Abstract
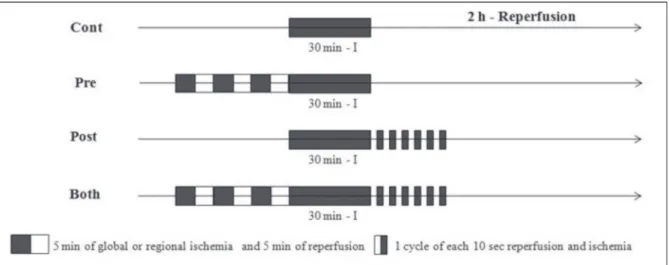
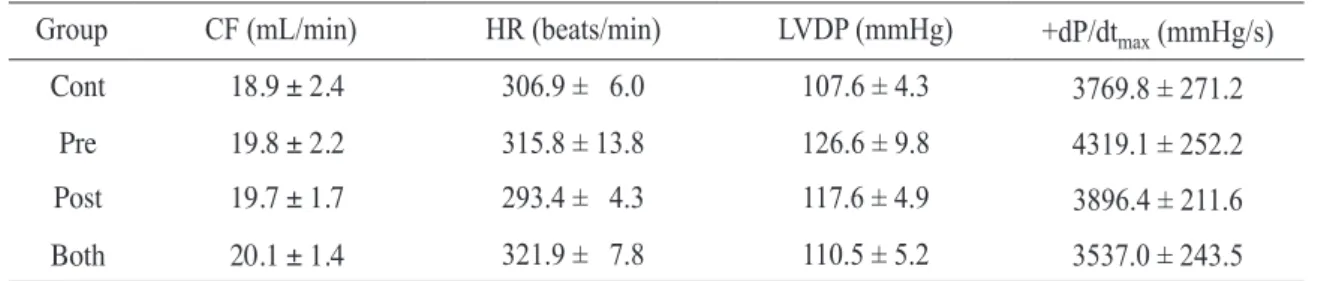
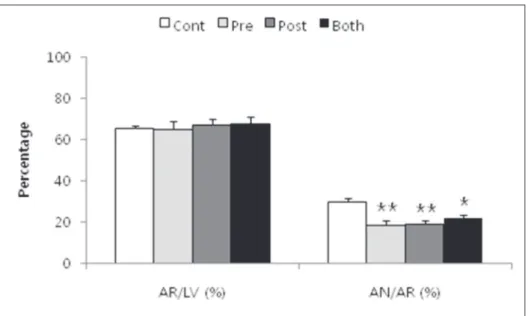
Ischemic preconditioning (Pre) phenomenon was well known as cardioprotective effects and its signaling pathways leading to myocardial protection activated by NO/cGMP pathways. In the meantime, the ischemic postconditioning (Post) in which brief intermittent repetitive interruptions to reperfusion at the onset of timely reperfusion after a prolonged period of ischemia also reduced myocardial injury to an extent comparable to Pre. In isolated working heart experiment, all hearts were subjected to 30 min of regional ischemia and 120 min of reperfusion: Control, no intervention; Pre, 3 cycles of 5-min of global ischemia and 5 min of reperfusion before the ischemic insult, Post; 6 cycles of 10 sec of reperfusion followed by 10 sec of global ischemia immediately after the index ischemia; Both (Pre + Post). Infarct size, coronary flow (CF), heart rate (HR), left ventricular developed pressure (LVDP), and +dP/dt were measured. The infarct size in the Pre (n=7, 18.5% ± 2.1%), Post (n=7, 19.1% ± 1.5%), and Both (n=10, 21.7% ± 1.7%) groups was significantly decreased compared with Control (n=7, 29.9% ± 1.7%). However, there was no additive effect when Pre and Post were combined. There were no significant differences in baseline CF, HR, LVDP, +dP/dt among the groups, and no significant differences in HR, LVDP, +dP/dt in all groups after 2 hours of reperfusion. In conclusion, Pre and Post, Both group improved cardioprotective effects than Control group.
However, combination of ischemic preconditioning and postconditioning showed no additive cardioprotective effects in isolated rat heart models.
Division of Cardiology, Department of Internal Medicine, Keimyung University School of Medicine, Daegu, Institute of Cardiovascular Research, Pusan National University Yangsan Hospital
1,
Gyeongsangnam-do, Korea
In Gyu Yeo, B.S., Hyoung Seob Park, M.D., Sang Woong Choi, M.D., Han Byul Kim, M.D., Jae Pil Lee, M.D., In Cheol Kim, M.D., Jeong Eun Lee, M.D., Hyuck Jun Yoon, M.D.,
Hyung Seop Kim, M.D., Chang Wook Nam, M.D., Seung Ho Hur, M.D., Yoon Nyun Kim, M.D., Kwon Bae Kim, M.D. Young Ho Jang
1, M.D.
Combination of Ischemic Preconditioning and Postconditioning in Isolated and Intact Rat Hearts: Does it Work or Not?
Corresponding Author: Hyoung Seob Park, M.D., Department of Internal Medicine, Keimyung University School of Medicine 56 Dalseong-ro, Jung-gu, Daegu 700-712, Korea
Tel : +82-53-250-7473 E-mail : [email protected]