□Original Article□
Vol. 15. No. 1, 2012
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Laparoscopic Primary Closure: A Better Method of Treatment in Perforated Peptic Ulcer Disease than Open Repair
Gyou Ra Lee, M.D., Jong Kyung Park, M.D., Sung Geun Kim, M.D., Seung Hye Choi, M.D., Sang Seob Yun, M.D., Seong Lee, M.D., Hee Yong Kwak, M.D.
Department of Surgery, St. Paul’s Hospital, The Catholic University of Korea, College of Medicine, Seoul, Korea Purpose: Perforation is a dreadful complication of peptic
ulcer disease requiring immediate management. This study examined the feasibility of laparoscopic primary closure in perforated peptic ulcer disease to allow an earlier return to normal life.
Methods: This study reviewed our experience retrospectively with 72 consecutive patients treated with the simple closure of a perforated peptic ulcer disease in our hospital from December 2002 to January 2011. Thirty five patients were treated laparoscopically and the rest underwent open surgery.
The operative time, nasogastric tube utilization, abdominal drain usage, time to oral feeding, hospital stay, postoperative complications and recurrence in both groups were compared.
A student’s t-test was used to make the comparisons. A p value<0.05 was considered significant.
Results: The operative time, use of nasogastric tubes, and abdominal drainage were similar in both groups. After laparoscopic surgery, the patients showed an earlier return to normal oral feeding and discharge than the open surgery group (4.17±0.62 vs. 5.03±2.34 days, p=0.040, 8.63±1.96 vs. 10.24±3.59 days, p=0.021, respectively). The decreased handling of tissue in laparoscopic surgery led to less wound infection (0 in laparoscopic surgery vs. 3 in open) and postoperative ileus (0 vs. 2).
Conclusion: Laparoscopic repair of a perforated peptic ulcer is a safe and feasible treatment that offers early oral feeding and a shorter postoperative hospital stay.
Key words: Laparoscopy, Primary closure, Peptic ulcer, Perforation
Received July 20, 2011, Revised October 24, 2011, Accepted November 18, 2011
※ Corresponding author:Hee Yong Kwak
Department of Surgery, St. Paul’s Hospital, The Catholic University of Korea, College of Medicine, Jeonnong-dong, Dongdaemoon-gu, Seoul 130-709, Korea
Tel: +82-2-958-2135, Fax: +82-2-958-2316 E-mail: [email protected]
INTRODUCTION
Complications of peptic ulcer disease such as perforation still occur in a number of patients and result in main cause of death in patients with comorbidities. Therefore emergent correction is required.
H. pylori infection is the most common known cause of peptic ulcer and accounts for the majority of cases. NSAIDs are the second most common cause and are responsible for the majority of ulcers not caused by H. pylori infection.1,2 Introduction of various medications including proton pump inhibitor (PPI) led to decline in uncomplicated peptic ulcer disease.3
Treatment options of perforated peptic ulcer are various from minimal invasive treatment to immediate definitive radical ulcer surgery. Even some patients with perforated ulcer can be managed successfully by nonoperative means.4 However, in
many cases the uncertainty of the exact underlying pathology and diagnosis can deter from this line of management.5 Nowadays, primary closure of the perforation remains an attractive option for perforated peptic ulcer in most centers.6 Many reports of laparoscopic treatment have shown that peritoneal lavage can be done effectively and perforation can be cured safely.7-11 Moreover, randomized trials showed some advantages of laparoscopic repair compared with conventional open repair regarding to shorter operating time, less postoperative pain, reduced postoperative hospital stay, and earlier return to normal daily activities.12
In this retrospective study, we evaluated whether or not laparoscopic surgery of perforated peptic ulcer offers patients an improved outcome compared with conventional open repair.
MATERIALS AND METHODS
This study is reviewed retrospectively. All patients who underwent emergent operation admitted by emergency department in St. Paul’s hospital, the Catholic University of Korea, College of Medicine with a clinical diagnosis of perforated peptic ulcer from December 2002 to January 2011 were included. Patient underwent laparoscopic or open repair depending on the favor of surgeons. Two surgeons were involved in the study, one of whom had a laparoscopic interest and was regularly performing
Fig. 1. The locations of trochars in abdominal wall.
laparoscopic procedures since the year of 2006.
