Fukuyama congenital muscular dystrophy (FCMD) is a genetic disease with an autosomal recessive mode of inheritance (1, 2). It is most common in Japanese pa- tients and is the second most common form of muscular dystrophy in Japan, after Duchenne muscular dystro- phy (2). FCMD causes severe mental retardation, seizures, muscular weakness soon after birth, and pathologic muscular changes that are consistent with muscular dystrophy. The typical clinical features are hy- potonia with early infantile onset, and severe develop- mental delay (1), and diagnosis is based on pathologic evidence of muscular dystrophy revealed by biopsy or increased serum creatine kinase levels. Since the neuro- logic assessment of young infants is not always straight-
forward, however, definite diagnosis is occasionally dif- ficult, and in this respect, MRI may be helpful; the modality readily demonstrates various brain malforma- tions occurring in FCMD, and may therefore facilitate diagnosis(3-6). The findings of MRI and neuropatholo- gy have four known categories: cerebral cortical malfor- mations, cerebellar malformations, white matter changes, and miscellaneous abnormalities (7). We pre- sent the MRI findings of a typical case of FCMD.
Case Report
A 4-month-old male patient was admitted due to hypo- tonia, sucking difficulty and developmental delay, though initial crying was good. He was born at 40 weeks gestation by difficult vaginal delivery, and birth weight was 3.4Kg. Due to poor sucking power he was admitted to a local clinic during his third day of life and was treat- ed under the impression of aspiration pneumonia.
MR Imaging of Fukuyama Congenital Muscular Dystrophy: A Case Report1
Jeonghyun Yoo, M.D., Yookyung Kim, M.D., Haesoo Koo, M.D.2, Ki Deuk Park, M.D.3
Fukuyama congenital muscular dystrophy is a genetic disease and common in Japan. The typical clinical features are hypotonia with an early infantile onset and se- vere developmental delay. The diagnosis is based on pathologic evidence of muscular dystrophy revealed by biopsy or an increased serum creatine kinase levels.
Involvement of the brain is characterized by abnormal cerebral cortical dysplasia, cerebellar dysplasia, and white matter changes. We encountered a case of Fukuyama congenital muscular dystrophy in which brain MRI findings were typical, and present this case together with a review of the literature.
Index words : Infants, newborn, central nervous system Infants, newborn, skeletal system
Brain, MR
1Department of Diagnostic Radiology, College of Medicine, Ewha Womans University
2Department of Anatomical Pathology, College of Medicine, Ewha Womans University
3Department of Neurology, College of Medicine, Ewha Womans
when ten years old.
Other than motor weakness, physical and neurologi- cal examinations showed no significance abnormal find- ings. The serum creatine kinase (CK) level was 1,330 (normal range 5-130) IU/l, and lactic dehydrogenase (LDH) was 1,780 (normal range 58-170) IU/l. EMG showed a diffuse myopathic process in muscles of the upper and lower extremities, compatible with congeni- tal muscular dystrophy. Muscle biopsy of the vastus rec- tus muscle was performed, revealing extensive degener- ated myofibers, fibrosis, and distorted myofilaments, but preserved myofiber structures. These findings were consistent with congenital muscular dystrophy.
MR was performed on a 1.5-T imaging system (Siemens, Erlangen, Germany), and T1- and T2-weight- ed spin-echo images were obtained. Myelination was present in the internal capsule and corpus callosum, but
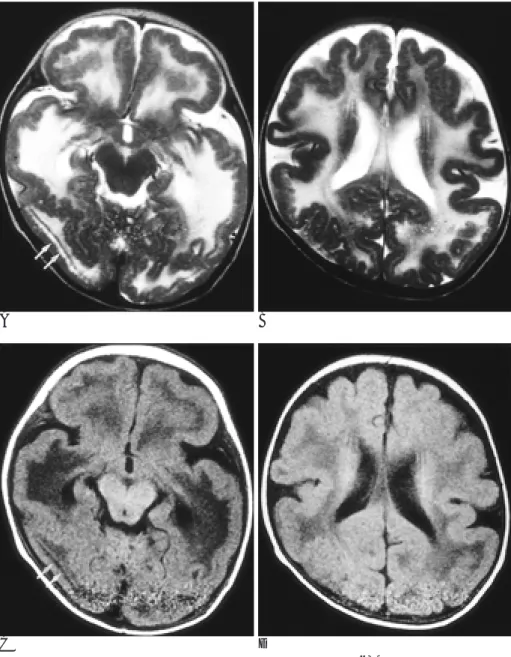
in other parts of the brain was absent. T2-weighted im- ages revealed symmetric unmyelineated white-matter changes, with extensive high signal intensities (Fig. 1).
