서 론
호흡기 감염은 병원에 입원하는 소아의 주된 진단이며,1 호흡기 계의 이상은 중환자실에 입원하는 소아의 가장 흔한 주 진단 중 하 나이다.2 비 호흡기계 주 진단까지 포함하였을 때 중환자실에 입실 한 소아 환자의 약 70% 이상이 호흡기 보조 치료를 받는다.3 그러나 중환자실에 입원한 소아는 연령이나 기저질환 등에 따라 다양한 경과를 보이기 때문에, 호흡기 보조를 받은 환자의 예후는 다양하 게 나타난다. 호흡곤란으로 중환자 치료가 필요했던 환자들의
32%–58%가 선천성심장질환, 후천성면역저하 또는 만성폐질환 등 의 복잡한 기저질환을 가지고 있었으며,4-7 이러한 만성병력은 사망 의 유의한 위험 인자로 보고되었다.8,9 급성폐손상으로 입원한 소아 에서 면역저하 환자는 정상 면역 환자에 비해 6.3배의 사망을 보였 으며, 기존에 만성장기 부전을 가진 급성폐손상 환자는 그렇지 않 은 경우에 비해 3배의 사망 위험을 보였다.4
만성의 기저질환이 호흡기질환에서 중요한 사망 위험 요인임에 도 불구하고 이러한 위험 인자가 없던 건강한 소아에서도 호흡기계 의 악화는 사망의 중요한 원인이다. 인플루엔자와 관련된 소아의 Allergy Asthma Respir Dis 6(2):103-109, March 2018 https://doi.org/10.4168/aard.2018.6.2.103 ORIGINAL ARTICLE
Correspondence to: Joongbum Cho https://orcid.org/0000-0001-5931-7553
Department of Critical Care Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, 81 Irwon-ro, Gangnam-gu, Seoul 06351, Korea
Tel: +82-2-3410-6399, Fax: +82-2-2148-7088, E-mail: [email protected] Received: July 3, 2017 Revised: August 18, 2017 Accepted: August 23, 2017
© 2018 The Korean Academy of Pediatric Allergy and Respiratory Disease The Korean Academy of Asthma, Allergy and Clinical Immunology This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License
(Allergy Asthma Respir Dis 2018;6:103-109)
만성 병력 없이 호흡보조를 위해 중환자실에 입원한 소아의 특성 및 예후인자
정민영1, 김민지2, 이옥정3, 최아영4, 황태웅4, 조중범4
1성균관대학교 의과대학 삼성서울병원 소아청소년과, 2한림대학교 의과대학 동탄성심병원 소아청소년과, 3서남대학교 의과대학 명지병원 소아청소년과,
4성균관대학교 의과대학 삼성서울병원 중환자의학과
Characteristics and prognostic factors of previously healthy children who required respiratory support in a pediatric intensive care unit
Minyoung Jung¹, Minji Kim2, Ok Jeong Lee3, Ah Young Choi4, Taewoong Hwang4, Joongbum Cho4
1Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul; 2Department of Pediatrics, Hallym University Dongtan Sacred Heart Hospital, Hallym University School of Medicine, Hwaseong; 3Department of Pediatrics, Myongji Hospital, Seonam University College of Medicine, Goyang; 4Department of Critical Care Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea
Purpose: Comorbidities have been considered a mortality risk factor in pediatric critical care patients. We studied the characteristics and prognostic factors of children without comorbidities who were admitted to the intensive care unit (ICU) due to respiratory failure.
Methods: We reviewed the medical charts of patients (<18 years) admitted to the ICU for respiratory support in a single tertiary cen- ter between January 2006 and December 2016. Patients with comorbidities and perioperative statuses were excluded.
Results: Of the 4,712 ICU patients, 73 (1.5%) were included in this study. The median age was 31 months (8–57) and 51 (69.9%) were boys. Twenty-nine patients (39.7%) presented with pneumonia, 14 (19.2%) with acute respiratory distress syndrome (ARDS), and 11 (15.1%) with obstructive airway disease. The median duration of ICU hospitalization was 5 days (2–14.5), and 45 of the 73 patients (61.6%) needed mechanical ventilation. Mortality was 13.7% (10/73). None of the patients with pneumonia or obstructive airway disease died. The most frequent cause of death was ARDS (5 of 10, 50%). In adjusted analysis, the extent of extrapulmonary organ dysfunction was significantly associated with mortality (odds ratio, 2.89; 95% confidence interval, 1.17–7.11; P= 0.023).
Conclusion: The mortality rate of previously healthy pediatric patients needing respiratory support in the ICU should not be negligi- ble. Multiple organ dysfunctions might be a significant risk factor for mortality in such patients. (Allergy Asthma Respir Dis 2018;6:103-109) Keywords: Child, Respiratory insufficiency, Comorbidity, Critical care, Mortality
사망을 분석한 연구에서 사망한 환자의 43%는 고위험 질환이 없 던 건강한 환자였고,10 호흡기세포융합바이러스(respiratory syncy- tial virus) 감염이 원인이었던 영유아 사망의 30%는 만성병력이 없 는 건강한 환자였다.11 따라서 이전에 건강하였다고 해서 소아의 호 흡기 관련 사망 위험을 무시할 수 없다. 만성병력이 없는 소아의 경 우 중환자실에 처음 입원하는 경우가 많으며 이때 보호자의 심리 적 스트레스는 이전에 입원 경험이 있던 경우에 비해 의미 있게 높 은 것으로 알려져 있으며,12 환자의 상태에 대해 적시에 정확한 설명 을 해주는 것은 보호자에게 매우 중요하다.13 그러나 이전에 건강하 였던 환자가 호흡기 악화에 의해 중환자실에 입원한 경우 예후에 대한 연구는 거의 없는 실정이어서 정확한 설명이 어려운 상태이 다. 따라서 이 연구에서는 호흡곤란으로 중환자실에 입원한 환자 중 만성질환이 없었던 소아의 임상적인 특징과 예후 인자를 분석 하고자 하였다.
