VOL. 18, NO. 2, 2019 Case Report
CLINICAL PAIN 111 https://doi.org/10.35827/cp.2019.18.2.111
접수일: 2018년 12월 30일, 게재승인일: 2019년 5월 31일 책임저자: 최은석, 대전시 중구 대흥로 64
34943, 가톨릭대학교 의과대학 대전성모병원 재활 의학교실
Tel: 042-220-9650, Fax: 042-252-6807 E-mail: [email protected]
쯔쯔가무시병에 의한 길랑-바레 증후군의 신경병성 통증
가톨릭대학교 의과대학 대전성모병원 재활의학교실
강새롬ㆍ이숙정ㆍ최은석
Neuropathic Pain in Guillain-Barre Syndrome Associated with Scrub Typhus
Saerom Kang, M.D., Sook Jung Lee, M.D., Ph.D. and Eunseok Choi, M.D., Ph.D Department of Rehabilitation Medicine, Daejeon St. Mary’s Hospital, College of Medicine,
The Catholic University of Korea, Daejeon, Korea
Guillain-Barre syndrome (GBS) is usually characterized by acute areflexic ascending paralysis with minimal sensory involvement.
Only a few cases of GBS associated with scrub typhus have been reported. Previous case reports focused on the laboratory findings, pathogenesis, and clinical manifestation. Unlike the previous case, neuropathic pain was a prominent symptom of GBS in our case. We report scrub-typhus-related GBS with a detailed description of the clinical manifestations, especially neuropathic pain, along with results of serial follow-up electrodiagnostic studies. (Clinical Pain 2019;18:111-114)
Key Words: Guillain-Barre syndrome, Scrub typhus, Neuralgia
INTRODUCTION
Guillain-Barre syndrome (GBS) usually presents as pro- gressive areflexic ascending paralysis with minimal sensory involvement.1 The pathophysiology of GBS involves T lymphocyte activation or immune cross-reactivity of patho- gen antibodies with axonal or Schwann cell membranes.2,3 Two-thirds of patients have a history of Campylobacter je- juni, cytomegalovirus (CMV), or Epstein-Barr virus (EBV) infection within the previous 6 weeks.1,2,4 Complications of scrub typhus are known to involve the central nervous systems.5,6 Only a few cases of GBS associated with scrub typhus (Orientia tsutsugamushi) infection have been reported.4,5,7,8 Previous case of GBS associated with scrub typhus reports focused on the fact that scrub typhus can cause GBS, the laboratory findings, pathogenesis, and clin- ical manifestation. There was no serial follow-up of elec- trodiagnostic studies and no describe of recovery course of neuropathic pain. In this case report, we present clinical de-
tails, particularly characteristics and duration of neuro- pathic pain, and serial electrodiagnostic results during dis- ease progression and recovery. We also consider the recov- ery course of each clinical manifestation and the relation- ship between neuropathic pain and electrodiagnostic stu- dies.
CASE REPORT
A 66-year old man presented with loss of appetite, gen- eral weakness, hematuria, and elevated liver enzymes 10 days after picking persimmons in the countryside. He had a dark-colored rash on his chest and an eschar on his me- dial thigh. Thus, he was diagnosed with scrub typhus and was prescribed doxycycline at the outpatient clinic. Three days later, he began to experience gait difficulty and visited the emergency department. Initial laboratory results were:
white blood cell (WBC) count, 8,300/mm3 (neutrophils 30.9%, lymphocytes 55.2%); hemoglobin, 14.4 g/dL; plate- lets, 390,000/mm3; serum aspartate aminotransferase and alanine aminotransferase, 80 IU/L and 68 IU/L; and C-re- active protein, 0.41 mg/dL. The serum O. tsutsugamushi antibody titer was positive (1:5120). There was no sero- logic evidence of EBV or CMV infection (VCA-IgG/IgM
+/−; EADR-IgG/IgM −/−; EBNA IgG/IgM +/−;
CMV IgG/IgM +/−) and the HIV and VDRL tests were
VOL. 18, NO. 2, 2019
CLINICAL PAIN
112
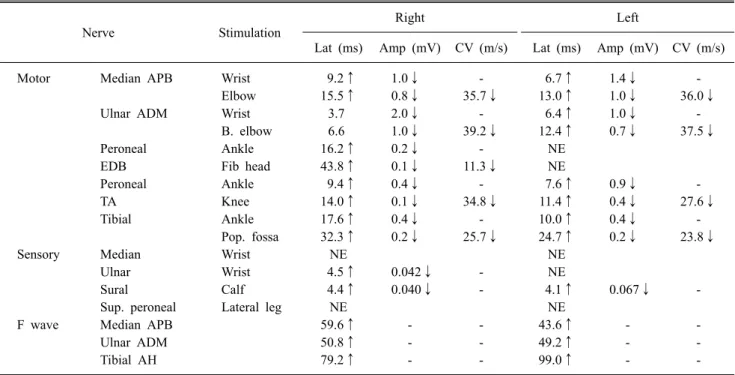
Table 1. Initial Nerve Conduction and F Wave Studies (20 Days after Onset)
Nerve Stimulation Right Left
Lat (ms) Amp (mV) CV (m/s) Lat (ms) Amp (mV) CV (m/s)
Motor Median APB Wrist 9.2↑ 1.0↓ - 6.7↑ 1.4↓ -
Elbow 15.5↑ 0.8↓ 35.7↓ 13.0↑ 1.0↓ 36.0↓
Ulnar ADM Wrist 3.7 2.0↓ - 6.4↑ 1.0↓ -
B. elbow 6.6 1.0↓ 39.2↓ 12.4↑ 0.7↓ 37.5↓
Peroneal Ankle 16.2↑ 0.2↓ - NE
EDB Fib head 43.8↑ 0.1↓ 11.3↓ NE
Peroneal Ankle 9.4↑ 0.4↓ - 7.6↑ 0.9↓ -
TA Knee 14.0↑ 0.1↓ 34.8↓ 11.4↑ 0.4↓ 27.6↓
Tibial Ankle 17.6↑ 0.4↓ - 10.0↑ 0.4↓ -
Pop. fossa 32.3↑ 0.2↓ 25.7↓ 24.7↑ 0.2↓ 23.8↓
Sensory Median Wrist NE NE
Ulnar Wrist 4.5↑ 0.042↓ - NE
Sural Calf 4.4↑ 0.040↓ - 4.1↑ 0.067↓ -
Sup. peroneal Lateral leg NE NE
F wave Median APB 59.6↑ - - 43.6↑ - -
Ulnar ADM 50.8↑ - - 49.2↑ - -
Tibial AH 79.2↑ - - 99.0↑ - -
Lat: Latency, Amp: Amplitude, CV: Conduction velocity, NE: Not evoked, APB: Abductor pollicis brevis, ADM: Abductor digiti minimi, EDB: Extensor digitorum brevis, TA: Tibialis anterior, AH: Abductor hallucis, B. elbow: Below elbow, Pop. Fossa: Popliteal fossa, Sup. peroneal: Superficial peroneal.
also negative. Muscle strength, manual muscle test (MMT), was: right upper extremity, grade 4; left upper extremity, grade 5; and both lower extremities, grade 4. There was no acute infarction or hemorrhage on initial brain imaging.
The patient was admitted to the infectious diseases de- partment for conservative care. On hospital day (HD) 2, he showed progressive tetraplegia (MMT: right upper ex- tremity, grade 2−; left upper extremity and both lower ex- tremities, grade 2). Cerebrospinal fluid (CSF) analysis showed no WBC, total protein 40 mg/dL, and glucose 73 mg/dL. A 5-day course of intravenous immunoglobulin (IVIG) was initiated (30 g, 400 mg/kg/day). On HD 7, fol- low-up CSF study showed no WBC, total protein 320 mg/dL, and glucose 93 mg/dL.
On HD 3, the patient developed respiratory failure with CO2 retention (arterial blood gas: pH 7.433, PCO2 40.2, PO2 130.1) requiring mechanical ventilation. The tetraple- gia continued to progress, with MMT in all extremities de- clining to grade 0. The patient began to recover motor power on HD 6 (MMT right proximal upper extremity, grade 3; right distal upper extremity, grade 2+; left upper
extremity, grade 3; both proximal lower extremities, grade 3+; and both distal lower extremities, grade 3). The serum anti-ganglioside antibodies GD1b IgM and GM1 IgM were positive, while the GM1 IgG was within normal range. On HD 11, the respiratory symptoms were improved and the ventilator was removed.
