책임저자:김경식, 고양시 덕양구 화수로 14번길 55
412-270, 명지병원 성형외과 Tel: 031-810-6830, Fax: 031-810-6837 E-mail: [email protected]
화상치료에서 동종유래배양세포이식과 젖산 융합체 합성창상치료제 적용의 비교
김대현ㆍ김경식ㆍ최 준ㆍ김승홍
명지병원 성형외과Comparison of Cultured Keratinocyte Allograft versus Alloplastic Material in Management of Burn Injury
Dae-Hyun Kim, M.D., Kyung-Sik Kim, M.D., Ph.D., Jun Choi, M.D., Ph.D. and Seung-Hong Kim, M.D., Ph.D.
Department of Plastic & Reconstructive Surgery, Myong-Ji Hospital, Goyang, Korea
Purpose: In the past days, the majority of 2nd degree burns
were treated conservatively, and deep 2nd degree burns were usually covered by skin grafts. However, conservative treatment spends a long time in complete healing and ac- companies severe pain and discomfort. Additionally, cover- ing the wound with skin graft causes recipient site scarring and donor site morbidity. Since keratinocyte graft was in- troduced, nowadays it is widely used in burn wound. These treatment methods are proved to be clinically successful by many clinical and experimental studies. However, there are several disadvantages such as inconvenient using methods and limited usage in several cases. For that reason, at 2004, alloplastic material was first introduced to come over these problems of keratinocyte graft. There had been no precious reports comparing theses two methods, so we planned to fo- cus on differences of two methods in our institute.Methods: From March 2013 to september 2014, among the
47 patients with burn wound (2nd degree - partial 3rd degree) underwent biologic dressing with cultured keratinocyte allog- raft (Kaloderm® (Tegoscience, Korea)) alloplastic material (Suprathel® (Polymedics Innovations GmbH, Germany). The outcomes were assessed using time for epithelization, TBSA (%), Vancouver Scar Scale and complication.Results: All burn wounds were completely epithelized without
any complication. The average time for epithelization was 13.4/13.4 days.Conclusion: The result of this study suggests that Kaloderm
® and Suprathel® did not show significant difference. Therefore, Suprathel® may be considered as an alternative choice fortreating 2nd and 3rd degree burns in some clinical settings.
(J Korean Burn Soc 2014;17:73-80) Key Words: Burn, Keratinocyte, Suprathel
®서 론
화상환자의 치료방법의 결정에 있어 과거에는 그 깊이에 따라 1도 화상 및 표재성 2도 화상에는 주로 보존적 화상처 치를 선택하였으며 심재성 2도 화상 이상의 깊이에서는 피 부이식술 및 피판술을 선택하였다.
하지만 보존적 화상처치의 경우 치유까지의 기간이 길고 통증 등으로 인한 환자들의 치료 순응도가 떨어지는 등의 단점이 있으며 피부이식술 및 피판술의 경우 치료후의 비 후성 반흔, 구축, 공여부 합병증 등의 단점이 있다.
따라서 화상 환자의 치료방법의 결정에 있어 환자들의 치료 과정 순응도를 높이고 이를 통하여 치료 후 남을 수 있는 비후성 반흔, 구축, 색소침착, 공여부 합병증 등의 최 소화가 중요한 고려요소라고 할 수 있겠다.
1975년 동종 유래 배양피부 이식(cultured keratinocyte allograft)이 소개된 이후
1)환자 본인 또는 보호자가 수술적 처치를 원하지 않는 경우, 수술 후 협조가 되지 않을 것으로 판단되는 심재성 2도 화상 및 부분 3도 화상 환자에 있어 널리 적용되어지고 있다.
하지만 안면부, 소아환자, 관절부의 화상환자 등의 경우 에 동종유래 배양피부 이식(cultured keratinocyte allograft (Kaloderm
®(Tegoscience, Korea)), 이하 Kaloderm) (Fig. 1) 의 적용이 부착 및 고정의 문제 그리고 보관(냉동보관 및 보유기간의 제한)상의 이유로 제한점이 있다
9).
젖산 융합체 합성창상치료제((synthetic film made of
Lacto-Capromer and Polylactic Acid, Suprathel
®(Poly-
medics Innovations GmbH, Germany), 이하 Suprathel)
8)(Fig. 2)은 2004년 소개된 후 화상창상에 적용 시 생체에 재
흡수 되는 특성으로 안면부, 소아, 관절부의 화상 환자 등
Kaloderm의 사용에 제한이 있는 경우 적용이 용이하며 실
온에서 3년간 보관이 가능한 것으로 보고되고 있다.
