65
Copyright ⓒ 2015 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received August 26, 2014 Revised October 29, 2014 Accepted November 26, 2014
Address reprint requests to: Youn-Soo Kim, M.D.
Department of Orthopedic Surgery, The Catholic University of Korea, Buchon St. Mary’s Hospital, 327 Sosa-ro, Wonmi-gu, Bucheon 420-717, Korea
Tel: 82-32-340-7036 ㆍFax: 82-32-340-2671 E-mail: [email protected]
Financial support: None. Conflict of interest: None.
Irreducible Open Dorsal Dislocation of the Proximal Interphalangeal Joint - A Case Report -
Youn-Tae Roh, M.D.*, Il-Jung Park, M.D., Hyoung-Min Kim, M.D., Jae-Young Lee, M.D., Sung-Lim You, M.D., Youn-Soo Kim, M.D.
Department of Orthopedic Surgery, The Catholic University of Korea, School of Medicine, Seoul, Department of Orthopedic Surgery, Uijeongbu Paik General Hospital*, Uijeongbu, Korea
Dorsal dislocation of the proximal interphalangeal joint is a common injury in the orthopedic department. In most cases, the joint is reduced simply by closed manipulation. However, in rare cases, the joint is not reducible by closed manipulation, therefore, surgery is required. We report on a case of irreducible open dorsal dislocation of the proximal interphalangeal joint which was surgically treated. Because the flexor tendon interposed between the head of the proximal phalanx and the base of the middle phalanx, we could reduce the joint only after repositioning of the flexor tendon.
Key Words: Irreducible dislocation, Proximal interphalangeal joint, Flexor tendon
근위 지간 관절의 탈구는 정형외과 영역에서 자주 접하 는 수부 손상 중 하나로, 주로 과신전 손상에 의한 후방 탈구의 형태로 나타난다.1) 대개 단순 조작만으로도 쉽게 정복이 가능하나 드물게 도수 조작으로 정복이 되지 않아 관혈적 정복이 필요한 경우도 있다. 저자들은 근위 지간 관절의 개방성 후방 탈구에서 굴곡건에 의하여 도수 정복
이 되지 않아 수술적 정복술을 시행한 증례를 경험하였기 에 문헌 고찰과 함께 보고하는 바이다.
증례 보고
68세 남자가 계단에서 넘어지며 발생한 좌측 환지의 동 통과 열상을 주소로 내원하였다. 신체 검사상 좌측 환지 근위 지간 관절부에 2 cm 크기의 열상과 함께 변형이 관 찰되었다. 열상을 통해 근위지골의 골두가 피부 밖으로 노 출되어 있었으며, 근위 지간 관절의 굴곡 및 신전이 불가 능하였다. 단순 방사선 검사상 근위 지간 관절의 후방 및 척측 탈구가 관찰되었다(Fig. 1). 응급실에서 도수 정복을 시도하였으나 정복이 되지 않아 관혈적 정복술을 시행하기 로 하였다. 자기공명영상(magnetic resonance imaging) 검
Fig. 1. Radiographs showed the dorsoulnar dislocation of the proximal interphalangeal joint.
Fig. 2. Preoperative magnetic resonance imagings. The flexor digitorum profundus tendon interposed between the head of the proximal phalanx and the base of the middle pha- lanx. (A) Sagittal images. (B) Coronal images.
사상 파열된 수장판과 굴곡건이 근위지골 골두와 중위지골 기저부 사이에 끼여 있는 것을 확인할 수 있었다(Fig. 2).
액와 마취 후 수장측의 개방창을 연장하여 관혈적 정복 술을 시행하였다. 수술 소견상 좌측 환지 근위 지간 관절 의 수장판이 근위부에서 완전 파열되어 있었으며, 굴곡건 이 근위지골 골두 척측 과(condyle)의 후방으로 위치하여
탈구된 중위지골이 원래 위치로 돌아가는 것을 방해하고 있었다(Fig. 3). 이에 둔한 탐침(probe)을 이용하여 근위지 골과 중위지골 사이에 위치한 굴곡건을 들어 올려 원래 위 치인 근위지골의 수장측으로 재위치시킨 후 근위 지간 관 절을 정복할 수 있었다. 파열된 수장판을 부착부 주변 연 부조직과 봉합하고, K-강선을 이용하여 근위 지간 관절을
proximal phalanx protruded through the palmar open wound. (B) Flexor digitorum profundus tendon (black arrow head) had slipped behind the condyle of the proximal pha- lanx.
Fig. 4. Postoperative radio- graphs showed well-reduced state of the proximal inter- phalangeal joint.