Electrodiagnostic studies were first performed on HD 19. The sensory nerve conduction studies (NCS) showed delayed peak latencies and decreased amplitudes of sensory nerve action potentials (SNAPs) in the right ulnar nerve and in both sural nerves; absent in the left ulnar nerve, both median nerves, and the superficial peroneal nerves. The motor NCS showed delayed onset latencies of compound motor action potentials (CMAPs) in the left ulnar nerve, both median nerves, and the common peroneal and tibial nerves. Decreased amplitudes and delayed nerve con- duction velocities (NCVs) of CMAPs in both median, ul- nar, tibial, and right common peroneal nerves; absent in the left peroneal nerve. F wave studies showed delayed laten- cies in all four extremities (Table 1). Needle electro- myography (EMG) showed denervation potentials (fibril-
강새롬 외 2 인: 쯔쯔가무시병에 의한 길랑- 바레 증후군의 신경병성 통증
CLINICAL PAIN 113 Table 2. Follow-up Nerve Conduction and F Wave Studies (2 Months after Onset)
Nerve Stimulation Right Left
Lat (ms) Amp (mV) CV (m/s) Lat (ms) Amp (mV) CV (m/s)
Motor Median APB Wrist 4.8↑ 3.1↓ - 5.4↑ 3.6↓ -
Elbow 10.1 2.8↓ 43.2↓ 9.8 3.4↓ 50.0
Ulnar ADM Wrist 3.5 4.3 - 4.9↑ 1.4↓ -
B. elbow 7.9 2.7 51.1 9.6 0.9↓ 44.8↓
Peroneal Ankle 8.8↑ 0.3↓ - NE
EDB Fib. head 20.6↑ 0.3↓ 22.9↓ NE
Tibial Ankle 8.6↑ 1.4↓ - 10.3↑ 0.5↓ -
Pop. fossa 17.3 1.0↓ 40.2 20.9↑ 0.3↓ 25.5↓
Sensory Median Wrist NE NE
Ulnar Wrist NE NE
Sural Calf 4.4↑ 0.035↑ - 4.1↑ 0.041↓ -
Sup. peroneal Lateral leg NE NE
F wave Median APB 35.8↑ - - 38.4↑ - -
Tibial AH 69.4↑ - - 66.4↑ - -
Lat: Latency, Amp: Amplitude, CV: Conduction velocity, NE: Not evoked, APB: Abductor pollicis brevis, ADM: Abductor digiti minimi, EDB: Extensor digitorum brevis, AH: Abductor hallucis, B. elbow: Below elbow, Pop. Fossa: Popliteal fossa, Sup. peroneal:
Superficial peroneal.
lation and positive sharp waves) bilaterally in the biceps brachii, flexor carpi radialis (FCR), and tibialis anterior (TA) muscles, the medial head of gastrocnemius (GCM), and in the right first dorsal interosseous and left abductor pollicis brevis muscles. There was no motor unit action po- tential (MUAP) in bilateral TA, and the medial heads of both GCM; and the interferential patterns of muscles were also reduced in bilateral biceps brachii, FCR, first dorsal interossei, abductor pollicis brevis, gluteus maximus, and gluteus medius muscles.
Follow-up electrodiagnostic studies were preformed 2 months later. No SNAPs were evoked in any sampled nerve on sensory NCS, except the sural nerves; on motor NCS, delayed onset latencies and decreased amplitudes of CMAPs persisted in all sampled nerves except the right ul- nar nerve, and absent in the left common peroneal nerve.
Compared with initial study, there was some improvement in the result of motor NCS, and the F wave studies in all sampled nerves (Table 2). Needle EMG continued to show denervation potentials (positive sharp waves) in the right TA and the medial head of GCM. Large and long duration of MUAP were in right TA and medial head of GCM. All interferential patterns on maximal volition remained reduced. Compared with the previous exam, denervation
potentials were decreased and interferential patterns were improved. The electrodiagnostic results were compatible with a demyelinating peripheral polyneuropathy, clinically acute inflammatory demyelinating polyradiculoneuropathy (AIDP).
On HD 28, he began to complain of neuropathic pain in all four extremities, which he scored as a 5/10 on the visual analog scale (VAS). He had no other cause of pe- ripheral neuropathy. AP/lateral view of plane radiographies of C and L spine showed no newly developed lesion. Sen- sory examination showed hypesthesia and paresthesia in all extremities, and gabapentin 600 mg divided in two was prescribed for neuropathic pain. The patient's motor power continued to improve (MMT both upper extremities grade 5 and both lower extremities grade 4), and he able to walk under supervision. On HD 29, the neuropathic pain was getting worse, and the total dose of gabapentin was in- creased to 1200 mg daily, divided in two. The patient was discharged to home on HD 40 with minimal gait dis- turbance and residual neuropathic pain (VAS 4). Two weeks after discharge, the patient continued to have neuro- pathic pain (VAS 3 to 4) in both hands and feet. One month after discharge, his motor power improved nearly normal, he able to walk independently. The neuropathic pain was
VOL. 18, NO. 2, 2019
CLINICAL PAIN
114
slightly improved, and the total dose of gabapentin was re- duced to 900 mg. Numbness and pain (VAS 2) persisted in the fingertips of the left hand. The neuropathic pain was completely resolved at 4 months, and the gabapentin was tapered and stopped.