Fig. 1. Cultured keratinocyte allo-
gaft (Kaloderm® (Tegoscience, Korea) 3.5×3.5 cm sized).Fig. 2. Synthetic film made of
Lacto-Capromer and Polylactic Acid, Suprathel® (Polymedics Innovations GmbH, Germany 5×5 cm sized).이용하여 치료하였으며 현재까지 동종유래 배양세포이식 과 젖산 융합체 합성창상치료제 적용 시 효과에 대한 비교 연구가 진행되지 않아 그 효용성의 차이를 비교, 평가 하기 위한 목적으로 진행되었다.
대상 및 방법
1. 연구설계
본 연구는 심재성 2도 화상 환자 및 부분 3도 화상환자에 서 동일부위에 Kaloderm과 Suprathel을 적용하여 그 효용 성의 차이를 비교, 평가하기 위한 비교연구이다.
5일 이내에 입원한 총 47명을 대상으로 하였으며, 환자 및 보호에게 설명 후 동의를 얻고 Kaloderm 및 Suprathel을 적용하는 연구에 참여시켰다.
동일한 깊이의 심재성 2도 화상 및 부분3도 화상환자에 서 100 cm
2이상의 화상면적을 대상으로 하였으며 성별, 연 령, 수상부위 등을 고려하여 연구에 참여시켰다.
단, 회음부, 점막부의 화상환자 및 임산부, 수유부, 스테 로이드제재, 항응고제 및 항암제복용의 과거력이 있거나 현재 복용중인 환자는 연구에서 제외하였다.
3. 연구도구 및 방법
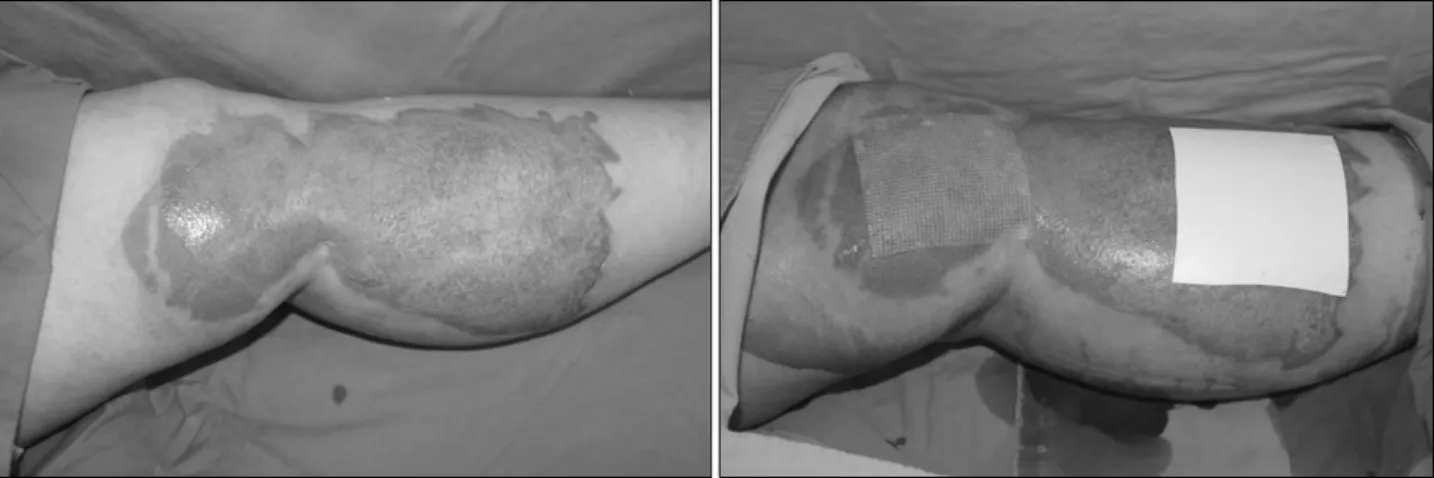
Fig. 3. A 37-year-old woman had Deep 2
nd and partial 3rd degree scalding burn. After radical debridement, Kaloderm® and Suprathel® were applied.Fig. 4. Follow-up on postoperative 15 days.