Surgery was performed under general anesthesia. All patients received 1.0 g of cefuroxime at the time of initial diagnosis and nasogastric tube was placed. Surgery was performed soon shortly after the clinical diagnosis.
1) The laparoscopic repair
The laparoscopic repair was performed as follows:13 the operating surgeon stood on the left side of the patient. 3 ports were used. The Hassan method was used for insertion of 11-mm supraumbilical optical port. A 30-degree laparoscope was used in all cases. One operating port was placed in the Rt. mid clavicular line. An additional 11-mm port was used to facilitate suturing at the Lt. para-epigastric area. Fig. 1 shows the location of ports on the abdominal wall.
Intracorporeal oversewing was done through the duodenum or stomach near the site of perforation, and then a mobilized omental patch was tied. An intracorporeal knot was tied. The omental patch was fixed over the perforation site where additional sutures were passed to close the perforation.
Vigorous peritoneal irrigation with normal saline was followed.
2) The open repair
The open repair is well described in standard textbooks.5,6 Through an upper midline incision, a piece of omentum was fixed down under an arch of full thickness absorbable sutures placed on either side of the perforation and then the sutures were tied. Peritoneal irrigation was followed.
3) Perioperative and postoperative care
Postoperatively, patients were given pantoprazole 40 mg (proton pump inhibitor) via intravenous infusion and 500 mg of metronidazole.
Nasogastric tube was removed when drainage from tube was less than 200 ml/24 hours. Abdominal drains were removed when output was less than 50 ml/24 hours. Oral fluids were introduced upon patients’ request only after removal of nasogastric tube. All surgeons followed the above protocols. Patients were given 1.0 g cefuroxime every 12 hours and 500 mg metronidazole every 8 hours. Reintroduction of drinking water implicates the ability to tolerate a hospital diet. The length of hospital stay was the number of days after surgery (day 0).
Operative time, estimated blood loss, time of nasogastric tube utilization, abdominal drain usage, time to oral feeding, hospital stay, and postoperative complications of both group were compared. Omentopexy was done in some circumstances.
Student’s t-test was conducted to verify and p<0.05 was considered statistically significant.
RESULTS
110 consecutive patients who visited emergency department in our hospital between December 2002 and January 2011 were reviewed. A total of 73 patients were included in the study and the rest who underwent radical ulcer surgery (eg. Vagotomy with antrectomy) were excluded in this study.
1) Comparison of clinical outcome between open and lapa- roscopic repair group
Table 1 shows the demographics of the patients included in the study. 35 patients underwent laparoscopic repair, and the remaining 37 conventional open repair. The male: female ratio was 10.67 vs. 8.25. The patients of open repair group had a mean age of 45.2 (range, 19∼83) years and that of laparoscopy 47.4 (range, 24∼83). Mean duration of history of both groups were 1.46 vs. 1.57 days. The majority of ulcers were noted to be duodenal (79.5%). Median size of perforation was 5 mm in both groups. In the laparoscopic group, no patients required intraoperative or perioperative conversion to open surgery.
2) Perioperative and postoperative outcomes between open and laparoscopic repair group
Table 2 shows data of perioperative and postoperative outcomes. The total operative time and estimated blood loss for laparoscopic repair of perforated peptic ulcer disease were
Table 1. Comparison of clinical outcome between open and laparoscopic repair group
Laparoscopic Open
No. of patients 35 37
Male 32 (91%) 33 (89%)
Female 3 (9%) 4 (11%)
Mean age (years) 47.4 (24∼83) 45.2 (19∼83) Mean duration 1.46 (1∼7) 1.57 (1∼10) of history (days)
Site of ulcer
Duodenal 28 (80%) 29 (78%)
Stomach 7 (20%) 8 (22%)
Median size of 5 (2∼20) 5 (2∼20) perforation (mm)
Table 3. Comparisons of postoperative complications between open and laparoscopic repair group
Laparoscopic Open
No. of patients 35 37
Wound infection 0 3
Pneumonia 1
Atelectasis 1*
Other lung disease 1‡ 1†
Ileus 2
Others 1§
Overall morbidity 3/35 (8.6%) 7/37 (18.9%)
*Pancreatitis was accompanied; †Spontaneous pneumothorax;
‡Pulmonary edema; §Herpes zoster was aggrevated during the hospital day.