DISCUSSION
The incidence of neuropathic pain in GBS is responsible in 34.8% of cases.9 Previous case reports of GBS asso- ciated with scrub typhus focused on the fact that scrub ty- phus can cause GBS, the laboratory findings, and patho- genesis. Nonetheless, there was no mention of serial fol- low-up electrodiagnostic studies and the recovery course of neuropathic pain. Also, the exact duration of recovery from neuropathic pain and the relationship between improvement of motor power and neuropathic pain are not clearly de- fined. It is the first study to describe the relationship be- tween electodiagnostic studies and clinical symptoms. In this case, neuropathic pain was a prominent symptom of GBS. The pain began after the patient's acute paralysis and respiratory failure were resolved, and it persisted at the last.
First NCSs showed delayed latencies and reduced or ab- sent amplitude of SNAPs and CMAPs. We consider AIDP and acute motor-sensory axonal neuropathy (AMSAN).
Follow-up study still showed markedly reduced amplitudes and decreased NCVs of CMAPs. Usually, the latencies of CMAPs and the NCVs should be normal or mildly affected in AMSAN. Therefore, the presence of prolonged latencies, slow NCVs with low amplitudes were determined to be more likely the result of demyelination and conduction block, which mean AIDP.10
Generally, the course of GBS is marked by progressively worsening muscle weakness during the first 2 weeks, which slowly recovers from its nadir during weeks 2 to 4.
Respiratory failure tends to improve first, and the weakness improves from proximal to distal over several weeks to months.1 In this case, the patient's muscle weakness began from 1 week after onset and began to recover after 3 weeks, while the neuropathic pain began at 1 month and persisted for about 4 months. Detailed evaluation of the se- rial electrodiagnostic studies did not show any correlation
with the improvement of the neuropathic pain. Instead, even after the motor weakness and neuropathic pain were completely resolved, the electrodiagnostic studies con- tinued to show signs of demyelinating neuropathy. Thus, we confirmed the order of recovery as: recovery of sponta- neous respiration, recovery of motor strength, recovery from neuropathic pain, and finally, recovery from electro- diagnostic abnormalities. We report this case for the pur- pose of insisting that it is necessary to correctly diagnose and treat neuropathic pain during rehabilitation in patients with GBS.
REFERENCES
1. Hughes RA, Cornblath DR. Guillain-Barre syndrome.
Lancet 2005; 366: 1653-1666
2. Hadden RD, Karch H, Hartung HP, Zielasek J, Weissbrich B, Schubert J, et al. Preceding infections, immune factors, and outcome in Guillain-Barre syndrome. Neurology 2001;
56: 758-765
3. Hartung HP, Pollard JD, Harvey GK, Toyka KV. Immuno- pathogenesis and treatment of the Guillain-Barre syn- drome--Part I. Muscle Nerve 1995; 18: 137-153
4. Ju IN, Lee JW, Cho SY, Ryu SJ, Kim YJ, Kim SI, et al.
Two cases of scrub typhus presenting with Guillain-Barre syndrome with respiratory failure. Korean J Intern Med 2011; 26: 474-476
5. Kim JH, Lee SA, Ahn TB, Yoon SS, Park KC, Chang DI, et al. Polyneuropathy and cerebral infarction complicating scrub typhus. J Clin Neurol 2008; 4: 36-39
6. Silpapojakul K, Ukkachoke C, Krisanapan S, Silpapojakul K. Rickettsial meningitis and encephalitis. Arch Intern Med 1991; 151: 1753-1757
7. Lee SH, Jung SI, Park KH, Choi SM, Park MS, Kim BC, et al. Guillain-Barre syndrome associated with scrub ty- phus. Scand J Infect Dis 2007; 39: 826-828
8. Kim KW, Kim YH, Kim BH, Lee CY, Oh MS, Yu KH, et al. Miller Fisher syndrome related to Orientia tsutsuga- mushi infection. J Clin Neurosci 2014; 21: 2251-2252 9. Artemiadis AK, Zis P. Neuropathic Pain in Acute and
Subacute Neuropathies: A Systematic Review. Pain Physi- cian 2018; 21: 111-120
10. Amato AA, Dumitru D. Acquired neuropathies. In:
Dumitru D, Amato AA, Zwarts M, editors. Electrodiag- nostic medicine, 2nd ed, Philadelphia: Hanley & Belfus, 2002, 937-946