90
책임저자: 박민호, 전남 화순군 화순읍 일심리 160
519-809, 화순전남대학교병원 외과 Tel: 061-379-7646, Fax: 061-379-7661 E-mail: [email protected]
접수일:2010년 10월 7일, 게재승인일:2010년 12월 31일 이 논문은 전남대학교병원 임상의학연구소 학술연구비(CRI09079-1) 에 의하여 연구되었음.
수술 전 관상피내암으로 진단되었던 환자에서 침윤성 유방암이 발견될 위험 인자
화순전남대학교병원 외과
신선형ㆍ김병천ㆍ송영주ㆍ윤현철ㆍ조진성ㆍ박민호ㆍ윤정한ㆍ제갈영종
Risk Factor of Invasive Breast Cancer in Patients with Preoperative Diagnosis of Ductal Carcinoma in Situ
Sun Hyoung Shin, M.D., Byung Chun Kim, M.D., Young Ju Song, M.D., Hyun Chul Yoon, M.D., Jin Seong Cho, M.D., Min Ho Park, M.D., Jung Han Yoon, M.D., Young Jong Jegal, M.D.
Department of Surgery, Chonnam National University Hwasun Hospital, Hwasun, Korea
Purpose: Ductal carcinoma in situ (DCIS), unlike invasive ductal carcinoma, does not require sentinel lymph node biopsy or axillary lymph node dissection because the possibility of axillary lymph node metastasis is low. However, occasionally, despite preoperative diagnosis of DCIS, invasive ductal carcinoma can be diagnosed by postoperative biopsy. Therefore, a study of the associated risk factors is necessary.
Methods: 198 patients with an initial diagnosis of DCIS, treated between February 2005 and December 2009, were retrospectively analyzed. Associations between clinical and pathologic factors were analyzed for significance using univariate and multivariate analyses.
Results: Of the 198 patients, 57 (28.8%) were found to have invasive disease on final pathology. Multivariate analysis revealed 4 independent predictors of invasive cancer upon final pathology: diagnosis by needle biopsy (OR, 3.165; P=0.008), positive p53 on preoperative biopsy (OR, 2.494; P=0.019) DCIS size (>2 cm) on microscopic finding (OR, 2.683; P=0.014), and relatively young age (OR, 0.958, P=0.046). Of the 13 patients with positive axillary lymph nodes, 11 (84.6%) were shown to have invasive cancer on final pathology (P<0.001).
Conclusion: In cases of preoperative diagnosis based on needle biopsy, positive p53, large tumor, and relatively young age, an SLNB procedure can be considered because in almost 30% of the patients an invasive carcinoma is found after surgery. (J Korean Surg Soc 2011;80:90-95)
Key Words: Ductal carcinoma in situ, Invasive breast cancer 중심 단어: 관상피내암, 침윤성 유방암
서 론
관상피내암은 유방암에 대한 인식의 발전 및 진단 기술 의 발달로 점차 그 비중이 증가하여 현재 한국에서 약 8.1%,(1) 서양에서는 20∼25%로 보고되고 있다.(2) 관상피 내암의 수술적 치료는 아직까지 논란이 있으나 유방절제술 과 유방보존술 및 방사선 치료의 병합이 주로 권유되고 있 다. 관상피내암이 액와림프절로 전이될 확률은 약 1%로 보
DICS* Invasive
carcinoma P-value Age
Mean age 51.7 (±10.7) 48.2 (±8.9) 0.021 Symptoms
Screening 97 (68.8%) 27 (47.4%) 0.004 Palpable mass 30 (21.3%) 21 (36.8%) 0.020
Mastalgia 3 (2.1%) 5 (8.8%) 0.046
Nipple discharge 11 (7.8%) 4 (7.0%) 0.557 Palpation by clinician 62 (44.0%) 36 (63.2%) 0.011
Operation method 0.450
BCS† 76 (53.9%) 32 (56.1%)
Mastectomy 65 (46.1%) 25 (43.9%)
Total 141 57
*DCIS = ductal carcinoma in situ; †BCS = breast conserving surgery.
