606
목 적 :자가 골-슬개건-골 및 생체 흡수형 간섭 나사(Bioscrew�, poly L-lactic acid, Linvatec co., USA)를 이용한 슬관절 전방 십자 인대 재건술의 결과 를 알아 보고자 하였다.
대상 및 방법 : 1998년 1월부터 12월까지 수술 받았던 39예를 대상으로 하였으며 평균 추시 기간은 2년 8개월이었다. 수술 전 KT-2000 검사, Lysholm score, IKDC score 및 Tegner score를 측정하여 최종 추시 시의 결과와 비교하였으며 2차적 관절경을 시행한 4예에서 생체 흡수형 간섭 나사의 흡수 정도 를 관찰하였다.
결 과 :수술 전 KT-2000검사는 평균 8.1±3.4 mm, Lysholm score는 66.2±16.3, IKDC score는 모든 예에서 C 이하의 소견을 보였으며 Tegner score는 3.7±0.9였다. 수술 후 KT-2000 검사는 평균 2.8±2.2 mm, Lysholm score는 91.7±7.5, IKDC score는 3예를 제외한 모든 예에서 B 이상의 결과를 보였으 며 Tegner score는 6.9±1.1였다. 2차 관절경 소견상 수술 후 3, 12개월이 경과한 예에서는 생체 흡수형 간섭 나사의 흡수 소견을 발견할 수 없었으나 수 술 후 21, 33개월에는 부분적인 흡수 소견을 관찰할 수 있었다.
결 론 :생체 흡수형 간섭 나사는 전방 십자 인대 재건술시 금속성 간섭 나사를 대체할 수 있는 고정 물질로 사료되나 흡수까지 비교적 많은 시간이 필요 한 것으로 사료되어 이에 대한 더 많은 연구가 필요하다.
색인 단어 :전방 십자 인대 재건술, 자가 골-슬개건-골, 생체 흡수형 간섭 나사
606
자가 골-슬개건-골과 생체 흡수형 간섭 나사를 이용한 관절경하 전방 십자 인대 재건술
김명구∙고석면∙김려섭∙오인석∙조규정∙이용재
인하대학교 의과대학 부속병원 정형외과학교실
606 606 통신저자 : 김 명 구
인천광역시 중구 신흥동 3가 7-206 인하대학교병원 정형외과학교실
TEL: 032-890-3662∙FAX: 032-890-3099 E-mail: [email protected]
*본 논문의 요지는 제 45차 추계 정형외과 학회에서 발표되었음.
Arthroscopic ACL Reconstruction using Bone-patellar Tendon-bone Autograft and Bioabsorbable Interference Screw
Myung Ku Kim, M.D., Suk Myun Ko, M.D., Rhuh Sub Kim, M.D., In Suk Oh, M.D., Kyu Jung Cho., M.D., and Yong Jae Lee, M.D.
Department of Orthopaedic Surgery, College of Medicine, Inha University, Inchon, Korea
Purpose :We report the results of arthroscopic ACL reconstruction using a bone-patellar tendon-bone (BPTB) autograft and a bioab- sorbable interference screw (Bioscrew�, poly L-lactic acid, Linvatec co., USA).
Materials and Methods :From January 1998 to December 1998, we performed 39 cases of arthroscopic ACL reconstruction using a BPTB autograft and a bioabsorbable interference screw. The average follow-up period was 2 years and 8 months. We performed KT- 2000 testing and measured the IKDC, Tegner and Lysholm scores preoperatively and compared these with the results of a final evalua- tion. We performed second-look arthroscopy on 4 cases and observed the degree of degradation of the bioabsorbable interference screw.
Results : Preoperative evaluation revealed an average range with a KT-2000 of 8.1±3.4 mm, a Lysholm score of 66.2±16.3, an IKDC score below C in all cases and a Tegner score of 3.7±0.9, but final results showed a KT-2000 of 2.8±2.2 mm, a Lysholm score of 91.7
±7.5, an IKDC score above B in all except 3 cases and a Tegner score of 6.9±1.1. Second-look arthroscopy at 3 and 12 months post- operatively showed no degradation of the bioabsorbable interference screw, but there was partial degradation of the bioabsorbable inteference screw at 21 and 33 months.