심재성 2도 및 부분3도 화상 환부의 삼출물이 감소하면서 괴사 조직, 가피(eschar) 및 딱지(scab)이 충분히 제거되어 진피층이 노출되고, 세균배양 검사에서 균이 동정되지 않 을 때 Kaloderm과 Suprathel을 적용하였으며 적용부위는 무작위로 선정하였다.
환부에 Kaloderm 및 Suprathel을 적용 후 메피렉스 폼드 레싱(Mepilex
®, Molnlycke Health Care, Sweden)을 이용 하여 드레싱하였으며 3∼5일후 첫 드레싱 교체를 하였으며 이후 2일 간격으로 재상피화 시까지 메피렉스 폼드레싱을 시행하였다(Fig. 3).
Kaloderm은 환부에 적용하고 7일째 제거하였으며 Suprathel은 환부에서 재흡수 되어 제거의 필요성이 없었다.
고정이 필요한 경우에는 Kaloderm을 나일론봉합 및 의료용 스테플러를 이용하여 피부에 고정 하여 주였고, Suprathel 은 고정이 필요하지 않았다. 환부가 사지인 경우 부목을 대 어 Kaloderm 및 Suprathel의 움직임을 최소화 하였다.
상피화의 기준은 각각 다를 수 있지만 상피화의 완료 시
까지의 기간을 치료효과에 대한 평가 및 효용성의 비교, 평 가의 기준으로 설정하였다.
저자들은 상피화의 기간을 화상상처에 Kaloderm 및 Su- prathel을 적용한 시점부터 화상상처가 치료되어 더 이상의 드레싱이 필요 없고 상처를 열어놓고 연고나 보습제를 바르 기 시작한 상태를 상피화가 완료된 것으로 정의하였다(Fig. 4).
화상반흔의 정도를 판단하기 위해 치료가 완료되어 퇴원 후 외래 방문 시 Vancouver Scar Scale
10)을 이용하였고 관 찰 기간은 3개월부터 13개월(평균 6.3개월)이었다.
4. 자료분석
수집된 자료의 통계적 분석은 SPSS 17.1 for Windows (SPSS Inc., Chicago, IL, USA)를 사용하였다. Kaloderm과 Suprathel을 적용한 부위의 상피화의 기간에 대한 비교분 석은 평균과 표준편차로 기술하였고 Paired t-test를 이용하 였으며 P-value가 0.05이하일 경우 통계학적으로 유의성이 있는 것으로 판단하였다.
결 과
연구에 참여한 대상자는 47명으로 남성이 26명(55.3%), 여성이 21명(44.7%)이었으며 평균연령은 나이는 33세(range, 2∼81세)였고 평균화상범위 5.4%였다. 평균 추적 관찰기간 은 6.2개월(3개월∼13개월)이었다. 화상의 원인으로는 열탕 화상이 41예, 화염 화상이 2예, 증기화상이 4예였다(Table 1).
화상 후 환부에서 괴사 조직, 가피(eschar) 및 딱지(scab)
를 제거하고 Kaloderm 및 Suprathel을 적용하기까지는 평
균 4.3일이 적용 후 상피화가 완료될 때까지는 Kaloderm이
평균 13.4일, Suprathel이 평균 13.4일이 소요되었다.