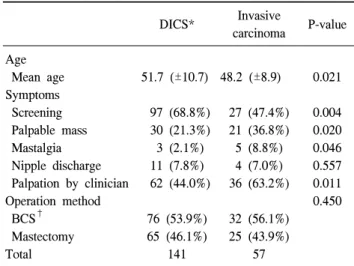
Table 1. The relation of invasiveness with age distribution, clinical presentations and operation methods
고되며(3,4) 액와림프절 절제술은 전이 확률에 비해 그 합 병증과 위험성이 높다고 하여 추천되지 않았으나, 이와 관 련되어 끊임없이 제기되는 문제는 수술 전 관상피내암으로 진단된 환자 중 약 19∼35%가 침윤성 유방암으로 최종 진 단된다는 것이다.(5) 침윤성 유방암의 경우 종양의 크기가 2 cm 미만이어도 액와림프절 전이가 10∼40%까지 발생하 기 때문에,(6) 결국 수술 전 관상피내암으로 진단된 환자 중 약 10∼15%가 액와림프절 전이가 존재한다. 그래서 최근에 는 관상피내암으로 진단된 환자에서도 특정한 고위험군에 서는 감시림프절 생검술을 시행하자는 주장이 대두되고 있 다.(7,8)
본 연구에서는 수술 전 관상피내암으로 진단된 환자들 중 최종 조직검사 결과가 침윤성 또는 미세 침윤성 유방암 으로 병기 상향되게 하는 위험 인자들을 밝히고자 하였다.
방 법
2005년 2월부터 2009년 12월까지 수술 전 조직검사에서 관상피내암으로 진단되어 수술을 시행한 249명의 환자 중 감시림프절 생검술 이상을 시행하여 액와림프절 전이 여부 를 확인했던 198명의 환자를 대상으로 연구를 시행하였다.
198명의 환자를 최종 조직검사 결과에서 관상피내암으로 진단된 군(n=141)과 침윤성 또는 미세 침윤성 유방암으로 진단된 군(n=57)으로 분류하였으며 두 군에서 환자의 나이, 내원 동기, 종양의 위치와 크기, 종양의 수, 수술 방법, 액와 림프절 전이 여부, 진단을 위해 시행한 조직검사 방법을 비 교하였고, 조직검사에서 호르몬 수용체의 발현 여부 및 핵 등급, 조직학적 세부 특성 등을 비교 분석 하였다.
통계학적 분석은 SPSS, version 18.0 프로그램으로 카이제 곱 검정 및 평균비교를 이용하였고 다변량 분석을 위해 로 지스틱 회귀분석을 시행하였다. 통계학적 유의성 검정은 P 값이 0.05 미만인 경우를 유의한 것으로 정의하였다.
결 과
1) 림프절 전이
수술 전 관상피내암으로 진단 받고 수술 받은 전체 198명 의 환자 중 최종 조직검사 결과에서 관상피내암으로 진단 된 환자가 141명(71.2%), 침윤성 유방암은 42명(21.2%), 미 세 침윤성 유방암은 15명(7.6%)이었다. 이 중 액와림프절 전이가 있었던 환자는 모두 13명(6.6%)으로 최종 조직검사
결과가 침윤성 유방암으로 진단된 환자에서 9명으로 가장 많았고 미세 침윤성 유방암에서 2명, 관상피내암 환자에서 2명이 액와림프절 전이가 있었다.
2) 임상적 특성
평균 나이는 관상피내암 환자군에서 51.7세, 침윤성 유방 암 환자군은 48.2세였으며 두 군 간의 척도를 이용한 평균 비교에서 통계학적 의미가 있는 것으로 보여졌다(P=0.021).