Conclusion :Bioabsorbable interference screws seems a reasonable alternative to metallic screws in ACL reconstruction. Bioab- sorbable screw implanted in humans may take much longer to degrade than expected, more study is needed.
Key Words : ACL reconstruction, Bone-patellar tendon-bone autograft, Bioabsorbable interference screw
Address reprint requests to Myung Ku Kim, M.D.
Department of Orthopaedic Surgery, Inha University Hospital 7-206, 3-ga Shinheung-dong, Jung-gu, Inchon 400-103, Korea Tel : +82.32-890-3662, Fax : +82.32-890-3099
E-mail: [email protected]
서 론
골-슬개건-골을 이용한 슬관절 전방 십자 인대 재건술은 전 방 십자 인대 재건술의 시금석으로 알려져 있다3,12,28,34). 자가 골-슬개건-골을 이용한 전방 십자 인대 재건술의 결과에는 많은 인자가 영향을 미치며 이들 중 수술적 기술, 이식 건의 강도 및 이식 건의 고정이 중요한 인자이다13,17,18,29). 최근 수술 후 가속 적 재활 치료가 전방 십자 인대 재건술 후 좋은 결과를 얻기 위 한 중요한 과정으로 여겨지고 있어 이식 건의 초기 고정력이 매 우 중요하다. 이식 건의 고정으로는 많은 방법이 있으나 금속성 간섭 나사가 견고한 초기 고정력으로 널리 사용되고 있고 그 예 후도 좋은 것으로 보고되고 있다2,6,14,21,30). 그러나 금속성 간섭 나사 고정은 경우에 따라 수술 중 이식 건의 파열을 초래할 수 도 있으며26) 수술 후 자기 공명 영상 촬영시 간섭 현상을 초래 하여 정확한 영상을 얻을 수 없고31) 재 재건술시 문제점을 초래 한다. 이러한 이유로 최근 생체 흡수형 간섭 나사의 이용이 증 가하고 있으며 그 결과 또한 금속성 간섭 나사와 비슷한 것으로 보고되고 있다. 생체 흡수형 나사는 그 구성 성분에 따라 신체 와의 반응이 다르며 흡수 시기도 차이가 있는 것으로 알려져 있 다. 본 연구의 목적은 생체 흡수형 간섭 나사와 자가 골-슬개 건-골을 이용하여 전방 십자 인대 재건술을 실시하고 그 결과를 분석 하였으며 2차 관절경이 필요하였던 4예의 환자에서 관절경 소견상 생체 흡수형 간섭 나사의 흡수 정도를 관찰하여 보고하 고자 하였다.
연구 대상 및 방법
1.대상1998년 1월부터 12월까지 자가 골-슬개건-골 및 생체 흡수형 간섭 나사를 이용한 관절경적 전방 십자 인대 재건술을 실시하 고 최소 2년 6개월의 추시가 가능하였던 39예를 대상으로 하였 으며 최장 추시 기간은 3년 5개월로 평균 추시 기간은 2년 8개 월이었다. 수술 당시 환자의 연령은 17세에서 58세로 평균 31세 였으며 남자가 27예, 여자가 12예였다. 손상 기전으로는 스포츠 손상이 30예로 가장 많았으며 교통 사고가 4예, 기타 낙상 등 일상 생활중의 사고에 의한 경우가 5예였다. 수상 후 수술까지 의 기간은 3개월 미만의 급성이 18예, 3개월 이상의 만성이 21 예였다. 손상 부위는 우측이 18예, 좌측이 21예였으며 동반 손 상은 내측 반월상 연골 파열이 12예, 외측 반월상 연골 파열이 10예였으며 내측 측부 인대 파열이 7예였다. 2차 관절 경을 실 시하였던 환자는 4예였으며 2예는 수술 3개월, 12개월 후 각각 진단적 관절경을 실시하였던 경우였으며, 1예는 21개월 전 타 병원에서 동종 골-슬개건-골과 생체 흡수형 간섭 나사를 이용하 여 재건술을 실시하였으나 내원 당시 전방 불안정성이 심하여
재 재건술을 실시하였던 경우였고 나머지 1예는 수술 33개월 후 외상에 의한 혈 슬관절로 재 관절경을 실시한 경우였다.