Tab le 1. Etiology, Site, B od y Surfa ce Ar ea a nd R e-epithelia liz ation of P atients N o . Age Sex E tiology Site TBSA (%) Du ra ti o n o f E p it h eli zat io n ( da y) Ka lo de rm
®/ Su pr at h el
®Ti me for appl ication (PBD o r PTD) 1 33 M Scal di ng b u rn (2nd) D or su m o f fo ot a n d a n kl e 3 12 /12 5 2 17 M Scal di ng b u rn (2nd) L at er al tibia 4 11 /12 3 3 60 F Scal di ng b u rn (2nd and p ar ti al 3 rd ) B u tt o ck a n d l o w er l eg 11 14/1 5 6 4 42 F Steam bur n (2 nd) A bdomen and thigh 10 12 /14 2 5 9 M Sca ld in g b u rn ( 2n d) T igh t 3 10 / 11 5 6 71 M Scal di ng b u rn (2nd and p ar ti al 3r d ) D ors um o f foo t 5 15 /16 6 7 20 F Scal di ng b u rn (2nd) T ight 6 13 /15 6 8 37 F Scal di ng b u rn (2nd and p ar ti al 3r d ) T ight 6 17 / 18 4 9 51 M Scal di ng b u rn (2nd and p ar ti al 3r d ) D ors um o f foo t 3 15 /17 3 10 33 M Scal d in g bu rn (2nd ) Dors um o f fo ot 2 12 / 14 4 11 46 F Scal d ing bu rn (2nd ) Tibia 3 15 /15 5 12 42 F Scal d in g bu rn (2nd ) For earm 3 13 /14 5 13 4 M Scal di ng b u rn (2 nd a nd p ar ti al 3r d ) D ors u m of h and 3 17 /16 3 14 68 M Scal d ing bu rn (2nd ) Thigh 5 12 /12 4 15 21 F F la me b urn (2nd) H and 3 12 /10 2 16 7 M Scal di ng b u rn (2nd) T ight 7 10 / 10 5 17 81 M Scal d in g bu rn (2nd a n d p ar ti al 3r d) Trunk and should er 12 15 / 15 5 18 17 F Sca ld in g b u rn ( 2n d) T ight and knee 6 13/12 6 19 49 F Scal d in g bu rn (2nd a n d p ar ti al 3r d) Up p er arm 4 17 /16 4 20 48 M Sca ld in g bur n ( 2n d) L at era l ti bi a 3 11/1 1 3 21 60 F F la me burn (2nd and p ar tial 3 rd ) B u tt o ck a n d a b d o m en 11 14 / 14 6N 22 16 F Steam b ur n (2 nd) H an d and wr ist 3 12 /10 2 23 2 M Scal di ng b u rn (2nd) C hest and abdomen 12 10 /8 5 24 55 M Sca ld in g b u rn ( 2n d an d pa rt ia l 3r d ) D o rs u m o f foo t an d an k le5 15 / 14 4 25 35 M Scal d in g bu rn (2nd a n d p ar ti al 3r d) Thigh and p reti b ia 8 15 / 155 26 30 F Scal d ing bu rn (2nd ) Tight 6 13 /13 6 27 47 F Scal d in g bu rn (2nd a n d p ar ti al 3r d) Tight 5 17 /19 4 28 26 M Scal d in g bu rn (2nd a n d p ar ti al 3r d) Dors um o f fo ot 3 17 / 17 3 29 39 M Scal d in g bu rn (2nd ) Dors um o f fo ot 2 12 / 13 4 30 6 F Scal di ng b u rn (2nd) C hest and ha nd 13 15 /13 5 31 3 M Scal di ng b u rn (2 nd ) D ors um of f oot and a n kle 3 12 /11 5 32 8 M Scal di ng b u rn (2 nd ) L at er al tibia 4 11 /11 3 33 51 F Scal d in g bu rn (2nd a n d p ar ti al 3r d) Bu ttock and back 11 14 /14 6N 34 15 F Steam b ur n (2 nd) F or earm 3 12 / 11 2 35 18 M Scal d ing bu rn (2nd ) Abdom en and tight 10 12 / 13 5 36 28 M Sca ld in g b u rn ( 2n d an d pa rt ia l 3r d ) D o rs u m o f foo t an d an k le4 15 / 14 7 37 12 F Steam b ur n (2 nd) T ight 6 13 /14 6
Table 2. Burn Wound Re-epithelialization Period Difference
between The Kaloderm® and Suprathel® ApplicationNo. Kaloderm® Suprathel® Difference (δ)
1 12 12 0
2 11 12 1
3 14 15 1
4 12 14 2
5 10 11 1
6 15 16 1
7 13 15 2
8 17 18 1
9 15 17 2
10 12 14 2
11 15 15 0
12 13 14 1
13 17 16 +1
14 12 12 0
15 12 10 +2
16 10 10 0
17 15 15 0
18 13 12 +1
19 17 16 +1
20 11 11 0
21 14 14 0
22 12 10 +2
23 10 8 +2
24 15 14 +1
25 15 15 0
26 13 13 0
27 17 19 2
28 17 17 0
29 12 13 1
30 15 13 +2
31 12 11 +1
32 11 11 0
33 14 14 0
34 12 11 +1
35 12 13 1
36 15 14 +1
37 13 14 1
38 15 16 1
39 17 16 +1
40 12 11 +1
41 15 13 +2
42 10 9 +1
43 15 16 1
44 13 13 0
45 11 10 +1
46 14 13 +1
47 13 13 0
Mean±SD Min∼Max
13.4±2.1 10∼17
13.4±2.4 8∼19
0.02±1.2*
2∼+2 Difference in Re-epithelialization period between The Kaloderm® and Suprathel® application. *P<0.0001.