내원 동기를 묻는 질문에서 단순 건강검진을 위해 내원한 환자가 두 군 모두에서 가장 많았고, 관상피내암 환자군 (n=97, 68.8%)에서 침윤성 유방암 환자군(n=27, 47.4%)에 비 해 의미있게 많았으며(P=0.004), 유방에 종괴가 촉지되거나 유방통이 있어 내원한 경우 침윤성 유방암으로 진단될 확 률이 더 높았다(P=0.020, P=046). 전문의에 의한 신체검사상 종괴가 촉지된 경우도 관상피내암 환자군(n=62, 44.0%)보 다 침윤성 유방암 환자군(n=36, 63.2%)에서 의미 있게 많았 다(P= 0.011). 유두 분비물 여부는 차이가 없는 것으로 나타 났고(P=0.56), 수술 방법에서 두 군간에 차이는 없었다 (Table 1).
3) 종괴의 특성
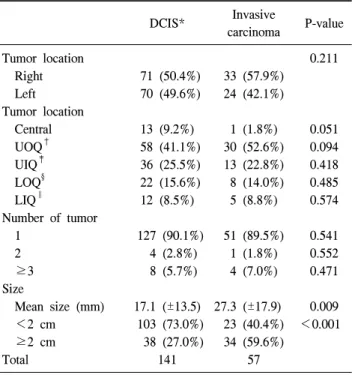
종괴의 좌우와 위치, 단발성 혹은 다발성 여부는 통계학 적 차이를 보이지 않았다. 종양의 크기는 최종 조직검사에 서 관상피내암의 장축을 측정하여 비교하였으며, 관상피내 암 환자에서 평균 17.1 mm, 침윤성 유방암 환자에서 평균
DCIS* Invasive
carcinoma P-value
Tumor location 0.211
Right 71 (50.4%) 33 (57.9%)
Left 70 (49.6%) 24 (42.1%)
Tumor location
Central 13 (9.2%) 1 (1.8%) 0.051
UOQ† 58 (41.1%) 30 (52.6%) 0.094
UIQ‡ 36 (25.5%) 13 (22.8%) 0.418
LOQ§ 22 (15.6%) 8 (14.0%) 0.485
LIQ∥ 12 (8.5%) 5 (8.8%) 0.574
Number of tumor
1 127 (90.1%) 51 (89.5%) 0.541
2 4 (2.8%) 1 (1.8%) 0.552
≥3 8 (5.7%) 4 (7.0%) 0.471
Size
Mean size (mm) 17.1 (±13.5) 27.3 (±17.9) 0.009 <2 cm 103 (73.0%) 23 (40.4%) <0.001 ≥2 cm 38 (27.0%) 34 (59.6%)
Total 141 57
*DCIS = ductal carcinoma in situ; †UOQ = upper outer quadrant;
‡UIQ = upper inner quadrant; §LOQ = lower outer quadran; ∥LIQ
= lower inner quadrant.
Table 2. The relation of invasiveness with tumor characteristics
DCIS* Invasive
carcinoma P-value Microscopic finding
Comedo type 65 (46.1%) 29 (50.9%) 0.325 Cribriform type 61 (34.3%) 10 (18.2%) 0.001 Papillary type 25 (17.9%) 6 (10.5%) 0.142 Solid type 52 (36.9%) 17 (29.8%) 0.219 Microcalcification 100 (70.9%) 35 (61.4%) 0.129 Necrosis 81 (57.4%) 41 (71.9%) 0.040
ER† 0.073
Positive 94 (66.7%) 31 (54.4%) Negative 47 (33.3%) 26 (45.6%)
PR‡ 0.002
Positive 93 (66.0%) 24 (42.1%) Negative 48 (34.0%) 33 (57.9%)
p53§ 0.001
Positive 34 (27.6%) 30 (54.5%) Negative 89 (72.4%) 25 (45.5%)
C-erb2 (3+) 39 (27.9%) 19 (33.3%) 0.275
Nuclear grade
1 (low) 25 (19.2%) 7 (12.5%) 0.343 2(intermediate) 75 (57.7%) 34 (60.7%) 0.468 3 (high) 30 (13.1%) 15 (26.8%) 0.316
Total 141 57
*DCIS = ductal carcinoma in situ; †ER = estrogen receptor; ‡PR
= progesterone receptor; §p53 = tumor protein 53.
