악성 식도호흡기루 (esophagorespiratory fistula, 는 대부분 식도암 또는 폐암으로 인해 생기는 ERF)
치명적인 합병증이다 식도암의 경우 . 5~15% 에서 , 폐암의 경우에는 1% 미만에서 ERF 가 병발하는 것 으로 알려져 있다 일반적으로 . ERF 는 esophagotra-
또는 를 가리키
cheal fistula esophagobronchial fistula
나 넓은 의미에서는 esophagopulmonary fistula 를 포 함한다.
암 자체 외에 방사선 치료나 레이저 치료 그리 , 고 기존에 넣었던 스텐트 대부분 식도 스텐트 에 ( ) 의한 압박 괴사로 ERF 의 형성을 조장할 수 있다 . 임상적으로 환자들은 사래가 걸리지 않고서는 음 식을 삼키기 어렵고 결국 fistula 를 통한 흡인성 폐 렴 및 패혈증을 일으켜 사망에 이르게 된다 따라 . 서 빠른 진단과 치료가 필수적이라고 할 수 있다.
의 치료에 있어서 수술은 매우 제한적이라 ERF
고 할 수 있다 . Operative mortality 가 13~45% 로 보 고되었으며 excluded esophagus 의 disruption 이나 가 치명적인 합병증이라고 할 anasto- motic leakage
수 있다 최근에 . Seto 등이 gastric tube 를 이용한
와 를 시행하여 명의
esophageal bypass cardiostomy 4 환자에서 좋은 결과를 보고하였으나 더 많은 경험 이 요구된다.
1)경정맥 영양요법이나 위루술은 금식 을 유지하며 영양 공급은 할 수 있으나 침에 의한 흡인은 막을 수 없으므로 근본적인 치료라고 하기 어렵다 . 1990 년대 초반까지는 rigid plastic pro- 에 대한 보고가 있었으나 천공 출혈 압박
stheses , ,
괴사 그리고 , tube dislodgment / migration 이 높은 문 제점이 있다 . 1993 년도 이후부터 covered expand- 를 이용한 치료가 보고되기 시작 able metallic stent
했으며 현재 가장 널리 쓰이고 있는 비수술적 치료 방법이라고 할 수 있다.
2)진단은 ERF 가 생길만한 병을 가진 환자에서 음
大 韓 氣 管 食 道 科 學 會 誌
□ 종 설 □
Vol.14. No. 1, Jun. 2008
악성 기관지호흡기루와 기관지흉강루에 대한 인터벤션 치료
울산의대 서울아산병원 영상의학교실
신 지 훈 김 경 래 김 진 형 송 호 영
=Abstract=
Interventional Management of Malignant Esophagorespiratory Fistula and Bronchopleural Fistula
Ji Hoon Shin, M.D., Kyung-Rae Kim, M.D., Jin-Hyoung Kim, M.D., Ho-Young Song, M.D.
Department of Radiology, University of Ulsan Medical College, Asan Medical Center, Seoul, Korea
Malignant esophagorespiratory fistula is a devastating and life-threatening complication of esophageal and bronchogenic carcinomas. As a non-surgical treatment, peroral stent placement into the esophagus or airway can close-off the fistula and prevent progression of the pneumonia. Although reopening of the fistula is not uncommon despite stent placement, interventional treatment is effective for sealing off reopened ERFs. Bronchopleural fistula is a well-recognized complication of pneumonectomy. There have been several reports to occlude the fistula with use of stents and much more experience is required.
신지훈 서울시 송파구 풍납동
: , 388-1
서울아산병원 영상의학과
전화 : 02-3010-4380 Fax : 02-476-0090 E-mail: [email protected]
식물 섭취 시 흡인이 생기면 의심할 수 있고 내시 경으로 확진을 하게 된다 . CT 로 원래 가지고 있는 병과 동반된 폐렴의 범위를 보고 fistula 의 위치와 주위 조직 간의 관계를 보게 되는데 이는 스텐트 삽입술 시 중요한 정보를 제공한다 차원 영상 . 3 CT 의 경우 침범된 기도의 정상 직경과 기관분기부 및 성대까지의 거리에 대한 정보를 알 수 (carina)
있어서 스텐트의 크기를 결정하는데 매우 유용하 다.
전통적으로 ERF 라 하면 esophagotracheal or 를 의미한다 그러나 넓은 esophagobronchial fistula .