대상 및 방법
1. 연구 대상
2006년 1월 1일부터 2016년 12월 31일까지 삼성서울병원 소아 중 환자실에서 산소 치료를 받은 18세 미만 환자 4,712명 중 진단 코드 및 의무기록을 후향적으로 확인하여 기저질환이 없는 환자를 대상 으로 하였다. 기저질환의 기준은 주상병과 부상병 중에 종양, 면역 결핍, 선천성 기형 및 증후군, 주산기질환, 만성폐질환, 천식, 난치성 간질, 염증성장질환, 자가면역질환을 한 가지라도 진단받은 환자로 정의하였다. 또한 수술 후 관찰을 위해 중환자실에 입원한 환자도 수술이 필요한 기저질환이 있는 것으로 간주하여 대상에서 제외하 였다. 본원 소아 중환자실의 호흡기계 입실 기준은 산소포화도 90% 이상 유지하기 위하여 흡입 산소 분율이 0.5 이상 필요한 경우, 무호흡 또는 호흡 수가 나이에 따른 정상 범위보다 낮은 경우, 진행 하는 호흡성산증 또는 생명을 위협하는 폐 또는 기도질환이 있는 경우, 이외 중증 혹은 생명을 위협할 수 있는 폐 및 기도질환이 있 는 경우이다.
2. 자료의 수집
입실 당시의 평가 항목으로는 연령, 성별, 몸무게, 전원 유무, 진 단명, 호흡 중증도 지표, 예측 사망률들을 수집하였다. 그리고 원인 병원체 동정 유무와 종류, 입실 기간 동안 최종적으로 적용했던 비 침습적 기계 환기와 침습적 기계 환기 종류, 기계 환기 치료 기간, 동 반된 장기 부전의 유무를 조사하였다. 호흡 보조는 환자의 중증도 가 증가됨에 따라 비강캐뉼라, 산소마스크, 비침습적 기도환기, 기 계환기, 고빈도 진동 환기(high frequency oscillatory ventilation), 체외막 순환 장치(extracorporeal membrane oxygenation)의 순서 로 적용하거나 일부가 생략되어 적용하였다. 중환자실에서 시행한
중재(intervention), 중환자실 입실 기간과 전체 재원 일수, 사망 유 무를 조사하였다.
진단명은 급성호흡곤란증후군(acute respiratory distress syn- drome, ARDS), 폐렴, 폐쇄성기도질환(천식, 모세기관지염), 패혈증 그리고 신경질환(뇌염, 뇌수막염, 대사성 뇌증)으로 분류하였다.
ARDS는 American-European Consensus Conference14 정의를 기 준으로 하여 진단하였다. 패혈증과 다발성장기부전은 Goldstein 등의 연구15에서 제안한 기준을 이용하여 평가하였으며 사망 전 24 시간 이내의 장기 부전이 새로 발생한 경우는 사망 과정으로 간주 하고 제외하였다. 심혈관계 부전은 한 시간 이내 정맥 내 생리식염 수 40 mL/kg 이상 투여하였음에도 불구하고 나이 정상 범위의 5th percentile 혈압보다 감소하거나, 정상 범위의 혈압을 유지하기 위해 혈관수축제(dopamine>5 μg/kg/min 또는 모든 용량의 dobuta- mine, epinephrine, norepinephrine)가 필요한 경우, 또는 다음 중 두 가지 이상 해당하는 경우로 정의하였다. (1) 설명되지 않은 대사 성 산증(base deficit >5.0 mEq/L), (2) 동맥혈 내 젖산염 >정상 상 위 2배, (3) 소변량 <0.5 mL/kg/hr, (4) 모세혈관 재 충만 시간 >5초, (5) 중심 체온과 말초 체온의 차이 >3°C. 신경학적 부전은 Glasgow Coma Score가 11점 미만이거나 급격한 의식 변화가 있으면서 Glasgow Coma Score가 기저보다 3점 이상 낮아질 때로 정의하였다. 그리고 혈액학적 부전은 혈소판이 80,000/mm3보다 낮아지는 경우 또는 international normalized ratio이 2 이상인 경우로 정의하였다. 신 부전은 혈청 크레아티닌(creatinine)이 정상 범위 중 상위 값의 2배 이상이거나 기저치보다 2배 이상 증가한 경우로 정의하였다. 마지 막으로 간부전은 총 빌리루빈(bilirubin) 값이 4 mg/dL 이상이거나 alanine aminotransferase가 정상 값의 2배 이상인 경우로 정의하 였다.
호흡 중증도의 지표들로는 입실 당시 호흡 수, 입실 24시간 이내 와 입실 당시부터 사망 또는 퇴실 24시간 이전 기간 동안 제일 낮았 던 경피 산소포화도/흡입 산소 분율(saturation by pulse oxymeter [SpO2]/fraction of inspiratory oxygen [FiO2])의 비, 동맥혈 이산화 탄소 분율 등을 조사하였다. 동맥혈 산소 분압/흡입 산소 분율(ar- terial partial pressure of oxygen [PaO2]/FiO2)비는 동맥혈가스검사 결과가 있는 환자에서만 조사하였다. 예측 사망률은 Pediatric In- dex of Mortality 3 score 방법16으로 계산하였다.