Pachygyria were prominent in both occipitotemporal lobes, and in the frontoparietal region, some polymicro- gyria were also present (Fig. 1). In addition, curvilinear bands with high signal intensity on T2-weighted images were noted in deep layers of the pachygyric cortices (Fig. 1). Cerebellar MRI showed diffuse cortical abnor- malities with distorted folia, and multiple, small intra- parenchymal cysts, about 1-2mm in diamater, in the posterior aspect of the hemispheres (Fig. 2).
Discussion
Congenital muscular dystrophy comprises a heteroge- neous group of disorders characterized by muscular hy-
A B
Fig. 1. Axial T2-weighted (A), (B) and T1-weighted (C),(D) MR images. The temporo-occipital lobes show thick cortices with smooth surface (pachy- gyria) and some frontoparietal lobes show slightly thick cortices with shal- low sulci (polymicrogyria). The white matter changes are symmetric and ex- tensive with low signal intensity on T1-weighted image and high signal in- tensity on T2-weighted image. And curvilinear bands presented deep within the pachygyric cortices (ar- rows) are also noted with low signal intensities on T1-weighted image and high signal intensities on T2-weighted image which may represent unmyeli- nated fibers in the third layer of pachygyria.
potonia and histologic features of muscular dystrophy (1, 2). On the basis of clinical features, pathologic findings, and pattern of inheritance, four distinct phenotypes are currently recognised : classic congenital muscular dystro- phy, FCMD, muscle-eye-brain disease (MEBD), and Walker-Warburg syndrome(WWS) (8).
Patients with classic congenital muscular dystrophy exhibit normal intelligence, while those with FCMD, MEBD, and WWS have CNS malformations. In all three entities the clinical phenotypes are severe, and include severe mental retardation. WWS is the phenotype in which the more severe disorders occur, and is associat- ed with type-II lissencephaly and ocular abnormali- ties(5, 8, 9). Brain malformations in WWS usually in- clude agyral malformation, hypomyelination of white matter, and hydrocephalus, and these conditions are more severe and diffuse than in FCMD. In addition, cerebellar hypoplasia, cephalocele, and absence of the corpus callosum occasionally occur in WWS but not in FCMD(7-9). The pachygyria seen in MEBD is less pro- nounced than in FCMD, and agyria, seen in approxi- mately half of FCMD cases, has not been reported(6-8).
The distribution of gyral malformations seen in MEBD , which differe from those found in FCMD, include pachygyria over the frontal, temporal, and parietal re- gions, and polymicrogyria over the occipital region.
Additionally, dysplasia of the septum pellucidum and corpus callosum are frequently seen in MEBD, but are rare in FCMD (7, 8).
Our patient showed delayed development, indicating associated CNS malformations in addition to muscle weakness. Brain MRI showed pachygyria in the occipi-
totemporal lobe and polymicrogyria in the frontopari- etal lobe, findings distinct from those seen in MEBD.
There was no dysplasia of the septum pellucidum and/or corpus callosum, a condition seen in MEBD and WWS.
The characteristic brain MR findings in FCMD in- clude four abnormalities : cerebral cortical malforma- tions, cerebellar malformations, white matter changes, and miscellaneous abnormalities (7). The histologic fea- tures of cerebral cortical malformations of FCMD have been divided by Takada et al.(3, 4) into three types : ver- rucose dysplasia (type 1), unlayered polymicrogyria (type 2), and the most severe type of cortical dysplasia (type 3), which is identical to type-II lissencephaly. For each type of cortical dysplasia, a characteristic regional distribution is also described: a predilection for the me- dial surface of the occipital lobe in type 1, for the frontal and parietal lobes in type 2, and for the lateral surface of the occipital and temporal lobes in type 3. MRI can demonstrate type-2 and -3 cortical dysplasia , but is un- able to detect type-1 (6). Type-2 cortical dysplasia, un- layered polymicrogyria, is depicted as a slightly thick cortex with shallow sulci, and a gray-white matter inter- face which has a bumpy appearance. These radiologic findings are typical. Type-3 cortical dysplasia presents as a thick cortex with a smooth surface, typical radi- ographic findings of pachygyria. Aida et al. (5) reported that type-2 dysplasia involved the frontal lobe in all, the cases they studies, and that type-3 involved the tem- porooccipital lobe in one-half. An increased number of curvilinear signal bands deep within abnormal cortices are detected in half of type-3 cases (7), appearing in the
Fig. 2. Axial T2-weighted (A) and T1- weighted MR images (B) of the cere- bellum. The T2-weighted image shows diffuse cortical abnormalities with disorganized and distorted folia.