의미에서는 esophagopulmonary fistula, 더 넓게는 를 포함할 수 있다
esophagopleural fistula . Esophag-
는 넓은 의미의 의
otracheobronchial fistula ERF 85 -
이상을 차지하며 약 가
95% 3-11% esophagopulmon-
나머지 가 를
ary fistula, 1-2% esophagopleural fistula 차지한다 본 소고에서는 이 중 . esophagotra cheo-
와 에 대해
bronchial fistula esophagopulmonary fistula 서 기술하고 ERF 의 개념이라고는 할 수 없으나 폐 절제술 등의 수술 후에 생길 수 있고 임상적으로 매우 중요한 bronchopleural fistula 에 대해서 다루고 자 한다.
Ⅰ. Esophagotracheobronchial Fistula
Conventional unexpandable plastic plastic pro- 는 천공 출혈 압박 괴사
stheses , , , tube dislodgment / 폐쇄와 같은 합병증이 약
migration, tube 15 - 40% 까 지 보고가 되어서
3)이를 극복하고자 1990 년대 중 반부터는 covered expandable metallic stent 가 ERF 의 치료로 보고되어 67 - 100% 의 ERF 폐쇄율을 보고 하였다
.2), 4-8)지금까지 61 명의 환자에서의 장기 추적 보고가 가장 대규모의 임상 보고로 스텐트 설치의 기술적 성공 여부 , fistula 폐쇄와 관련된 흡인 증상의 조절 여부 , fistula 의 재개통 합병증 그리고 생존 기간에 , , 대해 자세히 보고하였다.
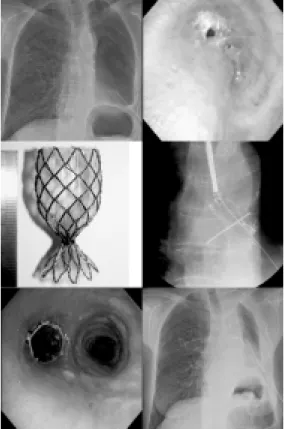
2)식도 스텐트로는 poly- 로 피복한 urethane or PTFE (polytetrafluoroethylene)
스텐트가 사용되었으며 (Fig. 1), 일부 환자에서는 기관기관지 스텐트도 쓰였다 . Fistula 가 있을 경우
식도 스텐트의 경우에는 18mm 짜리 직경의 것을 사용한다 (fistula 가 없는 경우 보통 16mm 직경의 스텐트를 사용).
명의 환자에서 스텐트는 모두 성공적으로 넣 61
을 수 있었고 시술과 관련된 직접적인 합병증은 없 었다 스텐트는 . 61 명의 환자 중 49 명의 환자에서 를 막을 수 있었으며 흡인 증상도 호전 (80%) fistula
되었다 (initial clinical success) (Fig. 2). 반면 12 명
의 환자에서는 의 불완전한 폐쇄로 계속
(20%) ERF
적인 흡인 증상이 남아있었다 (initial clinical
추적 검사에서 의 재개통은
failure). fistula initial
를 보였던 명의 환자 중 명
clinical success 49 17
에서 보였다 재개통 되었던 명 중
(35%) (Fig. 3). 17
다시 스텐트 재삽입이나 풍선확장술(food impaction 을 밀어냄 등의 인터벤션 치료를 받았던 명의 환 ) 8 자에서 다시 성공적으로 fistula 를 막을 수 있었다 (Fig. 3).
명의 환자에서 주의 평균 생존 기간을 보
61 13.4
였고 스텐트 설치 후 바로 fistula 가 막히는 initial 의 경우가 그렇지 않은
clinical success initial clinical 에 비해 통계적으로 유의하게 생존율이 높아 failure
Fig. 1. Covered retrievable expandable metallic
esophageal stent. 18-mm diameter stent is used for
the esophagorespiratory fistula (ERF) closure. To
make the stent removable, a nylon loop is hooked
inside each bend of the proximal end of the stent and
then two nylon drawstrings are passed through each
of the loops
서 (15.1 vs. 6.2 weeks) 초기 fistula 를 잘 막아주는 것이 생존 연장을 도와줄 수 있음을 시사한다고 할 수 있다.
재개통의 원인으로는 스텐트가 막히는 경우가 가장 흔한데 food impaction, granulation tissue for- 등이 스텐트 폐색의 주원인이었다 이 외에
mation .
