Introduction
The meniscus plays an important multifunctional role in main
taining the overall function of the knee, which involves load transmission, shock absorption, joint stability and lubrication, proprioception, and nutrient supply
1,2). Injuries involving detach
ment of the meniscus affect meniscal biomechanics and kinemat
ics, leading to accelerated degenerative changes within the knee joint. In particular, posterior root tears of the medial meniscus (PRTMM) have recently become a recognized issue, as a root tear destroys the ability of the meniscus to withstand hoop tension.
PRTMM is considered a radial tear or avulsion at the insertion of the medial meniscus, and it often may go unnoticed
3). This pathology may cause medial meniscus extrusion, loss of articular cartilage, and joint space narrowing, and it eventually progresses to medial compartment degenerative osteoarthritis
49). Hence, there has been an increasing interest in the surgical repair of tears at the meniscal root
3,9,1016).
High tibial osteotomy (HTO) was originally devised to treat medial compartment osteoarthritis of the knee with varus de
formity. Decreasing the pressure on the medial compartment by altering the weightbearing axis may lead to remodeling of the
Clinical and Radiological Results with SecondLook Arthroscopic Findings after Open Wedge High Tibial Osteotomy without Arthroscopic Procedures for Medial Meniscal Root Tears
Hyun Il Lee, MD, Dongjun Park, MD, and Jinho Cho, MD, PhD
Department of Orthopedic Surgery, Inje University Ilsan Paik Hospital, Goyang, Korea
Purpose: To identify the structural integrity of the healing site after medial open wedge high tibial osteotomy (MOWHTO) in patients with a
posterior root tear of the medial meniscus (PRTMM) and chondral lesion by secondlook arthroscopy and to determine the clinical and radiological findings.
Materials and Methods: From August 2010 to June 2016, 52 consecutive patients underwent MOWHTO and arthroscopic examination without a
chondral resurfacing procedure and meniscal treatment for PRTMM. Twentyfour patients were available for secondlook arthroscopic evaluation.
The mean followup period was 19.5 months (range, 5 to 46 months). Clinical evaluation was based on the Lysholm knee scores and Hospital for Special Surgery (HSS) scores.
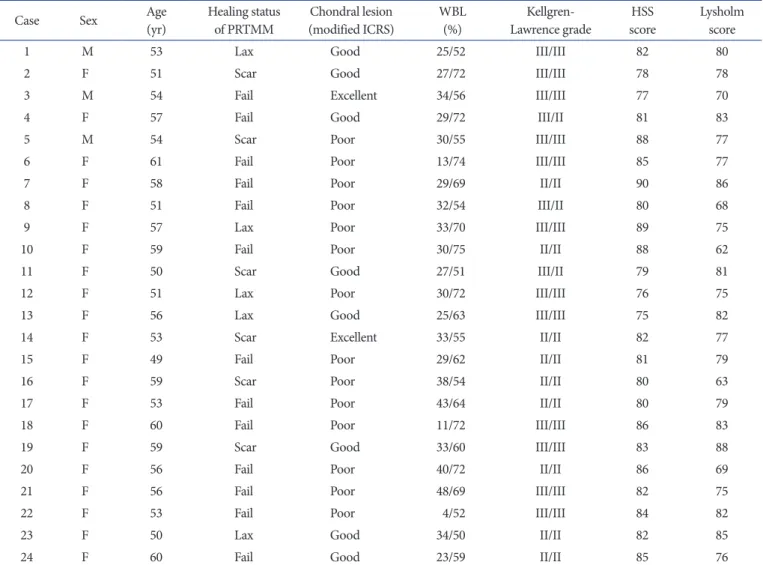
Results: There were 5 lax healing, 6 scar tissue, 13 failed healing of PRTMM. Definite change of chondral lesion was not observed. The Kellgren
Lawrence grade did not improve according to the followup plain radiograph. The mean Lysholm score improved from 34.7 preoperatively to 77.1 at the last followup, and the mean HSS score significantly increased from 36.5 to 82.4.
Conclusions: This study revealed a low rate of healing potency of PRTMM and chondral lesion after MOWHTO without any attempt for meniscal
treatment or chondral resurfacing. The cartilage and healing status of PRTMM was not associated with improved clinical outcomes and radiological findings.
Keywords: Knee, Osteoarthritis, Medial meniscus, Root tear, Osteotomy, Open wedge pISSN 2234-0726 · eISSN 2234-2451
Knee Surgery & Related Research
Received June 4, 2017; Revised (1st) September 18, 2017;
(2nd) November 3, 2017; Accepted December 11, 2017 Correspondence to: Jinho Cho, MD, PhD
Department of Orthopedic Surgery, Inje University Ilsan Paik Hospital, 170 Juhwaro, Ilsanseogu, Goyang 10380, Korea
Tel: +82319107301, Fax: +82319107967 Email: [email protected]
34
This is an Open Access article distributed under the terms of the Creative Commons Attribution NonCommercial License (http://creativecommons.org/licenses/bync/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Copyright © 2018 KOREAN KNEE SOCIETY
www.jksrr.org
articular cartilage
17). However, few articles have reported that regeneration of the articular cartilage is associated with clinical improvement. Furthermore, the specific factors influencing carti
lage regeneration remain unclear.
A recent study showed that reducing contact stress using HTO can heal PRTMM
18). Nha et al.
19)found that high tibial corrective osteotomy in patients with combined PRTMM and varus defor
mity resulted in acceptable clinical improvements in 20 patients.