호흡 보조 치료는 침습적, 비침습적으로 나누었고 비침습적 환 기 방법의 종류를 조사하였다. 중환자실 중재의 종류는 기계 환기 유무, 기계 환기 시작 후부터 사망 또는 기계 환기 이탈 24시간 이전 까지 중 제일 높았던 기계 설정값, 고빈도 진동 환기 요법, 산화질소, 근육 이완제, 승압제, 체외막 순환 장치 적용 유무를 확인하였다. 기 계 환기 설정값은 압력 조절형 방식에서 호기말 양압(positive end- expiratory pressure, PEEP), 최대 흡기압(peak inspiratory pres- sure, PIP), above PEEP (PIP과PEEP의 차이) 등을 조사하였다. 비
침습적 환기 치료는 비강내 캐뉼라, 산소 마스크, 지속적 호기말 양 압 장치, 고유량 산소 캐뉼라로 구분하였다.
원인 병원체의 확인은 입원 중 감염이 아닌 중환자실 입실 당시 시행한 검체에서 바이러스와 세균감염이 확인된 경우로 정의하였 다. 바이러스 감염은 객담, 대변, 혈액, 뇌척수액 등의 중합 연쇄반 응(polymerase chain reaction, PCR)에서 양성으로 나온 경우, 세 균 감염은 객담이나 혈액, 뇌척수액 배양검사에서 동정된 경우로 정의하였다.
3. 통계 분석
생존자와 비생존자를 비교할 때 성별, 전원 유무, 진단, 원인 병원 체, 장기 부전의 수, 기계 환기 적용 유무, 중환자실 중재 유무 등은 chi-square test 또는 Fisher exact test를 사용하였고, 연령, 중환자 실 재실 기간, 예측 사망률, 호흡 중증도 지표들은 Mann-Whitney U-test를 이용하였다. P값이 0.05 미만일 때 통계적으로 유의하다 고 판단하였다. 중환자실 사망자의 위험 인자를 구하기 위하여 단 변량 분석에서 통계적으로 유의했던 변수들 중 혼란 변수들(예측 사망률, 중환자실 중재, 기계 환기 기간, 가장 높았던 이산화탄소 분 율)을 제외하였다. 성별, 진단의 종류, 장기 부전의 수, above PEEP 등을 이용하여 다변량 회귀분석을 시행하였다. 모든 통계 분석은 IBM SPSS Statistics ver.23.0 (IBM Co., Armonk, NY, USA)을 이용 하였다.
결 과
1. 중환자실에 입원한 환자의 임상적인 특징
11년동안 중환자실에 입실한 소아 중 호흡 보조를 받았던 4,712 명의 환자 중 기저질환이 있었던 4,639명을 제외하고 73명(1.5%)이 연구에 포함되었다. 대상 환자의 연령은 중앙값(범위) 31 (8–57)개 월이었고 남자는 51명(69.9%)이었다(Table 1). 타 병원으로부터 전 원받아 직접 중환자실에 입실하는 환자는 34명(46.6%)이었다. 호흡 보조 치료가 필요한 원인 질환은 폐렴이 29명(39.7%)으로 빈도가 제일 높았고, ARDS, 폐쇄성기도질환, 패혈증, 신경계질환 순으로 있었다. 기계환기를 시행한 환자는 45명(61.6%), 치료 일수는 중앙 값 8 (4–18.5)일이었다. 비침습적 치료를 한 환자는 28명(38.4%), 치 료 일수의 중앙값은 2 (1–3)일이었고 그 중 비강내 캐뉼라를 제일 많이 사용하였다(20/28, 71.4%). 호흡 보조를 받은 전체 환자의 중 환자실 재원 기간은 중앙값 5 (2–14.5)일, 병원 입원 일수는 중앙값 11 (7–28.5)일이었다. 14명의 ARDS 환아에서 PaO2/FiO2비는 중앙 값 77 (52.5–142.7)이었고 Berline 정의에 따라 중증도를 분류하였 을 때 7명이 중증(PaO2/FiO2비 <100)에 속하였다.
호흡기바이러스는 46명, 단순포진바이러스는 2명, 장바이러스 가 1명에서 검출되었고, 2명에서 호흡기바이러스 중복감염이 있었
다. 호흡기바이러스 중 인플루엔자 바이러스 17명(37%), 호흡기융 합바이러스 10명(21.7), 파라인플루엔자 7명(15.2%)이 발견되었다.
기계 호흡 치료와 비침습적 호흡 치료의 중증도를 비교했을 때 입실 24시간 이내 제일 낮았던 SpO2/FiO2비는 유의한 차이가 있었 Table 1. Clinical characteristics of admitted pediatric patients who required re- spiratory support in the intensive care unit (n= 73)
Variable Value
Demographics
Age (mo) 31 (8–57)
Male sex 51 (69.9)
Body weight
< 3rd percentile 65 (89.0)
3rd–95th percentile 6 (8.2)
> 95th percentile 1 (1.4)
Transfer from other hospitals 34 (46.6)
Clinical characteristics Causes of respiratory support
ARDS 14 (19.2)
Pneumonia 29 (39.7)
Airway obstructive disease 11 (15.1)
Sepsis 10 (13.7)
Neurologic disorder 9 (12.3)
Identified pathogens 56 (76.7)
Extrapulmonary organ dysfunction 28 (38.4)
PICU LOS (day) 5 (2.0–14.5)
Hospital LOS (day) 11 (7.0–28.5)
Death 10 (13.7)
Interventions
Invasive MV 45 (61.6)
HFOV 11 (24.4)
ECMO 8 (17.8)
Noninvasive 28 (38.4)
Nasal cannula 21 (71.4)
Mask with reservoir 4 (14.8)
CPAP 2 (7.1)
HFNC 1 (3.5)
Respiratory parameters
Respiratory rate at admission 40 (32–48)
Worst SpO2/FiO2 within 24 hr 240 (121–384) Worst SpO2/FiO2 during hospitalization 230 (108–367) Highest PaCO2 during hospitalization 52 (41–68)
PaO2/FiO2 ratio* 77 (53–143)
Values are presented as median (interquartile range) or number (%).