Multiple, various sized intraparenchy- mal cysts (arrows) are seen in the pos- terior aspect of the hemispheres with low signal intensities on T1-weighted image and bright signal intensities on T2-weighted image.
third layer of such cases as unmyelinated fibers (6). The pathogenesis of cortical malformations in FCMD re- mains speculative. Takada et al.(4) suggested that the pi- al-glial barrier might be disrupted in FCMD, leading to the development of neuroglial heterotopias within the extracortical glial layer.
Two hallmarks of cerebellar malformations in FCMD are cerebellar polymicrogyria and intraparenchymal cyst (3, 5). In most cases, cerebellar malformation is re- stricted to the superior semilunar lobules, but it is occa- sionally more diffuse (3, 5). The sulci are often obliterat- ed by the fusion of malformed cerebellar folia, and small cystic lesions are usually located beneath the mal- formed cerebellar cortex, in areas of polymicrogyria.
The cystic lumina contain leptomeningeal tissue, and the walls are lined by a parenchymal tissue composed of a histologically-nearly-normal molecular layer (7). The process by which cerebellar cysts develop in FCMD is unknown. The assumption is that the cysts may repre- sent dilated subarachnoid spaces engulfed within the cerebellar parenchyma by fusion of the folia of the mal- formed cortex (5, 6). These cysts can be observed more easily than the cerebral cortical dysplasia present in FCMD, though they are not specific to FCMD and can arise in other types of congenital muscular dysplasia.
T2-weighted MR imaging of white-matter changes demonstrates diffusely increased signal intensities (7, 8, 10), though the cause of white-matter abnormality in FCMD has not been clearly explained. Myelin pallor and mild gliosis have been mentioned as possible causes (1-3), though on account of the way in which white-mat- ter changes spontaneously regress, the neuroradiologic literature on FCMD has attributed them to delayed myelination (10). In the report by Aida et al. (5), howev- er, the progressive myelination of white matter occuring in FCMD is described as centripetal rather than cen- trifugal, as in normal myelination, and this contradicts the hypothesis that delayed myelination is the cause of white matter abnormalities in FCMD (7).
In cases of FCMD, miscellaneous abnormalities such as enlarged subarachnoid space, ventriculomegaly due to hypoplasia, and a flattened ventral portion of the pons have been reported (6).
than FCMD, with the occurrence of type-II lissencephaly, cerebellar anomalies, and associated ocu- lar abnormalities (5, 8, 9). Gyral abnormalities are more severe and more diffuse, and white-matter involvement is more widespread than in FCMD. This latter, howev- er, is associated with less severe cerebellar anomalies, and ocular involvement is less constant. The symptoms of MEBD are less pronounced those of FCMD (5, 7, 9).
Dysplasia of the septum pellucidum and corpus callo- sum, frequently seen in MEBD and WWS, are rare find- ings in FCMD (7).
Traditionally, the diagnosis of FCMD has depended on the clinical findings and a muscle biopsy.
Nevertheless, it is difficult to assess the neurologic status of a young infant, and a muscle biopsy does not provide specific evidence of FCMD beyond the mere diagnosis of muscular dystrophy. The MR findings are thus useful for the early diagnosis of FCMD and may permit a cor- rect diagnosis.