2.방법
수술 전 KT-2000 관절계를 이용하여 건측과의 전방 전위 정 도 차이를 측정하였고 IKDC score, Lysholm 및 Tegner score 등을 이용하여 기능을 평가하여 이들을 최종 추시 시의 결과와 비교 분석하였으며 통계학적 처리가 가능하였던 결과는 paired t-test를 이용하였다. 전방 십자 인대 재건술은 수상 2-3주 후 슬관절 운동이 정상으로 회복된 시점에 실시하였으나 내측 측부 인대 파열이 동반된 경우는 각도 조절기가 부착된 장하지 슬관 절 보조기를 이용하여 점진적인 운동 범위 증가를 시도하여 수 상 후 6주에 전 운동 범위가 가능하게 한 후 실시하였다. 반월 상 연골 파열은 1차 봉합술을 원칙으로 하였으나 파손의 정도가 심한 경우 및 퇴행성 변화가 심한 경우는 부분 절제술을 실시하 였다. 수술 후 재활은 가속적 재활 치료를 원칙으로 하였으며 수술 9개월 후 모든 스포츠로의 복귀를 허용하였다. 최종 추시 시 환자와의 문답을 통해 슬관절 전방 동통의 여부, 일상 생활 및 수상 전 스포츠 활동 수준으로의 복귀 정도를 조사하였다.
2차 관절경을 실시하여 생체 흡수형 간섭 나사의 흡수 정도를 관찰하였다.
결 과
수술 전 KT-2000 관절계를 이용한 건측과의 최대 도수 전방 전위 차이는 최소 3 mm, 최대 14.5 mm로 평균 8.1±3.4 mm 이었으며, Lysholm score는 35에서 89로 평균 66.2±16.3,
Preop. evaluation (No. of patients)
Final evaluation (No. of patients)
Score Grade
Lysholm Excellent 0 20
Good 3 14
Fair 25 5
Poor 11 0
IKDC A 0 17
B 0 19
C 21 3
D 18 0
Table 1.Results of Lysholm and IKDC score
Final evaluation Score Preop. evaluation
Lysholm 66.2±16.3 91.7±7.5
Tegner 3.7±0.9 6.9±1.1
KT-2000 8.1±3.4 2.8±2.2
Table 2.Results of functional evaluation scale
Tegner score는 모든 예에서 5 이하의 소견을 나타냈으며 평균 3.7±0.9였고 IKDC score는 C가 21예, D가 18예로 모든 예에 서 C 이하의 소견을 보였다. 최종 추시 시 KT-2000 검사상 건 측과의 최대 도수 전방 전위 차는 3 mm 이하가 31예, 3-5 mm가 5예, 5-10 mm가 3예로 평균 2.8±2.2 mm를 보여 수술 전의 전위 차와 유의한 소견을 보였다(p<0.005). Lysholm score는 우수가 20예, 양호가 14예, 보통이 5예로 34예(87%)에 서 양호 이상의 결과를 보였으며 평균 91.7±7.5의 결과를 보여 수술 전에 비해 호전된 소견을 보였다(p<0.005). Tegner score 는 수술 후 6.9±1.1로 증가하였으며 IKDC score는 정상이 17 예, 유사 정상이 19예, 비정상이 3예로 36예(92%)에서 유사 정 상 이상의 결과를 보였다(Table 1, 2). 일상 생활로의 복귀 수 준은 32예(82%)에서 90% 이상의 복귀를 보였으며 이 중 26예 (67%)에서는 100%의 복귀를 보였고, 수상 전 스포츠 활동으
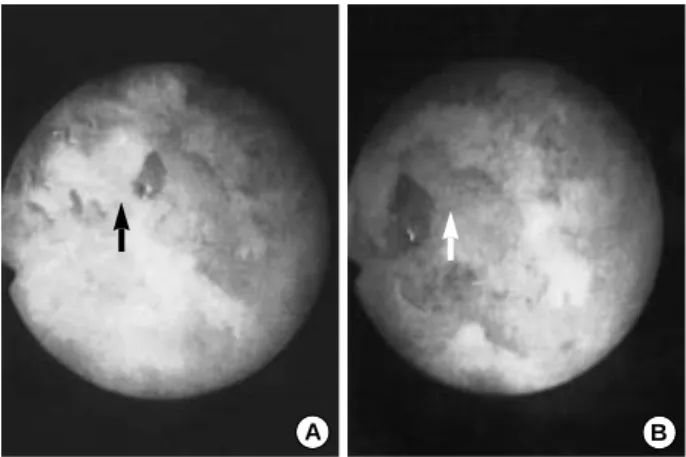