30도 굴곡 위치에서 고정하였다(Fig. 4). 이후 세척술 및 피부를 봉합한 후 수술을 마쳤다.
2주간 단상지 부목 고정을 하였으며, 술 후 3주에 관절 을 고정하던 K-강선을 제거하고 근위 지간 관절 운동을 시 작하였다. 수술 후 6개월 추시에서 통증은 완전히 소실되 었으며, 관절 운동 범위는 굴곡 구축 5도에서 완전 굴곡이 가능하였다(Fig. 5).
고 찰
근위 지간 관절의 탈구 중 가장 흔한 형태는 후방 탈구 이다. 주로 관절이 과신전 되고 종적인 압박력을 받아 발 생하는 것으로, 공이 손가락 끝에 부딪히는 경우가 좋은 예이다. 단순 탈구의 경우 대개 측부 인대는 기능적으로 온전하게 남아 있고 수장판은 원위 부착부에서 파열되며 종종 중위지골의 기저부에 작은 견열 골절을 동반하기도 한다. 보다 큰 압박력이나 전단력이 작용할 경우 중위지골
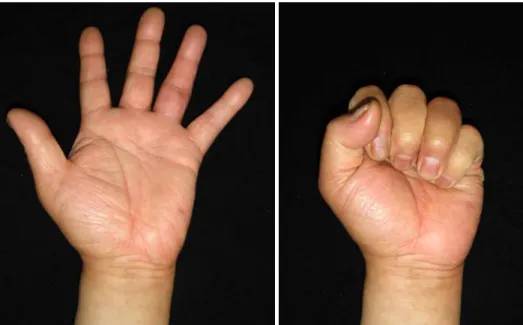
Fig. 5. At six months after the operation, there was mild swelling at the proximal in- terphalangeal joint. However, the patient regained a nearly normal range of motion.
Table 1. Summary of Cases
Patient No. Age (yr)/sex Affected finger Cause of injury PIP joint ROM (extension/flexion)
Structures interfering with reduction
1 60/male Ring Fall –20o/15o flexion limitation Flexor tendon
2 17/male Little Football –10o/90o Flexor tendon
3 51/female Middle Fall –65o/full Flexor tendon, volar plate
4 37/male Ring Fall –45o/100o Flexor tendon, volar plate
5 18/male Ring After a kick –20o/100o Flexor tendon, volar plate
6 30/male Little Handball Full ROM Flexor tendon, volar plate
7 19/male Little Volleyball –10o/full Flexor tendon, volar plate
8 39/male Middle Baseball 0o/100o Flexor tendon, volar plate
PIP: Proximal interphalangeal joint, ROM: Range of motion.
기저부에 큰 골절편을 만드는 골절-탈구 형태의 손상이 발 생할 수 있다.1,2)
골절을 동반하지 않는 후방 탈구는 크게 두 가지 형태로 구분된다. 제1형은 관절면의 접촉이 있으면서 중위지골이 근위지골에 대해 과신전 형태의 변형을 보이는 경우로, 약 간의 수장측 전이와 굴곡만으로 쉽게 정복이 가능하다. 제 2형은 중위지골이 근위지골에 대하여 총검형 위치(bayonet position)에 있는 것으로 제1형과는 다른 방법으로 정복이 이루어져야 한다. 즉, 중위지골에 신전 모멘트를 가하고 술 자의 엄지 손가락으로 중위지골의 기저부를 눌러 관절면을 접촉시킨 후 정복을 하여야 하며, 단순 견인을 이용하여 정복을 시도할 시에는 정복되지 않는 탈구로 변할 수 있 다.1) 정복이 되지 않는 탈구의 경우 수장판, 건, 측부 인 대, 관절 내 골편 등이 근위 지간 관절의 정복을 방해할 수 있으며,3) 이러한 경우 수장측 절개를 통한 관혈적 정복
술이 권장되고 있다.