Table 3. The relation of invasiveness with pathological subtype and molecular marker
DCIS* Invasive
carcinoma P-value Core needle biopsy 64 (45.4%) 45 (78.9%) <0.001 Excision biopsy 77 (54.6%) 12 (21.1%)
MGB† 39 (27.7%) 3 (5.3%)
Excision biopsy 24 (17.0%) 7 (12.3%)
Mammotome 14 (9.9%) 2 (3.5%)
Total 141 57
*DCIS = ductal carcinoma in situ; †MGB = mammography guid- ed excision biopsy.
Table 4. The relation of invasiveness with biopsy methods 27.3 mm로 관상피내암의 크기가 클수록 침윤성 유방암으
로 결과가 나올 확률이 더 높았다(P=0.009) (Table 2).
면포상(Comedo type), 유두상(Papillary type), 고형상(Solid type) 종양과 미세석회화 여부에서는 유의한 차이가 없었 다. 사상형(Cribriform)의 종양은 관상피내암일 확률이 더 높았으며(P=0.001) 내부 괴사를 포함한 경우 침윤성 유방암 일 확률이 더 높았다(P=0.040). 에스트로겐 수용체와 C-erb2 의 과 발현 여부는 차이를 보이지 않았으며 프로게스테론 수용체가 음성인 군(P=0.004)과 p53이 양성인 군(P=0.001) 에서 침윤성 유방암일 가능성이 유의하게 높은 것으로 나 타났다. 핵 등급에서는 차이를 보이지 않았다. 수술 전 검사 에서 p53 발현 여부와 핵등급의 결과가 각각 누락되어 있는 20명과 12명은 분석에서 제외하였다(Table 3).
수술 전 진단을 위한 조직검사 방법은 중심부 총생검술 과 절제생검으로 구분하였으며 절제생검으로는 유방 촬영 유도하 절제생검, 단순 종양 절제술, 맘모톰 절제술의 방법 이 있었다. 수술 전 중심부 총생검술로 관상피내암을 진단 받은 환자는 109명, 절제생검으로 진단받은 환자는 89명이 었고 중심부 총생검술로 진단받은 경우, 절제 생검을 시행 한 경우보다 최종 조직검사 결과가 침윤성 유방암으로 진
단될 확률이 더 높았다(45.4% (64/141) vs. 78.9% (45/57); P
<0.001) (Table 4).
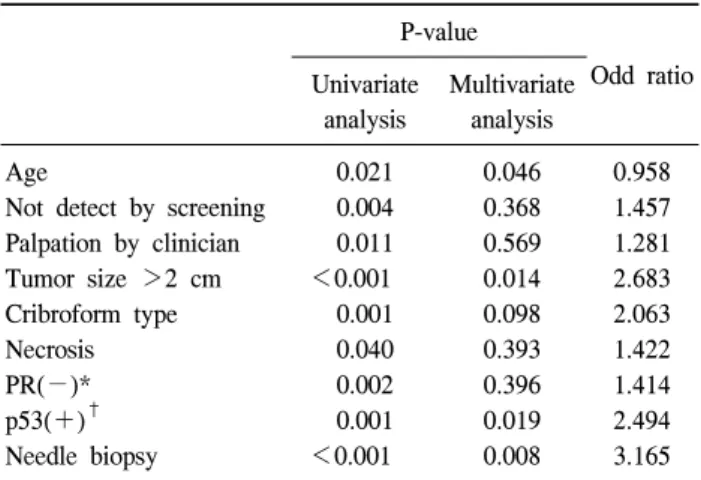
4) 침윤성을 예측하는 인자에 대한 다변량 분석 단변량 분석에서 침윤성을 예측하는 인자로서 의미를 보 였던 인자는 환자의 증상 유무, 촉지되는지 여부, 중심부 총
P-value
Odd ratio Univariate
analysis
Multivariate analysis
Age 0.021 0.046 0.958
Not detect by screening 0.004 0.368 1.457
Palpation by clinician 0.011 0.569 1.281
Tumor size >2 cm <0.001 0.014 2.683
Cribroform type 0.001 0.098 2.063
Necrosis 0.040 0.393 1.422
PR(−)* 0.002 0.396 1.414
p53(+)† 0.001 0.019 2.494
Needle biopsy <0.001 0.008 3.165
*PR = progesterone receptor; †p53 = tumor protein 53.