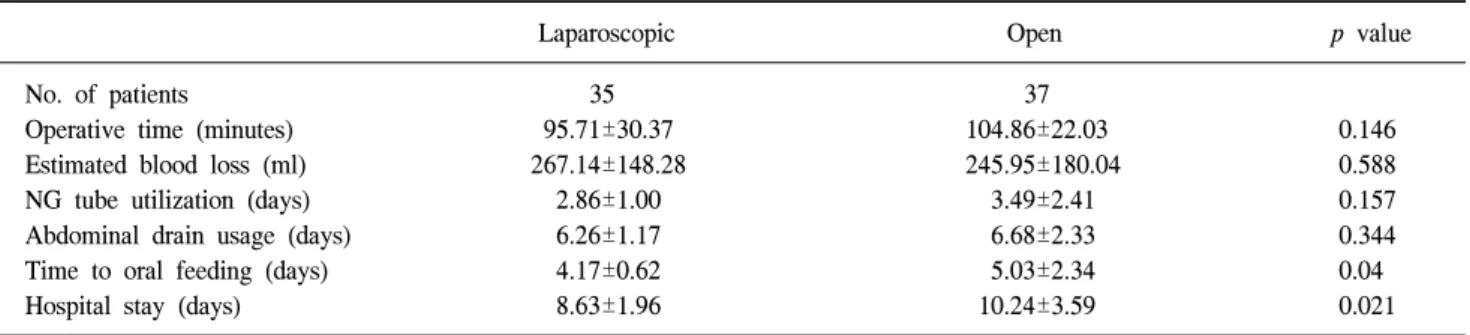
Table 2. Perioperative and postoperative outcomes between open and laparoscopic repair group
Laparoscopic Open p value
No. of patients 35 37
Operative time (minutes) 95.71±30.37 104.86±22.03 0.146
Estimated blood loss (ml) 267.14±148.28 245.95±180.04 0.588
NG tube utilization (days) 2.86±1.00 3.49±2.41 0.157
Abdominal drain usage (days) 6.26±1.17 6.68±2.33 0.344
Time to oral feeding (days) 4.17±0.62 5.03±2.34 0.04
Hospital stay (days) 8.63±1.96 10.24±3.59 0.021
Table 4. Recurrence of peptic ulcer complications in open and laparoscopic repair groups
Laparoscopic Open
No. of patients
Bleeding 1 2
Perforation 1
Aggravation of ulcer 1 2
Others 1*
*Discomfort due to bloating because of dilatation of stomach without any other complications.
comparable to open surgery (95.71±30.37 [SD] vs. 104.86±22.03 minutes, vs. 267.14±148.28 [SD] vs. 245.95±180.04 ml, respec- tively). Patients who underwent laparoscopic repair required nasogastric tubes and abdominal drainage for much the same time during the postoperative period (2.86±1.00 [SD] vs.
3.49±2.41 days, 6.26±1.17 [SD] vs. 6.68±2.33 days, respectively).
Patients were able to return to normal oral feeding significantly earlier if they had undergone laparoscopic repair (4.17±0.62 [SD] vs. 5.03±2.34 days, p=0.040).
3) Comparisons of postoperative complications between open and laparoscopic repair group
Table 3 shows the postoperative complications that are reduced when surgery was performed laparoscopically. Wound infected patients were 3 in open group and 0 in laparoscopic group. Those who experienced postoperative ileus were 0 vs.
2. Pneumonia, spontaneous pneumothorax occurred in open closure group and atelectasis, pulmonary edema in laparoscopic repair. Overall morbidity was 3/35 (0.086) vs. 7/37 (0.189).