Kilgore 등4)은 근위 지간 관절에 과신전 손상뿐 아니라 회전력이 함께 가해져 탈구가 발생하게 되면 근위지골의 골두가 수장판과 굴곡건 사이로 돌출되어 굴곡건이 근위지 골과(proximal phalangeal condyle) 후방으로 전위되어 정 복을 방해할 수 있다고 하였고, 이러한 경우 일반적인 도 수 정복으로는 근위 지간 관절의 정복을 얻을 수 없으며 굴곡건을 근위지골과 전방으로 재위치시켜야만 정복을 얻 을 수 있다고 하였다. 또한 Takami 등5)은 중위지골 기저 부의 관절면이 근위지골 골두의 관절면보다 작기 때문에 탈구가 발생하였을 경우 종적인 견인을 가하게 되면 굴곡 건, 신전건, 그리고 수장판이 신연되면서 근위지골 골두가 들어갈 공간을 오히려 좁게 만든다고 하였다. 따라서 이러 한 손상에서는 종적인 견인을 가하지 말고 탐침 등을 이용 하여 굴곡건을 들어 올려주면 근위지골 골두가 들어갈 수
는 정복을 얻을 수 없어 관혈적 정복술을 시행하였다. 모 든 예에서 수장측의 개방창을 통하거나 이를 연장하여 수 술을 시행하였고, 굴곡건을 근위지골 과의 전방으로 재위 치시킨 후 관절의 정복을 얻을 수 있었다. 후방 접근법 등 추가 절개를 시행한 경우는 없었다. 술 후 2-3주에 관절 운동을 시작하였고 대부분의 증례에서 관절의 불안정성 없 이 만족스러운 결과를 보였다. 그러나 Green과 Posner6)가 보고한 2예에서는 근위 지간 관절의 굴곡 구축이 45도, 65 도로 신전 운동이 제한되는 소견을 보였는데, 이는 환자가 수술 이후 관절 운동 제한에 대한 치료를 원하지 않았고, 알코올 중독으로 수술 후 재활 치료를 잘 따르지 않았던 경우였다(Table 1의 patient No. 3, 4).
저자들은 도수 정복으로 정복되지 않은 근위 지간 관절 의 개방성 후방 탈구 1예를 경험하고 수술적 치료로 좋은 결과를 얻었기에 문헌 고찰과 함께 보고하는 바이다. 본 증례와 같이 수장측에 열상을 동반한 근위 지간 관절의 후 방 탈구는 단순한 과신전 손상이 아닌 회전력을 동반된 복 잡 탈구의 가능성이 높다. 따라서 열상으로 골두가 돌출되 어 있고 도수 조작으로 쉽게 정복이 되지 않을 경우 굴곡
the finger joints. J Hand Surg Am, 34: 1140-1147, 2009.
3) Muraoka S, Furue Y, Kawashima M: Irreducible open dorsal dislocation of the proximal interphalangeal joint: a case report. Hand Surg, 15: 61-64, 2010.
4) Kilgore ES Jr, Newmeyer WL, Brown LG: Post-trau- matic trapped dislocations of the proximal interphalangeal joint. J Trauma, 16: 481-487, 1976.
5) Takami H, Takahashi S, Ando M: Irreducible open dor- sal dislocation of the proximal interphalangeal joint. Arch Orthop Trauma Surg, 121: 232-233, 2001.
6) Green SM, Posner MA: Irreducible dorsal dislocations of the proximal interphalangeal joint. J Hand Surg Am, 10:
85-87, 1985.
7) Kjeldal I: Irreducible compound dorsal dislocations of the proximal interphalangeal joint of the finger. J Hand Surg Br, 11: 49-50, 1986.
8) Stern PJ, Lee AF: Open dorsal dislocations of the prox- imal interphalangeal joint. J Hand Surg Am, 10: 364-370, 1985.
Copyright ⓒ 2015 The Korean Fracture Society. All rights reserved.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/
by-nc/3.0) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
가톨릭대학교 의과대학 정형외과학교실, 의정부백병원 정형외과*
근위 지간 관절의 후방 탈구는 정형외과 영역에서 자주 접하는 수부 손상 중 하나이다. 대부분의 경우 단순한 도수 조작만으로도 쉽게 정복이 되나, 드물게 도수 조작으로 정복이 되지 않아 수술적 정복이 필요한 경우도 있다. 저자들은 근위 지간 관절의 개방성 후방 탈구에서 굴곡건에 의하여 도수 정복이 되지 않아 수술적 정복술을 시행한 증례를 보고하고자 한다. 굴곡건이 근위지골의 골두와 중위지골의 기저부 사이에 감입되어 있어 탐침자를 이용하여 굴곡건을 제 위치로 옮긴 후에야 비로소 정복을 얻을 수 있었다.
색인 단어: 정복되지 않는 탈구, 근위 지간 관절, 굴곡건
접수일 2014. 8. 26 수정일 2014. 10. 29 게재확정 2014. 11. 26 교신저자 김 윤 수
부천시 원미구 소사로 327, 가톨릭대학교 부천성모병원 정형외과 Tel 032-340-7036, Fax 032-340-2671, E-mail [email protected]
70