ARDS, acute respiratory distress syndrome; PICU, pediatric intensive care unit; LOS, length of stay; MV, mechanical ventilation; HFOV, high frequency oscillation ventila- tion; ECMO, extracorporeal membrane oxygenation; CPAP, continuous positive air- way pressure; HFNC, high flow nasal cannula; SpO2, saturation by pulse oxymeter;
FiO2, fraction of inspired oxygen; PaCO2, partial arterial pressure of carbon dioxide;
PaO2, partial arterial pressure of oxygen.
*Values are calculated in the patients with acute respiratory distress syndrome.
다(중앙값 180 [245–396] vs. 중앙값 343 [245–396], P<0.001). 나 이, 성별, 입실 당시 호흡 수는 두 그룹 사이에 유의한 차이는 보이 지 않았다.
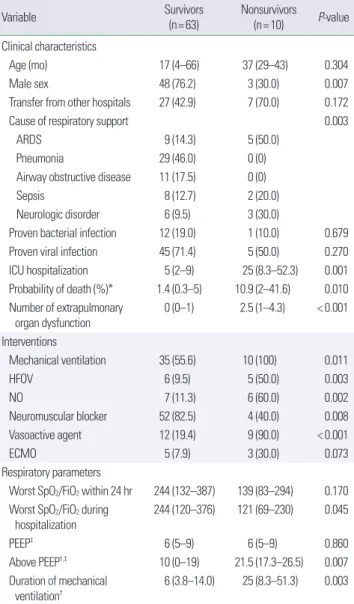
2. 소아 중환자실 사망의 위험 인자 분석
이 연구에 포함된 환자들의 사망률은 13.7% (10/73)이었다. 호흡 곤란의 원인이 폐렴과 폐쇄성기도질환이었던 환자는 모두 생존하 였다(Table 2). 생존자와 비생존자를 비교하였을 때 사망군에서 여
성의 비율(76.2% vs. 30%, P= 0.007)과 장기 부전의 수(0 [0–1] vs.
2.5 [1–4.3], P<0.001)가 생존군에 비해서 의미 있게 높았다. 입실 24시간 이내 제일 낮았던 SpO2/FiO2비, PIP과 PEEP 등의 변수들은 사망군과 생존군에서 유의한 차이는 없었다. 대신 입원 기간 중 제 일 낮았던 SpO2/FiO2비의 중앙값(244 [120–376] vs. 121 [69–230], P= 0.045)과 above PEEP (10 [0–19] vs. 21.5 [17.3–26.5], P= 0.007) 은 두 군에서 유의한 차이를 보였다. 사망률과 연관성이 확인된 임 상 변수들을 보정하여 시행한 다변량 분석에서는 사망위험도가 폐 외 장기부전 수와 의미 있게 상관 있었으며(adjusted odds ratio [OR], 2.89; 95% confidence interval [CI], 1.17–7.11; P= 0.023) (Ta- ble 3) 다른 변수들은 유의한 상관 관계를 보이지 않았다.
3. 사망한 환자들의 임상적 특징
사망한 환자들은 모두 기계환기를 적용하였다. 사망한 환자들 중 ARDS는 5명이었고 ARDS의 원인은 원인 불명이 3명, RSV 폐렴 1명, 폐조직검사에서 증명된 necrotizing bronchiolitis가 1명이었다 (Table 4). ARDS가 없이 패혈증 쇼크가 있었던 환자 중 1명은 대변 에서 장바이러스 PCR이 양성이었고, 1명은 혈액에서 단순포진 바 이러스 PCR이 양성으로 나왔다. 신경질환으로는 사망한 환자는 뇌염 2명과 간성 대사 뇌증 1명으로 모두 사망 전 뇌사에 합당한 소 견을 보여 치료를 중단하였다.