4) Recurrence of peptic ulcer complications in open and laparoscopic repair groups
Table 4 shows the recurrence of peptic ulcer disease after the patient returned to normal life. Clinical course of peptic ulcer itself is not influenced statistically by method of operation (open vs. laparoscopic). However, 1 of 37 open patients experienced recurrence of perforated peptic ulcer after 18
months and no one in laparoscopic group. 2 patients of open group underwent bleeding after 10 days and 4 years respectively and only 1 experienced bleeding after 45 days in laparoscopy. Overall recurrence was 3/35 (0.086) vs. 5/37 (0.135).
DISCUSSION
Perforated peptic ulcer disease needs immediate surgical intervention within 24 hours since the onset. There are various methods including definitive radical ulcer surgery (eg.
Vagotomy with antrectomy) and simple closure. There has been a great advance in development of medications, such as H2-antagonists and proton pump inhibitors, in eradiating Helicobacter pylori.14,15 More than 90% of perforated peptic ulcer can be treated with only simple closure due to such medications.16 Laparoscopic simple closure has been performed in many centers since Nathanson et al.,7 1990 and Mouret et al.,9 1990 first reported their cases. It is now believed that radical ulcer surgery is not required but it is rather equivocal to simple closure and irradiating Helicobacter pylori with medication.17
This study was performed retrospectively. Therefore, the re- sult has some limits for representing all circumstances.
However, it is aimed to find out better outcomes in laparos- copic repair of perforated peptic ulcer than open simple closure.
Primary advantage of primary closure is its minimal invasive- ness which allows less tissue damage. Therefore, laparoscopic repair can be favorable even in septic condition due to peritonitis. Poor general condition of the patient is a factor which makes surgeon to hesitate whether the patient should get operation or not. With minimal invasive technique, the patient is less exposed to harmful handling.
However, it is quite difficult to learn laparoscopic technique.
Earlier randomized studies showed that the laparoscopic repair took longer operation time,18 which means higher costs. Median operative time was 105 minutes in open vs. 90 in laparoscopy according to our study. This study includes our initial experience in laparoscopy and laparoscopic repair requires more technique. It is of no significance but less time is needed in laparoscopy. Major disadvantage of laparoscopic repair is that specific training in laparoscopic suturing technique is needed and this handling is associated with surgeon’s experience. Only efforts in learning practice of laparoscopy offer shorter operativ e time and patient’s safety. In addition, there are different methods of ulcer closure introduced other than suturing, such as gelatin sponge and fibrin glue18,19 and stapled omental patch
repair.20,21 These methods are easier to perform and contribute to shorten operative time.
There was no statistical significance in hospital stay and time to normal diet in previous studies of Johansson et al,22 1996, Lau et al.,18 1996, Miserez et al.,23 1996, Druart et al.,24 1997, Bergamaschi et al.,25 1999, and Lee et al.,26 2009. However, our patients who underwent laparoscopic repair were enabled to be discharged significantly earlier from the hospital (8.63±1.96 [SD] vs. 10.24±3.59 days, p=0.021). In addition, more recent randomized, controlled trials have shown that lapa- roscopic repair reduced hospital stay and induced earlier return to normal diet.12
We found that laparoscopic repair did result in earlier return to normal diet and reduced hospital stay than open repair (4.17±0.62 [SD] vs. 5.03±2.34 days, 8.63±1.96 [SD] vs.
10.24±3.59 days, respectively). This early return to work after laparoscopic surgery for perforated peptic ulcer offsets the cost incurred in performing laparoscopic repair.27
Many reports about laparoscopic treatment have shown that peritoneal lavage can be done effectively and perforation can be cured safely.7-11 It is beyond doubt laparoscopy offers better cosmetic results. Moreover, it is also shown that fewer post- operative complications, such as adhesions and incisional her- nias, occur in laparoscopy patients.28 Our result was 8.6% vs.
18.9%. This may be attributable to the decreased handling of tissue in laparoscopic surgery but little significance was shown.
