta-estradiol and dydrogesterone. J Bone Miner Res 1997;12:806-12.
12. Rymer J, Robinson J, Fogelman I. Effects of 8 years of treatment with tibolone 2.5 mg daily on postmenopausal bone loss. Osteoporos Int 2001;12:
478-83.
13. Castelo-Branco C, Vicente JJ, Figueras F, Sanjuan A, Martínez de Osaba MJ, Casals E, et al.
Comparative effects of estrogens plus androgens and tibolone on bone, lipid pattern and sexuality in postmenopausal women. Maturitas 2000;34:161-8.
14. Adami S, Braga V, Zamboni M, Gatti D, Rossini M, Bakri J, et al. Relationship between lipids and bone mass in 2 cohorts of healthy women and men. Calcif Tissue Int 2004;74:136-42.
15. Cui LH, Shin MH, Chung EK, Lee YH, Kweon SS, Park KS, et al. Association between bone mineral densities and serum lipid profiles of pre- and post-menopausal rural women in South Korea.
Osteoporos Int 2005;16:1975-81.
16. Meier CR, Schlienger RG, Kraenzlin ME, Schlegel B, Jick H. Statin drugs and the risk of fracture.
JAMA 2000;284:1921-2.
17. Wang PS, Solomon DH, Mogun H, Avorn J.
HMG-CoA reductase inhibitors and the risk of hip fractures in elderly patients. JAMA 2000;283:
3211-6.
18. Park JW, Song EH, Lee WK. A Comparative
Study of Continuous Combined Hormone Replace- ment Therapy and Tibolone on Lipid Metabolism in Postmenopausal Women. Korean J Obstet Gynecol 2002;45:678-81.
19. Yang SH. Effects of tibolone on postmenopausal osteoporosis, lipid, mammograph compared with continuous combined hormone replacement therapy.
J Korean Acad Fam Med 2001;22:904-14.
20. Namkung J, Kim JH, Jo HH, Oh EK, Cheon K, Kwon DJ, et al. Comparison of the Effects of Hormone Replacement Therapy on Bone Mineral Density, Lipid Profiles, and Biochemical Markers of Bone Metabolism. J Korean Soc Menopause 2010;16:107-15.
21. Heiss G, Wallace R, Anderson GL, Aragaki A, Beresford SA, Brzyski R, et al. Health risks and benefits 3 years after stopping randomized treat- ment with estrogen and progestin. JAMA 2008;299:
1036-45.
22. Kloosterboer HJ. Tibolone: a steroid with a tissue- specific mode of action. J Steroid Biochem Mol Biol 2001;76:231-8.
23. Archer DF, Hendrix S, Gallagher JC, Rymer J, Skouby S, Ferenczy A, et al. Endometrial effects of tibolone. J Clin Endocrinol Metab 2007;92:911-8.
24. Markiewicz L, Gurpide E. In vitro evaluation of estrogenic, estrogen antagonistic and progestagenic effects of a steroidal drug (Org OD-14) and its metabolites on human endometrium. J Steroid Biochem 1990;35:535-41.
25. Johnston CC Jr, Hui SL, Witt RM, Appledorn R, Baker RS, Longcope C. Early menopausal changes in bone mass and sex steroids. J Clin Endocrinol Metab 1985;61:905-11.
26. Cummings SR, Palermo L, Browner W, Marcus R, Wallace R, Pearson J, et al. Monitoring osteoporo- sis therapy with bone densitometry: misleading changes and regression to the mean. Fracture Inter- vention Trial Research Group. JAMA 2000;283:
1318-21.
27. von Eckardstein A, Nofer JR, Assmann G. High density lipoproteins and arteriosclerosis. Role of cholesterol efflux and reverse cholesterol transport.
Arterioscler Thromb Vasc Biol 2001;21:13-27.
28. Friedewald WT, Levy RI, Fredrickson DS. Estima- tion of the concentration of low-density lipoprotein cholesterol in plasma, without use of the prepara- tive ultracentrifuge. Clin Chem 1972;18:499-502.
29. Bots ML, Evans GW, Riley W, McBride KH, Paskett ED, Helmond FA, et al. The effect of
tibolone and continuous combined conjugated equine oestrogens plus medroxyprogesterone acetate on progression of carotid intima-media thickness: the Osteoporosis Prevention and Arterial effects of tiboLone (OPAL) study. Eur Heart J 2006;27:746- 55.
30. Park JW, Shin GC, Hur EJ. The Effect of Tibolone on Bone Mineral Density in Postmenopausal Women with Osteopenia or Osteoporosis. Korean J Obstet Gynecol 1999;42:1324-7.