도 식도 협착이 느슨해져 식도 벽과 스텐트 사이의 간격이 생겨서 재개통이 생긴 경우 피복 물질의 , 변성이나 스텐트 이동 등이 있을 수 있다.
가 있는 환자에서 식도와 기도의 해부학을 ERF
정확히 이해하는 것이 어느 쪽에 스텐트를 넣느냐 에 매우 중요하다 (Fig. 4). 일반적으로
1)식도의 협 착이 심하고 기도의 협착이 없거나 경미하면 식도
스텐트를,
2)기도의 협착이 심하고 식도의 협착이 없거나 경미하면 기도 스텐트를,
3)식도와 기도 둘 다 심하지 않을 경우 기도 스텐트를,
4)식도와 기도 둘 다 심한 경우에는 먼저 기도 스텐트를 넣고 추 후 식도 스텐트를 고려하거나 동시에 기도와 식도 에 스텐트를 넣을 수 있다 (Fig. 5).
에 스텐트를 넣을 경우 추적 검사가 매우 중 ERF
요하다 . Fistula 가 완전히 막히지 않거나 처음에는 막힌다 하더라고 재개통되는 경우에 흡인 증상이 생겨서 환자의 상태를 안 좋게 하기 때문이다 스 . 텐트를 넣자마자 식도조영술을 하는 것은 환자가 식사를 하기 전에 fistula 의 폐쇄 여부를 확인하는데 매우 중요하다 이 때 스텐트가 충분히 펴지지 않 . Fig. 2. Esophageal cancer with development of es-
ophagobronchial fistula. Covered expandable metallic stent (18mm in diameter) was inserted to dilate the stricture and occlude the fistula.
Fig. 3. Reopening of the esophagotracheal fistula.
Esophageal stent was inserted for the fistula. How- ever, reopening due to food impaction occurred one month later. To-and-fro movement of the inflated balloon was done to cleanse the stent.
Fig. 4. Determination of stenting area in cases of ERF. Left one is before stenting. Right one is after stenting.
아서 계속적인 조영제 유출이 있는 경우 2~3 일 후 에 다시 식도조영술을 시행하여 스텐트가 잘 펴져 있는지를 확인하는 것이 필요하다.
결론적으로 esophagotracheobronchial fistula 에 있 어서 covered metallic stent 치료는 initial clinical
가 정도이고 재개통률이 높다 그
success rate 80% .
러나 재개통이 되더라도 인터벤션 치료가 재계통 된 ERF 의 폐쇄에 효과적이라고 할 수 있다 .
Ⅱ. Esophagopulmonary Fistula 를 가진 환자의 약
ERF 3 - 11% 의 환자에서 폐
실질과의 교통이 있는 esophagopulmonary fistula 로 알려져 있다.
9-11)Esophagopulmonary fistula 에 대한 보고는 매우 제한적이나 폐농양 또는 폐렴의 빈도 가 더 높아서 esophagotracheobronchial fistula 보다 임상적으로는 더 좋지 않은 것으로 생각되어 이에 대한 치료가 절실히 필요하다고 할 수 있다.
1), 2)저자들은 약 20 여 년간 14 명의 esophagopul- 환자에서 스텐트 치료를 하였다
monary fistula (su-
식도암과 폐암 환자가 각각 명과
bmitted data). 9 5
명이었다 총 . 12 명에서 방사선 치료나 항암 치료를 받아서 이러한 치료가 fistula 를 조장할 수 있음을 시사한다 흡인성 폐렴은 . 14 명 모두에서 있었고 폐
농양은 11 명의 환자에서 보였다 .
모든 환자에서 스텐트 설치는 성공적이었고 스 텐트 치료로 12 명의 환자에서 fistula 를 막을 수 있 었으나 (86% 의 clinical success) (Fig. 6), 2 명의 환자 에서는 식도와 스텐트 사이의 간격으로 인해 fistula 가 막히지 않았다 . Clinical success 를 보였던 12 명의 환자에서 추적 검사에서 명의 환자에서 2 fistula 의 재개통이 있었다 추적 검사에서 폐농양의 크기는 . 평균 8cm 에서 5.4cm 으로 감소했으나 그럼에도 불 구하고 폐농양은 없어지지 않고 계속 남아 있어서 환자의 임상 증상 악화를 초래하는 원인으로 작용 하였다 염증이나 농양으로 인한 분비물이 스텐트 . 를 넣었을 때 기도를 통해 충분히 배출되지 못할 경우 폐렴 또는 농양이 지속될 수 있는 것으로 추 정된다 그러나 스텐트가 . fistula 를 잘 막을 경우 식 도를 통한 흡인이 방지되어 폐렴의 진행을 완화시 킬 수 있고 환자의 경구 섭취가 가능한 점은 스텐 트 설치 후 기대할 수 있는 장점이 될 수 있다.