Tab le 1. C o n ti n u ed N o . Age Sex E tiology Site TBSA (% ) Du rat ion o f E p itheli zation (da y ) Ka lo derm
®/ Supr athel
®Ti me for appl ication (PBD o r PTD) C om p lica tion 38 38 F Scal d in g bu rn (2nd a n d p ar ti al 3r d) Tight 6 15 /16 4 None 39 51 M Scal d in g bu rn (2nd a n d p ar ti al 3r d) Dors um o f fo ot 3 17 / 16 3 N o ne 40 15 M Scal d ing bu rn (2nd ) For earm and elbow 5 12 /11 4 None 41 49 F Sca ld in g bur n ( 2n d) Sh o ld er an d u pper ar m 6 15 /1 3 5 N o n e 42 22 F Sca ld in g b u rn ( 2n d) Fa ce a n d n ec k 3 10 / 9 6 N on e 43 56 F Scal d in g bu rn (2nd a n d p ar ti al 3r d) Tight 6 15 /16 4 None 44 55 M Scal d in g bu rn (2nd a n d p ar ti al 3r d) Dors um o f fo ot 3 13 / 13 3 N o ne 45 42 M Scal d in g bu rn (2nd ) Dors um o f fo ot 2 11 / 10 4 N one 46 5 M Scal di ng b u rn (2nd and p ar ti al 3r d ) T ight 6 14 / 13 4 N one 47 12 M Scal d in g bu rn (2nd a n d p ar ti al 3r d) Dors um o f fo ot 3 13 / 13 3 N o ne Average 33 (2 ∼ 81) 5.4 (2 ∼ 13) 13. 4/1 3.3 8 (10 ∼ 17 /8 ∼ 19 ) 4.3 (2 ∼ 7)
(minimal resistance)
2 Mixed Yielding
(moderate resistance)
2∼5 mm Red
3 Hyperpigmented Firm >5 mm Purple
4 Ropes
5 Contracture
Kaloderm 및 Suprathel 적용부위의 상피화에 따른 기간에 차이는 통계학적으로 유의한 차이를 보이지 않았다(Table 2).
하지만 통계학적으로는 유의한 차이를 보이지 않는다 하 더라도 대부분의 수부, 관절 및 소아화상환자의 경우에서 는 Suprathel 적용부위가 Kaloderm 적용부위보다 1∼2일 빠른 상피화를 보였고 그 외의 화상환자에서는 Kaloderm 적용부위의 상피화가 1∼2일 빠른 상피화를 보였다고 임상 적으로 판단할 수 있다(Table 1, 2).
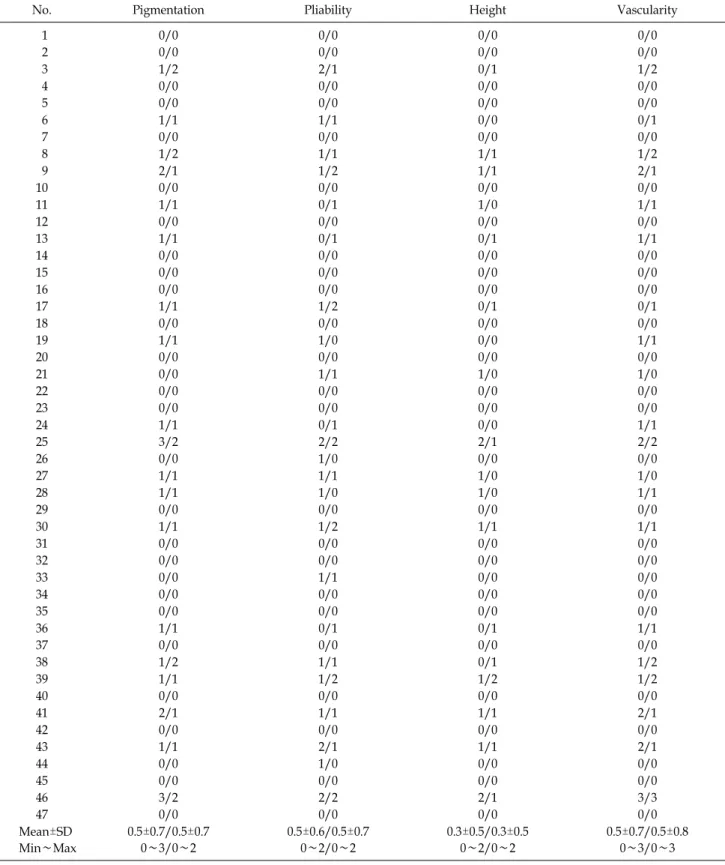
Vancouver Scar Scale을 이용하여 반흔의 상태를 평가하 였으며, 환자 전체의 평균 총 점수는 Kaloderm 및 Suprathel 이 동일하게 1.8점이었고, 항목별로도 pigmentation 평균 0.5점, Vascularity 평균 0.5점, Pliability 평균 0.5, Height 평 균 0.3점으로 판단되었다. 상피화에 대한 평가 및 반흔의 상 태 평가는 3명의 성형외과 전문의가 하였다(Table 3, 4).