However, the number of complications in laparoscopic surgery was small compared with open group. Therefore, laparoscopic method is now an option chosen by many surgeons which avoids wound complications and allows easier and more com- prehensive cleansing of the entire peritoneal cavity.9
Sebastian et al. recommends postoperative antibiotics for all who had simple closure.29 We gave patients oral proton pump inhibitor (omeprazole 40 mg) and antibiotics (supprax 200 mg) at the time of discharge. Omeprazole was given for 2 months and supprax for 2 weeks. There is no statistical significance but laparoscopic group experienced less recurrence (8.6% vs.
13.5%).
Laparoscopic repair is becoming standard treatment of perforated peptic ulcer but there are still limitations. First of all, laparoscopic simple closure is not available in all hospitals especially primary hospital center. As the number of surgeons is declining, there may be fewer doctors who can perform operation. More programs on laparoscopy should be set up to produce more laparoscopic surgeons. It is also reasonable that further studies are still needed to compare the late follow-up results (ulcer recurrence, incision hernias, and adhesions)
following different surgical approaches. Total number of patients needs to be larger to make generalized analysis.
However, laparoscopic simple closure of perforated peptic ulcer disease is safe and may be the first and suitable method of treatment up to now. Not only operative time but postoperative complications could be diminished with various methods that make laparoscopy easier.
Previous studies have shown a suture leak rate of 7% with laparoscopic repair; however, we demonstrated that this can be completely abolished and can be superior to open surgery, for which a leak rate of 0% has been reported.30 Leakage may be due to technical error or friability of the patients’ tissue.
Unfortunately, foreign materials are not available because intra- peritoneal cavity is contaminated and foreign materials may ag- gravate intraperitoneal contamination. Omentopexy will be the only protector that can reinforce the suture for now. There still needs improvement in surgical materials and more inves- tigations should be followed for far better outcome treating per- forated peptic ulcer.
CONCLUSION
Laparoscopic primary closure of perforated peptic ulcer is method of choice nowadays. Although it is still difficult to perform laparoscopic simple closure in primary hospital center, laparoscopic surgery of perforated peptic ulcer offers patients an improved outcome compared with conventional open repair even in secondary hospital center.
REFERENCES
1) Graham DY. Treatment of peptic ulcers caused by Helicobact- er pylori. N Engl J Med 1993;328:349-350.
2) Graham DY. Prevention of gastroduodenal injury induced by chronic nonsteroidal antiinflammatory drug therapy.
Gastroenterology 1989;96(Suppl):675-681.
3) Koo J, Ngan Lam SK. Trends in hospital admissions, perfo- ration and mortality of perforation and mortality of peptic ul- cer in Hong Kong from 1970-1980. Gastroenterology 1983;84:
1558-1562.
4) Croft TJ, Park KG, Steele RJ, Chung SS, Li AK. A random- ized trial of nonoperative treatment for perforated peptic ulcer.
N Engl J Med 1989;320:970-973.
5) Sawyer JL. Acute perforations of peptic ulcer. In: Scott HW, Sawyers JL, editors. Surgery of the stomach, duodenum and small intestine. 2nd ed. Boston, MA: Blackwell Scientific;
1992. 566-572.
6) Hugh TB. Perforated peptic ulcers. In: Schwarz S, Ellis HA,
editors. Maingot’s abdominal operations. 9th ed. Norwalk, CT:
Appleton and Lange; 1990. 627-645.
7) Nathanson LK, Easter DW, Cuschieri A. Laparoscopic re- pair/peritoneal toilet of perforated duodenal ulcer. Surg Endosc 1990;4:232-233.
8) Perrissat J, Collet D, Edye M. Therapeutic laparoscopy.
Endoscopy 1992;24:138-143.
9) Mouret P, Francois Y, Vignal J, Barth X, Lombard-Platet R.
Laparoscopic treatment of perforated peptic ulcer. Br J Surg 1990;77:1006.
10) Beriot J, Champault GG, Lebhar E, Sezeur A. Sutureless lapa- roscopic treatment of perforated duodenal ulcer. Br J Surg 1992;80:1212.
11) Lau WY, Leung KL, Zhu XL, Lam YH, Chung SC, Li AK.
