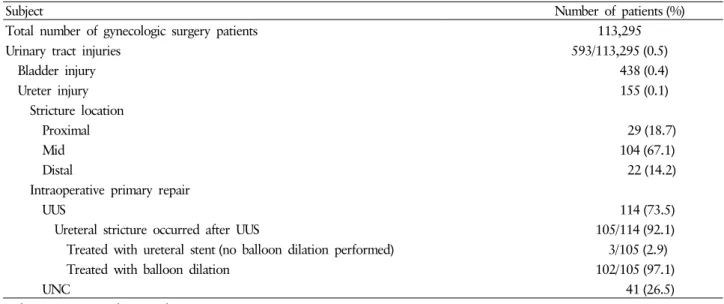
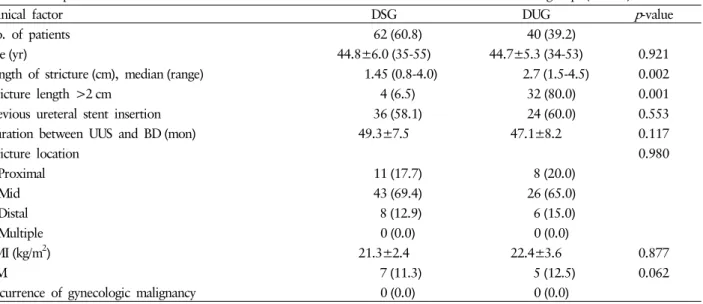
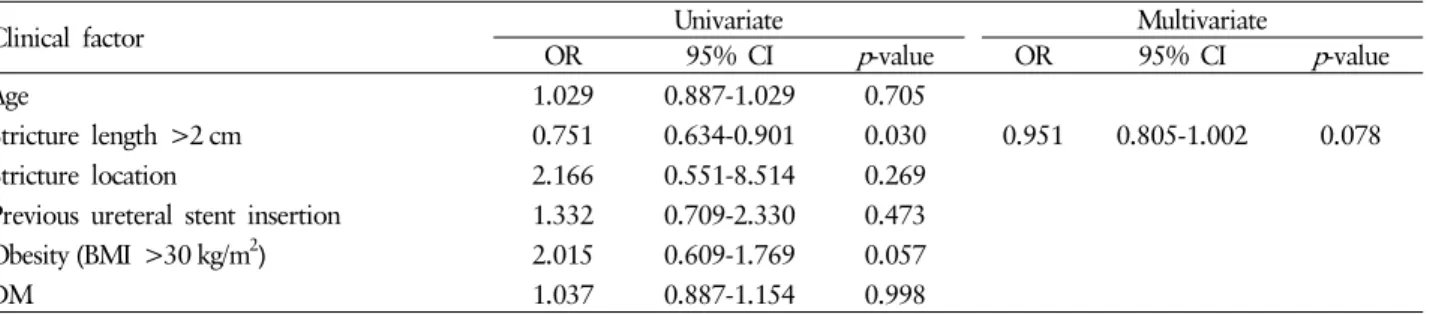
Retrograde balloon dilation as a therapeutic option for post-gynecologic surgery ureteral stricture followed by ureteroureterostomy: a comparative study regarding stricture length
8
0
0
전체 글
(2)
(3)
(4)
(5)
(6)
(7)
(8)
수치
관련 문서
Seven patients underwent H. pyroli eradication therapy. Three patients showed complete response, but four patients failed... Conclusion
Thermal balloon ablation versus endometrial resection for the treatment of abnormal uterine bleeding. Thermal balloon ablation in myoma-induced menorrhagia
As the option pricing models to provide a theoretical option values, Black-Scholes and a binomial lattice option pricing models, most widely used, will
Therefore, this study aims to maintain the even saponin content by standardizing balloon flower extract (60ml) to use as tea to maximize the
Thus, as visual expansion interprets expressive characteristics applied for walls as physical structures by a visual and perceptual recognition system, non-materialization
Endoscopic papillary large balloon dilation(EPLBD) involves endoscopic biliary sphincterotomy followed by balloon dilation using 12-20mm balloon to remove large
출처 : IAEA 발표 자료(Comprehensive inspection exercise at bulk handling facilities, “U-235 Enrichment measurements by gamma-ray spectroscopy”) 13. Uranium
Superior tensile properties were obtained, and heat treatment time could be shortened by the austenitizing treatment at A C1 +30∼40℃ followed by