고 찰
화상으로 의하여 손상을 받았을 때 화상의 깊이와 범위 에 따라서 적절한 치료가 이루어져야 화상으로 인한 후유 증을 최소화할 수 있다. 이에 화상의 깊이에 따라 보존적 화상처치 및 피부이식술, 피판술이 선택되고 있으나 수술 적 처치를 원하지 않거나 수술적 처치에 제한이 있는 경우 에 적용 될 수 있는 다양한 방법들이 개발되고 있다.
1975년에 Rheiwald와 Green이 인간 피부 각질세포 (human keratinocyte)를 배양하는 조건을 확립하고 발표한 이후
1)자가 유래 배양피부가 연구, 개발되어 사용되면서 1980년대 말부터는 동종유래배양피부가 개발되고 발전되 어 왔다
2-7). 국내에서는 여러 연구를 통해 동종유래 배양피 부를 이용하여 치료한 부분층 2도 화상 치료에 있어서 상처 치유 촉진 효과 및 환부의 상피화 정도, 환자의 만족도, 통 증의 감소 정도가 우수한 것으로 보고되었다
9).
국내에서 제품화되어 사용하고 있는 동종 유래 배양피부
α, IL-1β, IL-6, IL-8, GM-CSF, keratinocyte derived T-cell growth factor등과 같이 동종유래배양피부에서 생성, 분비 되는 cytokine에 의하여 화상상처 내와 상처 주변의 피부세 포의 증식과 이동을 일으키고 치유를 촉진하는 것으로 알 려져 있다
11-14). 또한 동종배양피부는 Epidermal Cell-de- rived Factor (EDF)을 분비하는 것으로 밝혀졌는데 이는 섬 유모세포의 수축을 억제하여 반흔 형성과 구축을 줄인다고 보고되었다
7,15). 이러한 작용을 통하여 동종유래 배양피부 는 피부의 재상피화를 촉진하고 비후성 반흔이나 구축을 최소화 할 수 있다.
젖산 융합체 합성창상치료제인 수프라셀((synthetic film made of Lacto-Capromer and Polylactic Acid, Suprathel
®(Polymedics Innovations GmbH, Germany)은 2004년 독일 에서 제품화되어 사용 중으로 창상에 적용 시 생체에 재흡 수 되는 특성으로 관절부 및 안면부 특히 소아환자들에 적 용이 용이하며 재흡수시의 산물로 인해 상처주변의 산도가 증가되어 Protease의 작용저해 및 Collangen 합성, Fibro- blast의 이동, Vascular Endothelial Growth Factor (VEGF)의 활성화를 촉진시키는 것으로 보고 되었다
8).
본 연구의 결과에서 Kaloderm 및 Suprathel 적용시 상피 화의 기간의 차이는 통계학적으로 유의한 차이를 보이지 않았다.
하지만 수부, 관절, 소아환자의 경우 Suprathel의 적용 시 상피화에서 더 적은 기간이 소요된 것을 확인 할 수 있다.
이는 Kaloderm이 환부에 잘 부착되도록 유지되지 못하여 상피화가 더뎠을 것으로 생각된다.
Kaloderm 및 Suprathel을 적용시 환부에 적용한 후 상피 화까지 약 13.4일 걸렸고 3개월에서부터 13개월까지 외래 경과 관찰 시 비후성 반흔, 구축 및 색소침착의 발생은 거의 관찰되지 않았다.