Table 5. Univariate and multivariate analysis of predictors of in- vasive breast cancer in patients with initial diagnosis of ductal carcinoma in situ
생검술로 진단받은 경우, 프로게스테론 수용체 음성 발현, p53 양성 발현, 내부 괴사를 포함한 경우, 사상형을 포함하 지 않은 경우, 종양의 크기가 큰 경우, 젊은 나이였다. 이 중 다변량 분석에서도 의미가 있었던 인자로는 중심부 총 생검술로 진단받은 경우와 p53의 양성 발현을 보이는 경우, 종양의 크기가 2 cm 이상인 경우와 젊은 나이였으며 이 중 중심총 생검술로 진단된 경우가 침윤성 유방암의 가장 큰 위험인자인 것으로 나타났다(Odd ratio=3.165).
고 찰
유방 관상피내암은 악성화 된 상피세포들이 유관의 기저 막에는 침윤하지 못한 상태로 암세포가 상피층에만 국한되 어 림프관 혹은 혈관으로의 전이는 없는 상태로 정의하고 있다.(8) 따라서 이론적으로는 림프절 전이가 있을 수 없으 나 실제로는 순수한 관상피내암의 약 1% 정도가 액와림프 절 전이가 동반된다. 알려진 위험 인자로는 젊은 나이, 수술 전 경피 바늘 검사를 시행한 경우, 종양의 크기가 클 때, 높 은 핵 등급 등이 있다.(9) 높은 핵 등급은 많은 연구에서 관 상피내암의 예후와 관련이 있거나 침윤성 암 포함 여부를 예측하는데 있어 도움이 된다고 하였으나,(9,10) 본 연구에 서 핵 등급은 침윤성 유방암의 예측과 관련을 보이지 않았 다.
중심부 총생검술의 경우 절제술을 대체할 수 있는 최소 침습적 방법으로서 사용이 많아지고 있는데 이는 절제생검 술에 비해 시술이 간단하며, 세침흡인 세포검사에 비해 민
감도가 높고 진단에서 비교적 높은 정확성을 가지기 때문 이다.(11,12) 그러나 Wahedna 등(13)은 중심부 총생검술로 관상피내암을 진단 받은 환자들을 대상으로 검사의 정확도 를 연구하였을 때 44%에서 침윤성 유방암이 발견되었다고 보고하였으며 Jackman 등(14)은 검사를 시행한 바늘의 크기 에 따라 그 정확도가 달라진다고 하였다. 최근에는 맘모톰 을 이용하면 많은 양의 조직을 빠르게 얻을 수 있어 암 진 단에 있어 높은 정확도를 얻을 수 있다는 연구가 있으 나,(15) 침윤성 유방암의 진단방법으로서 맘모톰의 역할은 아직 더 많은 연구가 필요하다. 반면, 절제생검에 비해 경피 바늘 검사는 진단의 정확도가 떨어지므로 수술 전 관상피 내암으로 진단되었더라도 반드시 감시림프절 생검술을 시 행하도록 하는 것은 여러 연구에서 일관되게 주장되고 있 다.(16,17) 본원에서는 절제술로 진단 받은 환자의 수술 후 최종 조직검사 결과가 일치하지 않는 경우 이전 조직에 대 한 정밀 재검사를 시행하고 있음에도 불구하고 종괴 절제 술을 통한 진단에서 관상피내암이었던 환자 중 13.5%가 수 술 후 침윤성 유방암으로 진단되었다. 유방 촬영술 유도하 절제 생검술과 맘모톰 절제술과 비교하여 단순 종양 절제 술의 경우 그 비율이 비교적 높은 것으로 보아 종괴의 핵 부위의 정확한 제거 술식이 관건인 것으로 보인다.