Laparoscopic repair of perforated peptic ulcer. Br J Surg 1995;82:814-816.
12) Siu WT, Leong HT, Law BK, Chau CH, Li AC, Fung KH, et al. Laparoscopic repair for perforated peptic ulcer: a randomized controlled trial. Ann Surg 2002;235:313-319.
13) Naesgaard JM, Edwin B, Reiertsen O, Trondsen E, Faerden AE, Rosseland AR. Laparoscopic and open operation in pa- tients with perforated peptic ulcer. Eur J Surg 1999;165:209-214.
14) Blomgren LG. Perforated peptic ulcer: long-term results after simple closure in the elderly. World J Surg 1997;21:414-415.
15) Van der Hulst RW, Rauws EA, Koycu B, Keller JJ, Bruno MJ, Tijssen JG, et al. Prevention of ulcer recurrence after eradication of Helicobacter pylori: a prospective long-term fol- low-up study. Gastroenterology 1997;113:1082-1086.
16) Hermansson M, Stael von Holstein C, Zilling T. Peptic ulcer perforation before and after the introduction of H2-receptor blockers and proton pump inhibitors. Scand J Gastroenterol 1997;32:523-529.
17) Ng EK, Lam YH, Sung JJ, Yung MY, To KF, Chan AC, et al. Eradication of Helicobacter pylori prevents recurrence of ulcer after simple closure of duodenal ulcer perforation:
randomized controlled trial. Ann Surg 2000;231:153-158.
18) Lau WY, Leung KL, Kwong KH, Davey IC, Robertson C, Dawson JJ, et al. A randomized study comparing laparoscopic versus open repair of perforated peptic ulcer using suture or sutureless technique. Ann Surg 1996;224:131-138.
19) Cuschieri A. Whither minimal access surgery: tribulations and expectations. Am J Surg 1995;169:9-19.
20) Darzi A, Cheshire NJ, Somers SS, Super PA, Guillou PJ, Monson JR. Laparoscopic omental patch repair of perforated duodenal ulcer with an automated stapler. Br J Surg 1993;
80:1552.
21) Nassar A. Laparoscopic omental patch repair of perforated du- odenal ulcer with automated stapler. Br J Surg 1994;81:1393.
22) Johansson B, Hallerback B, Glise H, Johnsson E. Laparoscopic suture closure of perforated peptic ulcer. A nonrandomized comparison with open surgery. Surg Endosc 1996;10:656-658.
23) Miserez M, Eypasch E, Spangenberger W, Lefering R, Troidl
H. Laparoscopic and conventional closure of perforated peptic ulcer. A comparison. Surg Endosc 1996;10:831-836.
24) Druart ML, Van Hee R, Etienne J, Cadiere GB, Gigot JF, Legrand M, et al. Lapsaroscopic repair of perforated duodenal ulcer. A prospective multicenter clinical trial. Surg Endosc 1997;11:1017-1020.
25) Bergamaschi R, Marvik R, Johnsen G, Thoresen JE, Ystgaard B, Myrvold HE. Open vs laparoscopic repair of perforated peptic ulcer. Surg Endosc 1999;13:679-682.
26) Lee JS, Park SH, Kim JH, Park JM, Ahn EJ. Early experience with laparoscopic primary closure of peptic ulcer perforation.
J Korean Soc Endosc Laparosc Surg 2009;12:63-67.
27) Bhogal RH, Athwal R, Durkin D, Deakin M, Cheruvu CN.
Comparison between open and laparoscpic repair of perforated peptic ulcer disease. World J Surg. 2008;32:2371-2374.
28) Lau H. Laparoscopic repair of perforated duodenal ulcer: a meta-analysis. Surg Endosc 2004;18:1013-1021.
29) Sebastian M, Chandran VP, Elashaal YI, Sim AJ. Helicobacter pylori infection in perforated peptic ulcer disease. Br J Surg 1995;82:360-362.
30) Lunevicius R, Morkevicius M. Comparison of laparoscopic versus open repair for perforated duodenal ulcers. Surg Endosc 2005;19:1565-1571.