따라서 esophagopulmonary fistula 환자에서 스텐 트 설치는 고식적 치료의 좋은 대안이 될 수 있을 것으로 생각된다 그러나 스텐트 치료에도 불구하 . 고 폐농양이 잔존하여 임상 양상의 악화가 흔하여 이에 대해서는 추후 더 연구가 필요하다고 할 수 있다.
Fig. 5. Simultaneous tracheal and esophageal stenting in a patient with hypopharynx cancer. Both trachea and esophagus were narrowed. Tracheal stent was inserted first, followed by esophagealstent. If esopha- geal stent had been inserted first, the patient would have suffered from tracheal compressionbefore trac- heal stent placement.
Fig. 6. Placement of a covered stent in a patient with esophago-bronchial (white arrow) and esophago- pulmonary (black arrow) fistulae. Stent placement was performed successfully with sealing of both fistulae.
Follow-up CT scans shows much resolution of the
abscess cavity in left lower lobe.
Ⅲ. Bronchopleural Fistula (BPF)
Bronchopleural fistula (BPF) 는 esophagorespiratory 라고 할 수 없지만 수술 후 생길 수 있는 중요 fistula
한 합병증으로 스텐트에 대한 치료가 최근 보고되 고 있어서 여기서 다루고자 한다.
는 말 그대로 와
BPF pleural space bronchial tree 간의 비정상적인 통로를 말하며 pulmonary resec- tion 후에 1.5 - 28% 정도 생기는 것으로 알려져 있
다.
1), 3)임상 양상과 더불어 기관지경을 가지고 진
단할 수 있으며 bronchial stump 와 fistula 의 크기 , 의 위치 등에 관한 정보는 치료 방침을 결정 fistula
함에 매우 중요하다고 할 수 있다.
1), 3)수술적 방법
외에 기관지경으로 fibrin glue 등의 tissue adhesive, 그리고 coil 을 넣는 방법 등이 소개되고 있으며 최근 에는 스텐트 치료의 좋은 성적들이 보고되고 있다.
Expandable metallic stents
14), 15)와 non-metallic stents
16), 17)
등의 보고가 있었으며 bronchial stump 가 있을
경우 bronchial stent-graft occluder 또는 plugged,
와 같은 에
bullet-shaped, angled stent occluding stent 관한 보고가 있었다.
18), 19)는 스텐트를 사다리 Bronchial stent-graft occluder
꼴 모양으로 만들고 Dacron graft 로 원위 부분을 감 싸게 만든 것으로 흉강을 통해 삽입할 수 있게 하 였고 두 명의 환자에서 성공적인 시술이 보고되었 다.
18)Plugged, bullet-shaped, angled stent 의 경우에는 실제로 hinge 모양으로 tracheal part 와 bronchial part 가 연결되어 있으며 bronchial part 의 끝 부분이 총 탄 모양으로 되어 있으며 polyethylene 으로 피복되 어 있으며 bronchial stump fistula 의 폐쇄가 명 중 6
명 에서 보였다
5 (83%) .
19)최근에 저자들은 bronchial
가 있는 의 경우 스텐트의 중간 부분을
stump BPF
잘록하게 하여 공기의 흐름을 차단하게 하는 occlu- 를 개발하여 환자에 적용하고 있다
der stent (Fig. 7).
이것은 입을 통해 비교적 쉽게 넣을 수 있는 장점 이 있으며 제거도 가능하게 하였다.
요약하면 ERF 와 BPF 이 생겼을 경우 수술적 치 료가 어려운 경우가 많고 내시경적 치료도 제한적 인 경우가 많다 스텐트가 더 정교해지고 질이 개 . 선되면서 스텐트를 통한 치료가 더 일반화될 것이 라고 기대된다.
References