로의 복귀 수준은 90% 이상이 25예(64%)였으며 이 중 11예 (29%)는 100%의 복귀를 보였다. 최종 추시 시 슬부 전방 동통 을 호소한 예는 10예(25%)였으나 동통의 정도는 경미하여 일 상 생활에는 지장을 주지 않는 경우였다. 수술 후 슬관절의 신 전 장애 소견이 있었던 1예를 제외한 모든 예에서 특별한 합병 증은 없었다. 재 관절경술을 실시하였던 경우는 4예로 관절경 소견상 수술 후 3개월 및 12개월의 환자에서는 생체 흡수형 간 섭 나사의 흡수 소견을 발견할 수 없었다(Fig. 1). 수술 후 21 개월의 환자에서는 간섭 나사가 일부 흡수와 파괴된 양상을 관 찰할 수 있었고 흡수된 부위에 섬유성 조직이 발견되었으며 섬 유 조직 제거 후 공동(cavity)이 형성 되어있는 소견을 관찰할 수 있었으나 골 내부 성장의 소견은 관찰할 수 없었다(Fig. 2).
수술 후 33개월의 환자에서는 생체 흡수형 간섭 나사가 일부 파 괴된 소견을 관찰할 수 있었다(Fig. 3).
고 찰
슬관절 손상 중 빈번이 발생하는 전방 십자 인대 파열은 재건 술로 좋은 결과를 얻을 수 있다. 성공적인 전방 십자 인대 재건 술를 위해서는 많은 요소들이 고려되어야 하며 이들 중 이식 건 의 강도와 이식 건의 고정 및 수술 후 재활이 중요한 요소이다.
자가 골-슬개건-골과 금속성 간섭 나사를 이용한 재건술은 이식 슬개건의 좋은 생역학적 특성과 견고한 고정력으로 좋은 결과를 얻을 수 있어 현재 널리 사용되고 있다. 그러나 금속성 간섭 나 사는 삽입시 이식 건에 손상을 초래할 수 있고5,26) 간섭 나사에 의해 이식 골 한쪽 면의 골유합이 영구히 방해를 받으며 추시 과정 중 자기 공명 영상 촬영시 금속에 의한 간섭 현상으로 정 확한 영상을 얻을 수 없다22,23,31). 또한 이식 건의 재 파열로 인 Fig. 1.A: Arthroscopic finding of the head of a bioabsorbable
interference screw 3 months after operation. The bioabsorbable screw is still intact without any evidence of degradation. B: The photograph of a bioabsorbable interference screw removed from a patient 12 months after operation because of loosening. There is no evidence of degradation.
A B
Fig. 2.Arthroscopic finding of the head of a bioabsorbable inter- ference screw 21 months after operation. A: There is fibrous tis- sue (black arrow) at the previous screw insertion site. B: After removal of the fibrous tissue, the cavity (white arrow) shows an imprint of the head of the bioabsorbable interference screw, implanted previously, but no bony ingrowth.
A B
Fig. 3.Arthroscopic finding of the head of a bioabsorbable inter- ference screw 33 months after operation. Grossly the head of the screw (white arrow) appears to be fragmented.