고 찰
저자들은 기저질환이 없었던 소아 환자들이 호흡보조 치료가 필요하여 중환자실에 입원하였을 때 임상적인 경과와 사망 위험 인 자에 대해 분석하였다. 연구 대상자의 전체 사망률은 13.7%였고 원 인 질환 중 ARDS가 동반되지 않은 폐렴이 전체 입실 중 39.7%으 로 제일 많았다. ARDS로 진단받은 14명의 환자들은 5명(35.7%)이 Table 2. Comparison between survivors and nonsurvivors in intensive care unit
Variable Survivors
(n= 63) Nonsurvivors (n= 10) P-value Clinical characteristics
Age (mo) 17 (4–66) 37 (29–43) 0.304
Male sex 48 (76.2) 3 (30.0) 0.007
Transfer from other hospitals 27 (42.9) 7 (70.0) 0.172
Cause of respiratory support 0.003
ARDS 9 (14.3) 5 (50.0)
Pneumonia 29 (46.0) 0 (0)
Airway obstructive disease 11 (17.5) 0 (0)
Sepsis 8 (12.7) 2 (20.0)
Neurologic disorder 6 (9.5) 3 (30.0)
Proven bacterial infection 12 (19.0) 1 (10.0) 0.679
Proven viral infection 45 (71.4) 5 (50.0) 0.270
ICU hospitalization 5 (2–9) 25 (8.3–52.3) 0.001
Probability of death (%)* 1.4 (0.3–5) 10.9 (2–41.6) 0.010 Number of extrapulmonary
organ dysfunction 0 (0–1) 2.5 (1–4.3) < 0.001 Interventions
Mechanical ventilation 35 (55.6) 10 (100) 0.011
HFOV 6 (9.5) 5 (50.0) 0.003
NO 7 (11.3) 6 (60.0) 0.002
Neuromuscular blocker 52 (82.5) 4 (40.0) 0.008
Vasoactive agent 12 (19.4) 9 (90.0) < 0.001
ECMO 5 (7.9) 3 (30.0) 0.073
Respiratory parameters
Worst SpO2/FiO2 within 24 hr 244 (132–387) 139 (83–294) 0.170 Worst SpO2/FiO2 during
hospitalization 244 (120–376) 121 (69–230) 0.045
PEEP‡ 6 (5–9) 6 (5–9) 0.860
Above PEEP†,‡ 10 (0–19) 21.5 (17.3–26.5) 0.007
Duration of mechanical ventilation†
6 (3.8–14.0) 25 (8.3–51.3) 0.003
Values are presented as median (interquartile range) or number (%).
ARDS, acute respiratory distress syndrome; ICU, intensive care unit; HFOV, high fre- quency oscillation ventilation; NO, nitric oxide; ECMO, extracorporeal membrane ox- ygenation; SpO2, saturation by pulse oximeter; FiO2, faction of oxygen; PEEP, positive end expiratory pressure.
*Values are calculated by the Pediatric Index of Mortality (PIM) 3 score. †Values are calculated in the mechanically ventilated patients. ‡Values are calculated in the me- chanically ven (PIP) and PEEP in the pressure control mode.
Table 3. Risk factors associated with mortality in previous healthy children who admitted to pediatric intensive care unit
Variable OR (95% CI) P-value
Male sex 0.09 (0.07–1.05) 0.055
ARDS 2.34 (0.57–96.76) 0.654
Sepsis 0.20 (0.004–10.67) 0.426
Neurologic disorder 4.65 (0.05–403.10) 0.499
No. of extrapulmonary organ dysfunction 2.89 (1.17–7.11) 0.023 Worst SpO2/FiO2 ratio during hospitalization 0.99 (0.98–1.02) 0.794
Above PEEP* 1.14 (0.93–1.40) 0.200
OR, odds ratio; CI, confidence interval; ARDS, acute respiratory distress syndrome;
SpO2, saturation by pulse oxymeter; FiO2, fraction of inspired oxygen; PEEP, positive end expiratory pressure.
*Difference between peak inspiratory pressure (PIP) and PEEP in the pressure control mode.
사망하여 높은 사망률을 보였다. 그리고 다변량분석에서 폐 외 장 기 부전의 개수가 증가할수록 사망 위험도가 유의하게 증가함을 보였다.
이번 연구의 사망률은 13.7%로, 기저질환이 없는 환자들의 소아 중환자실에 대한 자료는 없어 직접적으로 국내 연구들과 비교하기 어려운 실정이다. 그러나 국내 소아 중환자실의 전체 사망률이 8.5%–14.7%16,17로 보고된 연구들과 비교하면, 호흡보조를 위해 중 환자실에 입실한 경우 기저질환이 없어도 상대적으로 사망률이 낮 지 않았다.
소아 급성폐손상 환자의 사망 위험 인자가 폐 외 다발성 장기 부 전의 개수라는 결과는 다른 연구들에서도 관찰할 수 있다.18-21 미국 의 31개 소아 중환자실의 호흡 부전 연구에서는 폐외 장기 부전이 사망률과 관련 있음을 보였다.19 추후 소아에서 장기 부전 점수 시 스템에 대한 연구가 진행되어 급성폐손상의 중증도에 반영하는 것 이 필요하다는 의견들이 있다.22 이 연구에서는 기존의 연구가 만성 병력이 없는 호흡보조 환자에도 동일하게 적용됨을 보였다. 따라서 이러한 환자에서 장기 부전의 진행을 막고 사망률을 낮추기 위하 여 저산소증이 오래 지속되지 않도록 급성폐손상 환자에서 기계환 기 전략을 잘 세우는 노력과 동시에 다른 장기 기능을 면밀하게 살 펴 적절한 관류를 유지하는 노력도 필요할 것으로 보인다.
이 연구에 포함된 대부분의 환자에서는 폐의 환기-관류의 불균 형이 동반된 것으로 추측되며, 신경질환 환자에서는 호흡 구동(re- spiratory drive) 저하가 주된 기전일 것으로 생각된다. 하지만 중증 환자들의 특성 및 후향적 분석방법을 고려하였을 때 폐활량검사나 폐확산능검사 등 객관적 지표를 이용한 병태생리학적 분류는 시행 할 수 없었다. 따라서 임상적으로 흔히 사용되는 진단명을 이용하 여 호흡부전을 분류하였다. 이 연구의 단변량 분석에서 진단명이
생존자와 사망자에서 유의한 차이를 보였는데 이 중 ARDS가 사망 자의 50%를 차지하였다. ARDS는 직접적 또는 간접적인 다양한 원 인으로 비 균질적인 염증성급성폐손상을 유발하며 저산소증 호흡 부전으로 진행하는 질환이다.23 이번 연구에서는 ARDS 환자의 PaO2/FiO2비 중앙값은 77 (52.5–142.7)로 Berlin 기준24에 따르면 중 증(severe, PaO2/FiO2비<100)에 속하지만, 사망률은 35.7%로 국내 단일 기관들의 ARDS 사망률 37.5%–8.4%21,25,26보다는 낮은 사망 률을 보였다. 높은 중증도를 고려할 때 사망률이 상대적으로 낮았 던 이유는 기관에 따른 차이일 수도 있으나, 기저질환이 없었던 환 자만을 대상으로 한 본 연구의 특징 때문일 수 있다.