유방의 관상피내암은 유방촬영술 양상, 조직학적 특성, 분자생물학적 표지자에 따라 다양한 임상 경과 및 특성을 가지는 것으로 알려져 있는데 유방촬영술 검사에서 관상피 내암은 석회화 침착 소견을 보이는 경우가 많고 침윤성 유 방암에서는 종괴가 주로 관찰된다고 한다.(18,19) 조직학적 특성 중 면포상 존재 유무가 나쁜 예후와 관련이 있는 것으 로 보여지지만(20) 본 연구에서 면포상 존재는 침윤성 포함 정도와는 관련이 없는 것으로 보였으며 고형상, 유두상 등 도 마찬가지로 관련이 없었다. 사상형이 발견되는 경우 오 히려 침윤성 유방암일 확률이 더 적어진다는 결과가 나왔 으나 다변량 분석에서 의미 없었다. 그 외 높은 핵 등급, 괴 사의 존재가 상피내암의 예후 인자로서 관련이 있는 것으 로 알려져 있으며(21) 본 연구에서도 핵 등급의 차이는 없 었으나 괴사의 존재는 차이를 보였고 이는 종양의 크기와 관련이 있는 것으로 보여진다. 종양의 크기와 관련한 여러 연구들에서 크기가 클수록 침윤성 유방암이 많이 발견되 며,(22) 본 연구에서 최종 조직검사에서 측정한 관상피내암 의 크기를 평균 비교 했을 때 크기가 클수록 침윤성 유방암 일 가능성이 높았고 특히 크기를 2 cm 미만과 2 cm 이상으 로 구별하였을 때 그 차이가 확연하였다. 환자가 유방의 종
괴를 촉지하거나 유방통을 주소로 내원하여 관상피내암을 발견한 경우 단순 건강검진으로 발견된 경우보다 침윤성 유방암으로 나올 확률이 높은 것도 종괴의 크기가 클수록 환자의 자각 증상이 생기기 때문인 것으로 보인다.
젊은 나이는 관상피내암에서 재발과 관련하여 독립적인 예후 인자로 알려져 있으며 나이가 젊을수록 재발률이 높 다.(23) 이는 젊은 나이의 환자에서 진단된 관상피내암이 높은 핵등급을 가지거나 종양의 크기가 큰 경우가 많기 때 문으로, 본 연구에서 나이가 젊을수록 수술 후 침윤성 유방 암으로 진단될 확률이 더 높게 나타난 것도 이와 관련된 것으로 생각된다.
에스트로겐과 프로게스테론 수용체 발현은 관상피내암 과 침윤성 유방암에서 차이가 없는 것으로 보고되고 있으 며(24,25) 본 연구에서도 다변량 분석을 시행하였을 때 호 르몬 수용체 발현은 관련이 없는 것으로 보여진다. p53의 발현은 침윤성 유방암에서 좋지 않은 예후를 보이는 것으 로 알려져 있으나(26,27) 관상피내암에서의 침윤성 여부를 포함하는지에 대한 연구는 미흡하다. 본 연구에서는 수술 전 조직검사에서 p53이 양성으로 나온 경우 침윤성 유방암 을 포함한 경우가 더 많은 것으로 보여졌고, 수술 전 검사로 관상피내암을 진단받은 환자에서 침윤성 포함 여부를 예측 할 수 있는 효율적인 인자로 보여진다.
관상피내암의 수술적 치료에 있어 종양의 침윤성 포함 정도는 수술 범위를 결정하는데 중요한 요소로 작용한다.