한 재 재건술 및 슬관절 치환술시 나사를 제거해야 한다는 단점 이 있다. 생체 흡수형 고정물이 개발되면서 전방 십자 인대 재 건술에도 금속성 간섭 나사의 단점을 극복할 수 있는 생체 흡수 형 간섭 나사가 사용되고 있다7,32). 생체 흡수형 고정물은 여러 가지 재료로 만들어지고 있으나 전방 십자 인대 재건술시 이식 건의 고정에는 비교적 염증 반응 등의 부작용이 적은 poly L- lactic acid (PLLA)로 구성된 간섭 나사가 널리 사용되고 있
다7,32). 생체 흡수형 간섭 나사의 고정력에 대해서는 약간의 이
견이 있으며 Mark22)는 생체 흡수형 간섭 나사가 금속성 간섭 나사의 초기 고정력에 비해 낮은 수치로 측정 되었으나 통계학 적 유의한 차이는 없었다고 보고하였으며 고정 후 약 4주까지는 고정 강도가 초기에 비해 감소하나 이후 초기의 고정 강도로 복 귀되어 12주까지 강도가 증가한다고 보고하였다. 일반적으로 생 체 흡수형 간섭 나사의 고정 강도는 금속성 간섭 나사와 유의한 차이가 없어 금속성 간섭 나사와 같이 수술 후 급진적 재활 치 료가 가능한 것으로 알려져 있다1,19,20,33). 생체 흡수형 간섭 나사 의 흡수 시기는 아직도 이견이 있으며9,11,25) Georg 등16)은 자기 공명 영상 사진상 수술 후 6개월에서 간섭 나사의 음영이 사라 졌다고 발표하였으나 최근의 발표에 의하면 예상 기간 보다는 더 많은 시간이 필요하며 길게는 6년 정도가 걸리는 것으로 보 고되고 있다9,24). 그러나 Andreas 등4)은 생체 흡수형 간섭 나사 가 삽입 부위에서 완전히 흡수된 후에도 그 조각들이 주위의 연 부 조직에서 발견되고 있으며 경우에 따라서는 주위의 임파절에 서도 발견되고 있어 이러한 조각들이 완전히 흡수 되기 전에는 흡수 여부를 단호하게 판단하는 것에 문제가 있다고 경고하였 다. 생체 흡수형 간섭 나사의 합병증으로는 삽입 중 간섭 나사 의 파단이 보고 되고 있어27) 수술시 notcher, dilator, tap 및 삽 입 유도 강선을 이용하여 고정력에 영향을 미치지 않고 삽입이 용이하도록 하여 수술 중 발생할 수 있는 합병증에 대한 세심한 주의가 요구된다. 수술 후 합병증으로는 고정물의 무균성 염증 반응이 약 1.5%에서 보고 되고 있으며10) 그 정도는 미약한 염 증 반응에서 수술적 변연 절제술을 요할 정도의 심각한 염증까 지 다양하게 보고 되고 있다8,15). 생체 흡수형 간섭 나사를 이용 한 전방 십자 인대 재건술의 최종 결과는 금속성 간섭 나사를 이용한 재건술에 비해 유의한 차이가 없으며 금속성 간섭 나사 에 비해 삽입시 연부 조직의 손상을 줄일 수 있으며 수술 후 추 시 과정 중 자기 공명 영상 사진상 간섭 현상이 없어 정확한 영 상을 얻을 수 있고 재 재건술시 간섭 나사의 제거가 필요 없다 는 장점이 있다22,23,27). 저자들 경우도 80% 이상의 환자에서 모 든 분야의 결과가 양호 이상의 소견을 보였으며 환자의 주관적 인 평가도 약간의 차이는 있으나 만족 할 만한 평가를 받아 이 미 보고된 금속성 간섭 나사를 이용한 재건술의 결과와 유사한 결과를 보였으며5,14,23) 수술 중 및 수술 후 나사 파단 등의 특이 한 합병증은 없었다. 생체 흡수형 간섭 나사가 흡수된 후 흡수 부위가 골로 대치되는지의 여부는 아직 확실한 보고는 없으며 Andreas 등4)은 수술 20개월 후 재 관절경상 생체 흡수형 간섭
나사가 일부 흡수된 부위에 섬유성 조직이 발견되었으나 골 내 부 성장의 소견은 발견할 수 없었다고 보고하였다. 저자들의 경 우도 수술 후 21개월이 경과한 환자의 재 관절경 소견상 생체 흡수형 간섭 나사가 흡수된 부위에 골 조직이 아닌 섬유성 조직 을 관찰할 수 있었으며 수술 33개월이 경과한 환자에서는 흡수 되지 않은 파괴된 생체 흡수형 간섭 나사를 관찰할 수 있어 생 체 흡수형 간섭 나사의 흡수 시기가 Bergsma 등9)의 보고와 같 이 초기 예측 보다는 많은 시간이 소요될 것이라는 의견을 뒷받 침할 수 있었다.