이 연구는 소아 및 후향적 연구의 특성상 동맥혈가스 분석을 시행하지 않은 환자들이 많아서 저산소증의 정도에 따른 영향을 평가하기 위해 SpO2/FiO2비를 분석에 추가하였다. SpO2/FiO2비는 이전 연구들에서 소아 급성폐질환에서 PaO2/FiO2비와 같이 호흡 중증도를 나타내는 지표로 사용할 수 있음을 보였다.27-29 Pediatric Acute Lung Injury Consensus Conference Group22에서도 비 침습 적인 환기 치료하는 환자의 ARDS 진단 기준에 SpO2/FiO2비를 포 함시켰다. 이 연구에서 기계 호흡 치료 받은 군이 비침습적 호흡기 치료 받은 군보다 SpO2/FiO2비가 유의하게 낮아 저산소증의 중증 도 차이가 있음을 알 수 있었다. 생존자군과 비생존자군의 SpO2/ FiO2 비를 비교했을 때 통계적으로 의미 있는 차이를 보였으나 다 변량 분석에서는 유의한 사망의 위험 인자로 나타나지 않았다. 소 아 중환자실에서 SpO2/FiO2비와 사망률의 연관성을 보인 연구는 있지만30 단일 기관이며 후향적 연구이기 때문에 이에 대한 추가적 인 연구가 필요할 것으로 보인다.
이 연구의 단변량 분석에서 성별의 차이가 생존자와 비생존자의 비교 분석에서 의미 있게 나타났다. 성별 차이에 따른 진단명을 확 Table 4. Clinical characteristics of nonsurvivors
Subject Age (yr) Sex Diagnosis Pathogen PRD
(%) ICU duration (day)
Number of extrapulmonary
organ failure
Worst SpO2/FiO2
during hospitalization
Highest above PEEP during
hospitalization Other treatments
1 3 F ARDS Unknown 2.29 73 2 176 20
2 2 M ARDS RSV 8.87 32 3 79 21 Veno-venous ECMO
3 4 M Encephalitis HSV, mycoplasma 1.03 29 3 223 26
4 0 F ARDS Unknown 12.83 44 1 38 29
5 4 F Septic shock Enterovirus 20.54 2 1 84 28
6 0 F Encephalitis Unknown 0.46 8 1 457 12
7 0 F ARDS Unknown 7.69 19 1 81 19 Veno-venous ECMO
8 1 F Septic shock HSV 36.65 9 5 7 22
9 10 M ARDS Unknown 5.54 99 4 158 12 Veno-venous ECMO,
Lung transplantation
10 2 F Reye syndrome Influneza B 56.39 5 5 253 22
PRD, probability of death calculated by Pediatric Index of Mortality 3 score; ICU, intensive care unit; SpO2, saturation by pulse oxymeter; FiO2, fraction of oxygen; PEEP, positive end expiratory pressure; ARDS, acute respiratory distress syndrome; RSV; respiratory syncytial virus; ECMO, extracorporeal membrane oxygenation; HSV, herpes simplex virus.
인했을 때 남자가 사망자가 없었던 폐렴과 폐쇄성기도질환의 빈도 가 여자보다 의미 있게 높았다. 이와 같은 원인 질환의 차이 때문에 남자가 상대적으로 사망률이 낮게 나왔던 것으로 보인다. 소아 중 환자실에서 성별의 차이가 사망 위험 인자일 가능성을 보여준 연 구는 있지만31,32 최근에는 성별과 직접적인 연관성을 찾기 힘들다 는 연구가 더 많았다.4,20,33 이번 연구에서는 비생존자의 수가 적었 고 다른 인자들을 보정했을 때는 성별의 차이에서 통계적인 유의성 이 나타나지 않아 성별이 여자일 때 사망 위험 인자라고 하기에는 한계가 있다.
생존자와 비생존자의 기계 환기 지표들을 단변량 분석하였을 때 above PEEP이 유의한 차이를 보였다. 성인의 급성폐손상에서는 낮 은 일회 호흡량(low tidal volume), 높은 PEEP이 생존율을 높인다 는 보고34가 있지만 소아에서의 데이터는 아직 부족한 실정이다. 이 연구 대상들의 데이터를 분석했을 때 pressure control mode를 주 로 사용하였고, above PEEP으로 일회 호흡량을 조절하였다. 최근 Amato 등35의 연구에서는 성인의 9개 급성호흡곤란증후군 임상 연구들을 multilevel mediation analysis를 시행하였는데, 일회 환 기량, 호기말양압 등의 단일 지표보다 실제적인 기능적 폐용량을 반영하는 ‘driving pressure’ (ΔP =VT/CRS; VT, tidal volume;
CRS, respiratory-system compliance)가 사망률과 유의한 상관관 계가 있다고 보고하였다. Driving pressure값은 환자의 자발적인 흡 기 노력이 없을 때 plateau pressure와 PEEP차이인 측정값이므로 이 연구의 기계환기 설정 값인 above PEEP과는 약간의 차이가 있 다. 하지만 above PEEP값이 사망한 환아에서 의미 있게 높았던 이 번 연구의 결과는 pressure control mode를 사용하는 소아 중환자 실에서 low tidal volume lung protective strategy로 적용해 볼 수 있 다는 점에서 의미가 있을 수 있다. 그러나 이 연구에서는 동일한 질 환에 동일한 진료지침으로 적용한 값이 아니어서 중증도의 결과로 해석할지 결과에 영향을 주는 원인으로 해석할지에 대한 구분이 어려울 것으로 보이며, 다변량 분석에서도 유의한 차이를 보이지 않았다. 따라서 이에 대한 해석은 추가적인 연구가 필요할 것으로 보인다.