47명의 연구 대상환자에서 이상반응으로 판단할 수 있는 증상은 보이지 않았으며 이는 3명의 성형외과 전문의가 평 가 하였다.
Kaloderm의 적용에 대한 연구는 매우 활발히 진행되었 으며 그 효과 및 치료범위에 대해서도 널리 알려져 있으나 Suprathel의 경우, 국내에서 화상환자들에게 적용된 보고 및 연구가 많지 않으며 화상치료에서 널리 사용되는 Kalo- derm과의 효과에 대한 비교연구가 존재하지 않아 연구계 획단계에서부터 이를 비교하는 것이 중요한 점이었다.
단, 본 연구의 제한점으로는 첫째, 대조군의 설정에 있어
Table 4. Vancouver Scar Scale Difference between The Kaloderm
® and Suprathel® application (Kaloderm®/Suprathel®)No. Pigmentation Pliability Height Vascularity
1 0/0 0/0 0/0 0/0
2 0/0 0/0 0/0 0/0
3 1/2 2/1 0/1 1/2
4 0/0 0/0 0/0 0/0
5 0/0 0/0 0/0 0/0
6 1/1 1/1 0/0 0/1
7 0/0 0/0 0/0 0/0
8 1/2 1/1 1/1 1/2
9 2/1 1/2 1/1 2/1
10 0/0 0/0 0/0 0/0
11 1/1 0/1 1/0 1/1
12 0/0 0/0 0/0 0/0
13 1/1 0/1 0/1 1/1
14 0/0 0/0 0/0 0/0
15 0/0 0/0 0/0 0/0
16 0/0 0/0 0/0 0/0
17 1/1 1/2 0/1 0/1
18 0/0 0/0 0/0 0/0
19 1/1 1/0 0/0 1/1
20 0/0 0/0 0/0 0/0
21 0/0 1/1 1/0 1/0
22 0/0 0/0 0/0 0/0
23 0/0 0/0 0/0 0/0
24 1/1 0/1 0/0 1/1
25 3/2 2/2 2/1 2/2
26 0/0 1/0 0/0 0/0
27 1/1 1/1 1/0 1/0
28 1/1 1/0 1/0 1/1
29 0/0 0/0 0/0 0/0
30 1/1 1/2 1/1 1/1
31 0/0 0/0 0/0 0/0
32 0/0 0/0 0/0 0/0
33 0/0 1/1 0/0 0/0
34 0/0 0/0 0/0 0/0
35 0/0 0/0 0/0 0/0
36 1/1 0/1 0/1 1/1
37 0/0 0/0 0/0 0/0
38 1/2 1/1 0/1 1/2
39 1/1 1/2 1/2 1/2
40 0/0 0/0 0/0 0/0
41 2/1 1/1 1/1 2/1
42 0/0 0/0 0/0 0/0
43 1/1 2/1 1/1 2/1
44 0/0 1/0 0/0 0/0
45 0/0 0/0 0/0 0/0
46 3/2 2/2 2/1 3/3
47 0/0 0/0 0/0 0/0
Mean±SD Min∼Max
0.5±0.7/0.5±0.7 0∼3/0∼2
0.5±0.6/0.5±0.7 0∼2/0∼2
0.3±0.5/0.3±0.5 0∼2/0∼2
0.5±0.7/0.5±0.8 0∼3/0∼3
드레싱 만을 시행하는 대조군은 연구에서 제외하였다. 둘 째, 대부분 화상이 열탕화상으로 다른 종류의 화상환자에 서의 연구결과가 부족하다는 것과 셋째, 단일기관에서의 환자만을 대상으로 하였다는 점이다.
소아환자 및 고령환자의 경우, 수술적 치료를 원하지 않는 경우가 있으며 수술을 시행한 경우에도 수술부위의 유지 및 협조가 어려운 것이 사실이다. 또한 안면부의 경우 수술 적 처치로 인한 반흔의 가능성으로 수술의 결정이 쉽지 않 다. 이런 경우 Kaloderm 혹은 Suprathel을 이용한 화상치 료를 선택 할 수 있으며 Kaloderm의 경우 국민건강보험의 혜택이 적용되어 환자의 부담을 덜어 줄 수 있고, Suprathel 은 Kaloderm의 적용에 제한이 있는 안면부, 수부, 관절면, 소아 및 고령환자에게서 적용을 고려 할 수 있다.