최근 언급되고 있는 위험 요소 중 유방촬영술 소견, 핵 등 급, 면포형의 존재 등과의 관계는 본 연구에서 밝히지 못했 으나 중심부 총샘검술을 이용한 진단, 종양의 크기, 젊은 나 이 등이 침윤성 종양 포함을 예측할 수 있는 인자로 나타났 으며, 특히 수술 전 조직검사에서 p53이 양성으로 발현되었 을 때 관상피내암으로 진단되었더라도 침윤성 종양일 가능 성을 염두에 두고 수술 범위를 결정해야 할 것이다.
결 론
수술 전 관상피내암으로 진단받아 수술을 시행한 198명 의 환자 중 57명(28.8%)이 최종 조직검사에서 미세 침윤성 또는 침윤성 유방암으로 나왔다. 침윤성 유방암으로 병기 상향되는 위험 인자로는 경피 바늘 검사로 진단받은 경우 와 종양의 크기가 큰 경우, 비교적 젊은 나이로 보여지며 특히 수술 전 조직검사에서 p53이 양성으로 발현되는 경우 에도 침윤성 유방암으로 진단될 가능성이 높았다.
이러한 위험 인자를 가진 경우에는 수술 전 관상피내암 으로 진단되었더라도 침윤성 유방암일 가능성을 염두에 두 어야 하며 특히, 액와림프절의 전이율이 높아지므로 수술 중 감시림프절 생검술을 시행하여 액와 림프절 전이 여부 를 확인해야 한다.
REFERENCES
1) The Korean Breast Cancer Society. Nationwide Korean breast cancer data of 2002. J Korean Breast Cancer Soc 2004;7:
72-83.
2) Pendas S, Dauway E, Giuliano R, Ku N, Cox CE, Reintgen DS. Sentinel node biopsy in ductal carcinoma in situ patients.
Ann Surg Oncol 2000;7:15-20.
3) Zelis JJ, Sickle-Santanello BJ, Liang WC, Nims TA. Do not contemplate invasive surgery for ductal carcinoma in situ. Am J Surg 2002;184:348-9.
4) Leonard GD, Swain SM. Ductal carcinoma in situ, complex- ities and challenges. J Natl Cancer Inst 2004;96:906-20.
5) Morrow M, Venta L, Stinson T, Bennett C. Prospective com- parison of stereotactic core biopsy and surgical excision as di- agnostic procedures for breast cancer patients. Ann Surg 2001;233:537-41.
6) Ham HW. Incidence of axillary lymph node metastases in T1 breast cancer. J Korean Breast Cancer Soc 2002;5:142-6.
7) Leidenius M, Salmenkivi K, von Smitten K, Heikkila P.
Tumour positive sentinel node findings in patients with ductal carcinoma in situ. J Surg Oncol 2006;94:380-4.
8) Swain SM. Ductal carcinoma in situ. Cancer Invest 1992;10:
443-54.
9) Yen TW, Hunt KK, Ross MI, Mirza NQ, Babiera GV, mer- ic-Bernstam F, et al. Predictors of invasive breast cancer in patients with an initial diagnosis of ductal carcinoma in situ.
J Am Coll Surg 2005;200:516-26.
10) Hoorntje LE, Schipper ME, Peeters PH, Bellot F, Storm RK, Borel Rinkes IH. The finding of invasive cancer after a pre- operative diagnosis of ductal carcinoma-in-situ: causes of duc- tal carcinoma-in-situ underestimated with stereotactic 14-gauge needle biopsy. Ann Surg Oncol 2003;10:748-53.
11) Leifland K, Lagerstedt U, Svane G. Comparison of stereotactic fine needle aspiration cytology and core needle biopsy in 522 non-palpable breast lesions. Acta Radiol 2003;44:387-91.
12) Crowe JP, Rim A, Patrick RJ, Rybicki LA, Grundfest- Broniatowski SF, Kim JA, et al. Does core needle breast biop- sy accurately reflect breast pathology? Surgery 2003;134:
523-8.