이번 연구는 몇 가지 제한점을 가지고 있다. 첫째, 단일 기관에서 시행한 연구이기 때문에 제한된 수의 환자를 대상으로 연구하였 다. 둘째, 기저질환이 없는 환자가 전체 소아 중환자 입원의 1.5%밖 에 되지 않아 삼차 의뢰 기관의 특성이 연구 결과에 반영되어 선택 적 편향이 있을 수 있다. 셋째, 후향적으로 의무기록을 보고 연구하 였기 때문에 호흡기질환의 중증도를 나타내는 지표가 제한적이며, 사망과 관련된 위험 인자들은 사망 지표일 수는 있으나 인과관계 로 확인하기는 어렵다. 넷째, 이 연구는 가습기세정제연관 폐손상 이 있었던 기간(2006년부터 2011년)이 포함되어 있다. 관련 코호트 연구36에 따르면 기저질환이 없었던 아이들이 89.9%이고 중환자실 에서 침습적 기계환기를 56.5% 환자가 적용하였으므로 이 연구 대
상자에도 가습기세정제연관 폐손상의 환자가 포함되었을 가능성 이 있으나 의무기록으로는 확인할 수 없었다.
결론적으로 만성질환 없이 건강하게 지내던 소아가 호흡보조를 위해 중환자실에 입원한 경우 사망률은 13.7%로 보호자에게 양호 한 예후로 설명되기 어려움을 보였다. ARDS가 동반되지 않은 폐렴 이나 기도폐쇄성질환의 경우 사망은 없었으나, 폐 이외에 동반된 장 기 부전의 개수가 증가할수록 사망의 위험은 증가하였다. 향후 만 성병력이 없이 호흡보조를 위해 중환자실에 입실한 소아의 경과 및 예후에 대한 다기관 연구가 필요할 것으로 보인다.
REFERENCES
1. Carville KS, Lehmann D, Hall G, Moore H, Richmond P, de Klerk N, et al. Infection is the major component of the disease burden in aboriginal and non-aboriginal Australian children: a population-based study. Pedi- atr Infect Dis J 2007;26:210-6.
2. Crow SS, Undavalli C, Warner DO, Katusic SK, Kandel P, Murphy SL, et al. Epidemiology of pediatric critical illness in a population-based birth cohort in Olmsted County, MN. Pediatr Crit Care Med 2017;18:e137-45.
3. Namachivayam P, Shann F, Shekerdemian L, Taylor A, van Sloten I, Del- zoppo C, et al. Three decades of pediatric intensive care: who was admit- ted, what happened in intensive care, and what happened afterward. Pe- diatr Crit Care Med 2010;11:549-55.
4. Erickson S, Schibler A, Numa A, Nuthall G, Yung M, Pascoe E, et al.
Acute lung injury in pediatric intensive care in Australia and New Zea- land: a prospective, multicenter, observational study. Pediatr Crit Care Med 2007;8:317-23.
5. Randolph AG, Meert KL, O'Neil ME, Hanson JH, Luckett PM, Arnold JH, et al. The feasibility of conducting clinical trials in infants and chil- dren with acute respiratory failure. Am J Respir Crit Care Med 2003;167:
1334-40.
6. Barreira ER, Munoz GO, Cavalheiro PO, Suzuki AS, Degaspare NV, Shieh HH, et al. Epidemiology and outcomes of acute respiratory distress syndrome in children according to the Berlin definition: a multicenter prospective study. Crit Care Med 2015;43:947-53.
7. Edwards JD, Houtrow AJ, Vasilevskis EE, Rehm RS, Markovitz BP, Gra- ham RJ, et al. Chronic conditions among children admitted to U.S. pedi- atric intensive care units: their prevalence and impact on risk for mortali- ty and prolonged length of stay. Crit Care Med 2012;40:2196-203.
8. Spaeder MC, Custer JW, Bembea MM, Aganga DO, Song X, Scafidi S. A multicenter outcomes analysis of children with severe viral respiratory infection due to human metapneumovirus. Pediatr Crit Care Med 2013;
14:268-72.
9. Randolph AG, Reder L, Englund JA. Risk of bacterial infection in previ- ously healthy respiratory syncytial virus-infected young children admit- ted to the intensive care unit. Pediatr Infect Dis J 2004;23:990-4.
10. Wong KK, Jain S, Blanton L, Dhara R, Brammer L, Fry AM, et al. Influ- enza-associated pediatric deaths in the United States, 2004-2012. Pediat- rics 2013;132:796-804.
11. Byington CL, Wilkes J, Korgenski K, Sheng X. Respiratory syncytial virus- associated mortality in hospitalized infants and young children. Pediat- rics 2015;135:e24-31.