Furthermore, 10 of these patients showed complete repair during a secondlook arthroscopic examination, while 6 showed incom
plete repair. However, this study was unable to determine the exact healing mechanism of PRTMM.
The objectives of the present study were as follows: 1) to assess the structural integrity of the meniscal healing site and determine articular cartilage status using secondlook arthroscopy; and 2) to evaluate the clinical relevance of these findings after medial open wedge high tibial osteotomy (MOWHTO).
Materials and Methods
1. Patient Selection and Study Design
This was a retrospective study approved by the institution’s ethi
cal review committee (Institutional Review Board No. ISPAIK 201609004001). Fiftytwo MOWHTOs were performed. The study group comprised 52 patients (7 males and 45 females) with varus deformities who were surgically treated for medial compartment osteoarthritis or PRTMM. The procedures took place in our hospital from August 2010 to June 2016, and all procedures were performed by the same orthopedic surgeon. All the patients presented with pain on the medial side of the knee.
Weight bearing anteroposterior radiographs were taken in each case, and all knees showed varus deformities with medial joint space narrowing. The progression of osteoarthritis was evaluated by using the KellgrenLawrence radiographic grading scale.
Among 52 consecutive patients, 24 underwent secondlook arthroscopy, and they were enrolled in this study. Data were ana
lyzed, including information obtained from reviewing medical records and arthroscopic findings. Secondlook arthroscopy was performed in 23 patients following hardware removal upon the patient’s request 1 year following surgery.
2. Exclusion Criteria
Patients with a history of injury, tibial fracture, chronic instabil
ity of the knee, infection of the knee, severe osteoarthritis of the patellofemoral joint, femorotibial angle (FTA) more than 185°
(5° of anatomic varus), or flexion contracture more than 15° were
excluded from the study.
3. Surgical Technique
Preoperative planning included determination of the desired correction using fulllength standing radiographs according to the method of Miniaci. The mechanical axis was shifted to a point 62% lateral on the transverse diameter of the tibial plateau according to the criteria of Fujisawa.
The procedure was performed under general or spinal anes
thesia with the patients placed in a supine position on a radiolu
cent standard operating table a with lateral support. Initial knee arthroscopy was first performed on every patient to evaluate cartilage status and meniscal injury. The joint surface was not treated in any patient. An oblique incision 60 mm to 80 mm long, 40 mm distal to the joint line, and 10 mm proximal to the pes anserinus was made, extending from the medial aspect of the tibial tuberosity to the posterior border of the tibial plateau.
The semitendinosus and gracilis tendons were cut at the point of tibial insertion; medial collateral ligaments were released from the posteromedial cortex of the tibia; and a Hohmann retractor was inserted to protect the neurovascular structures. The first oblique osteotomy was started at the upper margin of the pes anserinus (approximately 35 mm distal to the medial proximal tibial joint surface), and it ended 10 mm from the lateral cortical margin at the upper level of the proximal tibiofibular joint. The second frontal osteotomy was started 10 mm or more proximal to the insertion of the patellar tendon to the first osteotomy plane (biplanar osteotomy). These osteotomy procedures were performed with a micro bone saw and completed with the use of chisels. The osteotomy site was opened by insertion of a specially designed bone spreader at a distance determined by a goniom
eter under fluoroscopic control. Alignment was checked using the rod method. The tibial slope was not changed. A TomoFix plate (DePuy Synthes, West Chester, PA, USA) was inserted into a subcutaneous tunnel over the soft tissues on the anteromedial aspect of the tibia and fixed in place with 8 locking screws with minimal invasiveness. Artificial bone graft materials (Btricalcium phosphate wedges [GeneX, Biocomposites Ltd., Staffordshire, UK] and ChronOS [DePuy Synthes]) were used to form a trian
gular pole equivalent to the size of the opening, and then it was inserted into the osteotomy site (Fig. 1).
4. Radiological Evaluation
Radiological evaluations of the mechanical FTA were per
formed using an anteroposterior weightbearing radiograph
taken with the knee joint in extension at 3 months and 1 year
postoperatively, and at the final followup examination. A weight bearing line (WBL) percentage was calculated using standing longcassette radiographs of the lower extremities. The WBL was determined by drawing a line from the center of the femoral head to the middle point of the proximal talar joint surface. Then, the WBL percentage was calculated as the horizontal distance from the WBL to the medial edge of the tibial plateau, divided by the width of the tibial plateau (Fig. 2A and B).
5. Postoperative Rehabilitation
For the first 6 postoperative weeks, patients were allowed to perform toetouch weight bearing using 2 crutches and a brace.
After removing the drains on the second postoperative day, active physical therapy with strengthening exercises and continuous passive motion was initiated. After 6 weeks, patients began full weight bearing. Return to normal sporting activities, including jogging, was permitted at 6 months postoperatively.
6. Second-Look Arthroscopic Findings
Healing status of the repaired meniscus was classified according to the method of Seo et al.
9)(complete healing, lax healing, scar tissue healing, or failed healing). Complete healing was defined as meniscal continuity with no cleft, no lifting on probing, and normal meniscal tension at the repair site (Fig. 3). Lax heal
ing was defined as an apparent increase in meniscus lifting and mobility on probing with good meniscal continuity. Scar tissue healing was defined as a meniscus that could be easily raised on A
B C
Fig. 1. Stabilization of open wedge in high tibial osteotomy. (A) After medial open wedge high tibial osteotomy and fixation of Tomofix (DePuy Synthes). (B) Artifical bone graft (ChronOS, DePuy Synthes). (C) Artifi
cal bone graft (GeneX, Biocomposites Ltd.).
A B
A A
B B A' A' B B