13) Wahedna Y, Evans AJ, Pinder SE, Ellis IO, Blamey RW, Geraghty JG. Mammographic size of ductal carcinoma in situ does not predict the presence of an invasive focus. Eur J
Cancer 2001;37:459-62.
14) Jackman RJ, Burbank F, Parker SH, Evans WP 3rd, Lechner MC, Richardson TR, et al. Stereotactic breast biopsy of non- palpable lesions: determinants of ductal carcinoma in situ un- derestimation rates. Radiology 2001;218:497-502.
15) Hung WK, Lam HS, Lau Y, Chan CM, Yip AW. Diagnostic accuracy of vacuum-assisted biopsy device for image-detected breast lesions. ANZ J Surg 2001;71:457-60.
16) Mittendorf ME, Arciero CA, Gutchell V, Hooke J, Shriver CD. Core biopsy diagnosis of ductal carcinoma in situ: An in- dication for sentinel lymph node biopsy. Curr Surg 2005;62:
253-7.
17) Renshaw AA. Predicting invasion in the excision specimen from breast core needle biopsy specimens with only ductal carcinoma in situ. Arch Path Lab Med 2002;126:39-41.
18) Kang SS, Ko SS, Jo BH, Hur MH, Lee HK, Lee SK, et al.
Ductal carcinoma in situ (DCIS) of the breast; Clinico-patho- logical analysis, expression of molecular marker, and correla- tion between known prognostic factors. J Korean Surg Soc 2003;64:289-95.
19) Liberman L, Abramson AF, Squires FB, Glassman JR, Morris EA, Dershaw DD. The breast imagine reporting and data sys- tem: positive predictive value of mammographic features and final assessment categories. AJR Am J Roentgenol 1998;171:
35-40.
20) Schwartz GF, Patchefsky AS, Finklestein SD, Sohn SH, Prestipino A, Feig SA, et al. Nonpalpable in situ ductal carci- noma of the breast: Predictors of multicentricity and micro- invasion and implications for teatment. Arch Surg 1989;124:
29-32.
21) Fisher ER, Costantino J, Fisher B, Palekar AS, Redmond C,
Mamounas E. Pathologic findings from the National Surgical Adjuvant Breast Project (NSABP) Protocol B-17. Intraductal carcinoma (ductal carcinoma in situ). The National Surgical Adjuvant Breast and Bowel Project Collaborating Investiga- tors. Cancer 1995;75:1310-9.
22) Huo L, Sneige N, Hunt KK, Albarracin CT, Lopez A, Resetkova E. Predictors of invasion in patients with core-nee- dle biopsy-diagnosed ductal carcinoma in situ and recom- mendations for a selective approach to sentinel lymph node biopsy in ductal carcinoma in situ. Cancer 2006;107:1760-8.
23) Vicini FA, Kestin LL, Goldstein NS, Chen PY, Pettinga J, Frazier RC, et al. Impact of young age on outcome in patients with ductal carcinoma-in-situ treated with breast-conserving therapy. J Clin Oncol 2000;18:296-306.
24) Lee HD, Kim DY, Choi JW, Park BW, Jung WH, Oh KK.
Clinicopatholotical analysis of ductal carcinoma in situ and ductal carcinoma in situ with microinvasion. J Korean Surg Soc 2001;60:495-500.
25) Kang HS, Roh DY, Yoon YG, Oh SG, Choi GJ. A clin- icopatholotical analysis of microinvasive carcinoma. J Korean Surg Soc 2000;58:182-9.
26) Poller DN, Roberts EC, Bell JA, Elston CW, Blamey RW, Ellis IO. p53 protein expression in mammary ductal carcinoma in situ: relationship to immunohistochemical expression of es- trogen receptor and c-erbB-2 protein. Hum Pathol 1993;24:
463-8.
27) O'Malley FP, Vnencak JC, Dupont WD, Parl F, Manning S, Page DL. p53 mutations are confined to the comedo type duc- tal carcinoma in-situ of the breast. Immunohistochemical and sequencing data. Lab Invest 1994;71:67-72.