결 론
Kaloderm 및 Suprathel은 수술적 처치가 어려운 경우 및 원하지 않는 경우의 심재성 2도 및 부분 3도 화상치료에서 고려 가능한 방법이다.
Kaloderm의 효능 및 효과에 대한 많은 연구가 진행되고 실제 임상에서 많이 적용되고 있으나 보관상의 문제(냉동 보관 및 유효기간의 존재)와 적용의 제한점이 있는 환자 및 신체부위 등이 있어 Suprathel의 적용을 고려해 볼 수 있으 며 본 연구의 결과 화상치료효과는 통계학적으로 유의한 차이를 보이지 않음을 확인 할 수 있다.
따라서 Kaloderm 및 Suprathel을 이용한 치료가 모든 심 재성 2도 이상의 화상환자에게 적용 가능하다고 할 수는 없지만 적절한 적응증을 선별하여 사용한다면 수술적 처치 가 아닌 보조적 치료방법으로 선택 가능하다는 것을 보고 하는 바이다.
REFERENCES
1) Rheinwald JG, Green H. Seria cultivation of strains of human epidemal keratinocytes: the formation keratinizin colonies from single cells. Cell. 1975;6:331-343.
2) O'Connora NE, Mullikena J, Susan BS, Kehindeb O, Green H.
Gragting of burns with cultured epithelium prepared from autologous epidermal cellas. Lancet. 1981;1:75-78.
3) Gallico GG III, O'Connor NE, Compton CC, Kehinde O, Green
5) Harvima IK, Virnes S, Kauppinen L, Huttunen M, Kivinen P, Niskanen L, et al. Cultured allogeneic skin cells are effective in the treatment of chronic diabetic leg and foot ulcers. Acta Derm Venereol. 1999;79:217-220.
6) Fratianne R, Papay F, Housini I, Lang C, Schafer IA.
Keratinocyte allografts accelerate healing of split-thickness donor sites: applications for improved treatment of burns.
The Journal of Burn Care & Rehabilitation. 1993;14:148-154.
7) Yanaga H, Udoh Y, Yamauchi T, Yamamoto M, Kiyokawa K, Inoue Y, et al. Cryopreserved cultured pidermal allografts achieved early closure of wounds and reduced scar formation in deep partial-thickness burn wounds (DDB) and split- thickness skin donor sites of pediatric patients. Burns.
2001;27:689-698.
8) Uhlig C, Rapp M, Hartmann B, Hierlemann H, Planck H, Dittel K.K. Suprathel - an innovative, resorbable skin substitute for the treatment of burn injury victims. Burns 2007;33: 221-229
9) Choi WY, Kim GB, Yang JY. The Usefulness of Cultured Allogenic Keratinocyte(Kaloderm®) for 2nd Degree Burn Patient Treatment. Journal of Korean Burn Society. 2011;14:111-117.
10) Shin JC, Seo CH, Jang KU. Scar Quality and Hand Function after Moist Exposed Burn Ointment and Skin Graft Treatment in Full Thickness Hand Burn J Korean Acad Rehab Med 2007;31:582-589
11) Robert JC Jr, Derynck R, Wilcox JN, Bringman ST, Goustin AS, Moses HL, et al. Production and auto-induction of trans- forming growth factor in human keratinocytes. Nature.
1987;328:817-820.
12) Kupper TS, Ballard DW, Chua AO, McGuire JS, Flood PM, Horowitz MC, et al. Human keratinocytes contain mRNA indistinguishable from monocyte interleukin-1 alpha and beta mRNA. Keratinocyte epidermal cell-derived thymocyte-activating factor is identical to interleukin 1. JEM. 1986;164:2095-2100.
13) Larsen CG, Anderson AO, Oppenheim JJ, Atsushima KM.
Production of interleukin-8 by human dermal fibroblasts and keratinocytes in response to interleukin-1 or tumor necrosis factor. Immunology. 1989;68:31-36.
14) Kupper ST, Lee F, David C, Jeffrey C, Patrick F, Mark H.
Keratinocyte derived T-cell growth factor(KTGF) is identical to granulocyte marcophage colony stimulating factor(GM- CSF). J Invest Dermatol. 1988;91:185-188.
15) Eisinger M, Sadan S, Silvers IA, Flick RB. Growth regulation of skin cells by epidermal cell-derived factors: Implications for wound healing(re-epithelization/keratinocytes/fibroblast inhibition). Proc Natl Acad Sci USA. 1988;86:1937-1941.