References
1. Fukuyama Y, Osawa M, Suzuki H. Congenital progressive muscu- lar dystrophy of the Fukuyama type : clinical, genetic and patologi- cal considerations. Brain Dev 1981;3:1-29
2. Menkes JH. Textbook of Child Neurology, 4th ed. Philadelphia:Lea
& Febiger, 1990;690-691
3. Takada K, Nakamura H, Tanaka J. Cortical dysplasia in congenital muscular dystrophy with central nervous involvement (Fukuyama type). J Neuropathol Exp Neurol 1984;43:395-407
4. Takada K. Fukuyama congenital muscular dystrophy as a unique disorder of neuronal migration : a neuropathological review and hypothesis. Yonago Actmedica 1988;31:1-16
5. Aida N, Yagishita A, Takada K, Katsumata Y. Cerebellar MR in Fukuyama congenital muscular dystrophy : polymicrogyria with cystic lesions. AJNR Am J Neuroradiol 1994;15:1755-1759 6. Aida N, Tamagawa K, Takada K, et al. Brain MR in Fukuyama
congenital muscular dystrophy. AJNR Am J Neuroradiol 1996;17:
605-613
7. Aida N. Fukuyama congenital muscular dystrophy : a neuroradio- logic review. J Magn Reson Imaging 1998;8:317-326
8. Philpot J, Dubowits V. Congenital muscular dystrophies. In : Rimon RL, Conner JM, Pyerits RE, eds. Principles and practice of medical genetics. 3rd ed. New York : Churchil Livingstone. 1996 9. Rhodes RE, Hatten HP Jr. Ellington KS. Walker-Warburg syn-
drome. AJNR Am J Neuroradiol 1992;13:123-126
10. Yoshioka M, Saiwai S, Kuroki S, Nigami H. MR imaging of the brain in Fukuyama type congenital muscular dystrophy. AJNR Am J Neuroradiol 1991; 12:63-65
대한방사선의학회지 2000;43:629-633
Fukuyama 선천성 근이영양증의 뇌자기공명영상소견: 1예 보고1
1이화여자대학교 의과대학 진단방사선과학교실
2이화여자대학교 의과대학 해부병리학교실
3이화여자대학교 의과대학 신경과학교실
유정현・김유경・구혜수2・박기덕3
Fukuyama 선천성 근이영양증은 일본에서 흔한 유전성 질환으로, 영아초기에 발병하는 긴장저하와 심한 발달장 애가 특징적인 임상 소견이다. 병리조직검사상 근이영양증을 확인하거나 혈청 creatine kinase의 증가로 진단할 수 있다. 특징적인 뇌의 병변은 비정상적 대뇌피질의 이형성증, 소뇌이형성증, 대뇌백질변화 등이다. 저자들은 Fukuyama 선천성 근이영양증을 특징적인 뇌자기공명영상 소견과 함께 경험하였기에 문헌고찰과 함께 보고하는 바이다.
라는 제목의 논문이 대한방사선의학회지에 출간될 경우 그 저작권을 대한방사선의학회에 이전한다.
저자는 저작권이외의 모든 권한 즉, 특허신청이나 향후 논문을 작성하는데 있어서 본논문의 일부 혹은 전부를 사용하는 등의 권한을 소유한다. 저자는 대한방사선의학회지로부터 서면허가를 받으면 타논문에 본논문의 자료 를 사용할 수 있으며 이 경우 자료가 발표된 원논문을 밝힌다. 본논문의 모든 저자는 본논문에 실제적이고 지적인 공헌을 하였으며 논문의 내용에 대하여 공적인 책임을 공유한다.
본논문은 과거에 출판된 적이 없으며 현재 타학술지에 제출되었거나 제출할 계획이 없다.
본 동의서는 원고에 기술된 순서대로 전 저자의 서명이 있어야 함.
대한방사선의학회 원고 최종 점검표
원고 1부, 사진 1부를 동봉한다.
행간 여백 1행(double space)에 21×30cm (A4)용지에 작성한다.
원고배열은 한글과 영문으로 기재된 표지, 내표지, 초록(한글과 영문), 서론, 대상과 방법, 결과, 고찰, 참고문헌, 표, 사진설명의 순으로 한다.
초록은 목적, 대상과 방법, 결과, 결론으로 나누어 기술한다.
영문초록 하단에 색인단어 (Index Words)를 기입한다.
저작권에 관한 동의서에 전 저자가 서명한다.
제 1 저 자 / 년 월 일 제 2 저 자 제 3 저 자
제 4 저 자 제 5 저 자 제 6 저 자
[ 분 야 : ]