12. Nizam M, Norzila MZ. Stress among parents with acutely ill children.
Med J Malaysia 2001;56:428-34.
13. Bartel DA, Engler AJ, Natale JE, Misra V, Lewin AB, Joseph JG. Working
with families of suddenly and critically ill children: physician experienc- es. Arch Pediatr Adolesc Med 2000;154:1127-33.
14. Bernard GR, Artigas A, Brigham KL, Carlet J, Falke K, Hudson L, et al.
The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994;149(3 Pt 1):818-24.
15. Goldstein B, Giroir B, Randolph A; International Consensus Conference on Pediatric Sepsis. International pediatric sepsis consensus conference:
definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med 2005;6:2-8.
16. Lee OJ, Jung M, Kim M, Yang HK, Cho J. Validation of the Pediatric In- dex of Mortality 3 in a single pediatric intensive care unit in Korea. J Ko- rean Med Sci 2017;32:365-70.
17. Hwang HS, Lee NY, Han SB, Kwak GY, Lee SY, Chung SY, et al. Perfor- mance effectiveness of pediatric index of mortality 2 (PIM2) and pedi- atricrisk of mortality III (PRISM III) in pediatric patients with intensive care in single institution: Retrospective study. Korean J Pediatr 2008;51:
1158-64.
18. Panico FF, Troster EJ, Oliveira CS, Faria A, Lucena M, João PR, et al. Risk Factors for Mortality and Outcomes in Pediatric Acute Lung Injury/Acute Respiratory Distress Syndrome. Pediatr Crit Care Med 2015;16:e194-200.
19. Weiss SL, Asaro LA, Flori HR, Allen GL, Wypij D, Curley MA, et al. Mul- tiple organ dysfunction in children mechanically ventilated for acute re- spiratory failure. Pediatr Crit Care Med 2017;18:319-29.
20. Flori HR, Glidden DV, Rutherford GW, Matthay MA. Pediatric acute lung injury: prospective evaluation of risk factors associated with mortal- ity. Am J Respir Crit Care Med 2005;171:995-1001.
21. Kang SS, Pae RM, Lee EK, Bang KW, Kim HS, Chun YH, et al. Outcome of acute respiratory distress syndrome in children: a single center study.
Allergy Asthma Respir Dis 2014;2:266-71.
22. Pediatric Acute Lung Injury Consensus Conference Group. Pediatric acute respiratory distress syndrome: consensus recommendations from the Pediatric Acute Lung Injury Consensus Conference. Pediatr Crit Care Med 2015;16:428-39.
23. Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med 2000;342:1334-49.
24. ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, et al. Acute respiratory distress syndrome: the Berlin definition. JAMA 2012;307:2526-33.
25. Kim SY, Kim YH, Sol IS, Kim MJ, Yoon SH, Kim KW, et al. Application of the Berlin definition in children with acute respiratory distress syn- drome. Allergy Asthma Respir Dis 2016;4:257-63.
26. Ko JM, Ha EJ, Lee EH, Lee SY, Kim HB, Hong SJ, et al. Clinical outcome and prognostic factors of acute respiratory distress syndrome in children.
Korean J Pediatr 2005;48:599-605.
27. Khemani RG, Thomas NJ, Venkatachalam V, Scimeme JP, Berutti T, Schneider JB, et al. Comparison of SpO2 to PaO2 based markers of lung disease severity for children with acute lung injury. Crit Care Med 2012;
40:1309-16.
28. Lobete C, Medina A, Rey C, Mayordomo-Colunga J, Concha A, Menén- dez S. Correlation of oxygen saturation as measured by pulse oximetry/
fraction of inspired oxygen ratio with Pao2/fraction of inspired oxygen ratio in a heterogeneous sample of critically ill children. J Crit Care 2013;
28:538.e1-7.
29. Rice TW, Wheeler AP, Bernard GR, Hayden DL, Schoenfeld DA, Ware LB, et al. Comparison of the SpO2/FIO2 ratio and the PaO2/FIO2 ratio in patients with acute lung injury or ARDS. Chest 2007;132:410-7.
30. Ghuman AK, Newth CJ, Khemani RG. The association between the end tidal alveolar dead space fraction and mortality in pediatric acute hypox- emic respiratory failure. Pediatr Crit Care Med 2012;13:11-5.
31. DeBruin W, Notterman DA, Magid M, Godwin T, Johnston S. Acute hy- poxemic respiratory failure in infants and children: clinical and patho- logic characteristics. Crit Care Med 1992;20:1223-34.
32. Nichols DG, Walker LK, Wingard JR, Bender KS, Bezman M, Zahurak ML, et al. Predictors of acute respiratory failure after bone marrow trans- plantation in children. Crit Care Med 1994;22:1485-91.
33. Zimmerman JJ, Akhtar SR, Caldwell E, Rubenfeld GD. Incidence and outcomes of pediatric acute lung injury. Pediatrics 2009;124:87-95.
34. Petrucci N, De Feo C. Lung protective ventilation strategy for the acute respiratory distress syndrome. Cochrane Database Syst Rev 2013;(2):
CD003844.
35. Amato MB, Meade MO, Slutsky AS, Brochard L, Costa EL, Schoenfeld DA, et al. Driving pressure and survival in the acute respiratory distress syndrome. N Engl J Med 2015;372:747-55.
36. Kim KW, Ahn K, Yang HJ, Lee S, Park JD, Kim WK, et al. Humidifier disinfectant-associated children's interstitial lung disease. Am J Respir Crit Care Med 2014;189:48-56.