pISSN: 1225-4207 eISSN: 2233-7296
Technical Report
RECEIVED September 1, 2013, REVISED September 19, 2013, ACCEPTED January 15, 2014 Correspondence to Min-Keun Kim
Department of Oral and Maxillofacial Surgery, College of Dentistry, Gangneung-Wonju National University 7 Jukheon-gil, Gangneung 210-702, Korea
Tel: 82-33-640-2753, Fax: 82-33-640-3103, E-mail: [email protected]
CC
This is an open access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
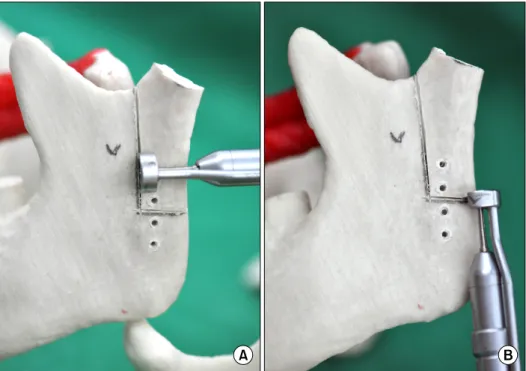
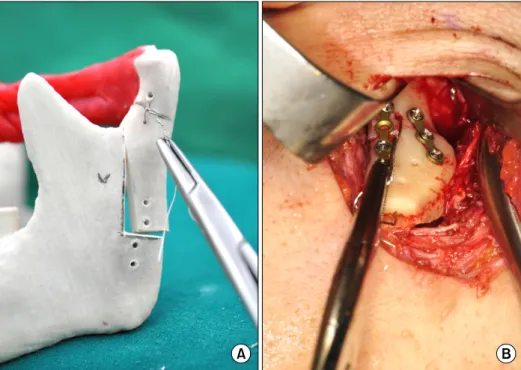
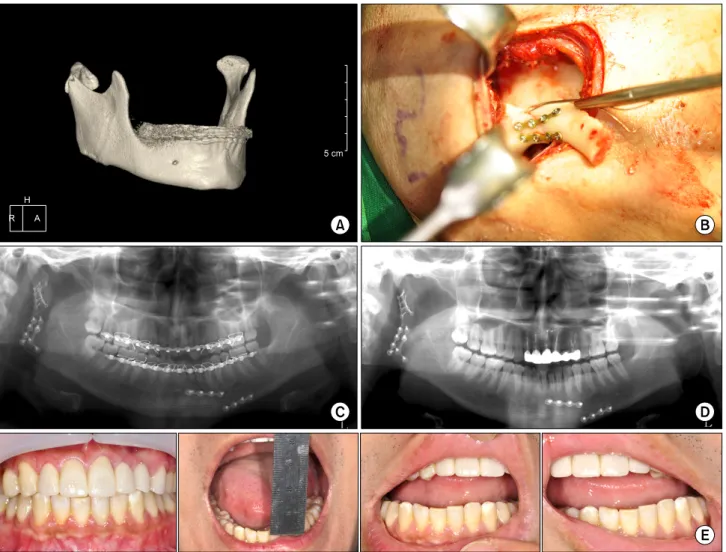
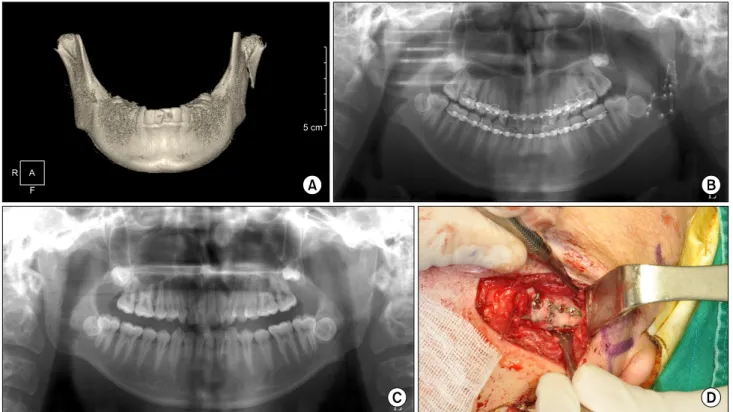
Modified Extracorporeal Reduction of the Mandibular Condylar Neck Fracture
Min-Keun Kim, Kwang-Jun Kwon, Seong-Gon Kim, Young-Wook Park, Jwa-Young Kim 1 , Hae-Yong Kweon 2
Department of Oral and Maxillofacial Surgery, College of Dentistry, Gangneung-Wonju National University,
1
Department of Oral and Maxillofacial Surgery, Hallym University College of Medicine,
2