결 론
생체 흡수형 간섭 나사는 전방 십자 인대 재건술시 그 장점으 로 금속성 간섭 나사를 대체할 좋은 방법으로 생각되며 수술 후 부작용도 매우 적은 것으로 사료된다. 그러나 생체 흡수형 간섭 나사의 흡수 과정에서 발생할 수 있는 생체 흡수형 간섭 나사의 파편이 중, 장기적으로 인체에 어떠한 영향을 미치는 지와 생체 흡수형 간섭 나사의 정확한 흡수 시기 및 흡수 후 골로의 완벽 한 대체 여부 등에 관한 연구가 이루어져야 할 것으로 판단된다.
참고문헌
1. Abate JA, Fadale PD, Hulstyn MJ and Walsh WR: Initial fixation strength of polylactic acid interference screws in anterior cruciate ligament reconstruction. Arthroscopy, 14: 278-284, 1998.
2. Aglietti P, Buzzi R, D’’Andria S and Zaccherotti G:Long-term study of the anterior cruciate ligament reconstruction for chronic instability using the central one-third patellar tendon and a lateral extraarticular tenodesis.
Am J Sports Med, 20: 38-45, 1992.
3. Alm A and Gillquist J: Reconstruction of the anterior cruciate ligament by using the middle third of the patellar ligament. Acta Chir Scand, 140:
289-296, 1974.
4. Andreas CS, Andreas W, Hansjorg R, Reinhard H, Alfred G and Richard F:Clinical degradation and biocompatibiliy of different bioab- sorbable interference screws: A report of six cases. Arthroscopy, 13: 238- 244, 1997.
5. Bach BR Jr: Potential pitfalls of Kurosaka interference screw fixation for ACL surgery. Am J Knee Surg, 2: 76-82, 1989.
6. Bach BR, Jones GT, Sweet FA and Hager CA: Arthroscopy assisted anterior cruciate ligament reconstruction using patellar tendon substitution.
Two to four years follow up results. Am J Sports Med, 22: 758-767, 1994.
7. Barber FA, Elrod BF, McGuire DA and Paulos LE: Preliminary results of an absorbable interference screw. Arthroscopy, 11: 537-538, 1995.
8. Barfod G and Svendsen RN: Synovitis of the knee after intraarticular
fracture fixation with Biofix. Report of two cases. Acta Orthop Scand, 63:
680-681, 1992.
9. Bergsma JE, de Bruijn WC, Roxema FR, Bos RR and Boering G:
Late degradation tissue response to poly bone plates and screws. Biomate- rials, 16: 25-31, 1995.
10. Bostman OM: Current Concepts Review: Absorbable implants for the fixation of the fracture. J Bone Joint Surg, 73-A: 148-153, 1991.
11. Bostman OM and Pihlajamaki HK: Late foreign-body reaction to an intraosseous bioabsorbable polylactic acid screw. J Bone Joint Surg, 80-A:
1791-1794, 1998.
12. Burks RT: Practical considerations on cruciate graft fixation. Oper Tech Orthop, 2: 71-75, 1992.
13. Burks RT, Daniel D and Losse G: The effect of continuous passive motion on anterior cruciate ligament reconstruction stability. Am J Sports Med, 21: 880-886, 1984.
14. Buss DD, Warren RF, Wickiewicz TL, Galinat BJ and Panariello R: Arthroscopically assisted reconstruction of the anterior cruciate liga- ment with use of autogenous patellar-tendon grafts: Results after twenty- four to forty-eight month. J Bone Joint Surg, 75-A: 1346-1355, 1993.
15. Friden T and Rydholm U: Severe aseptic synovitis of the knee after biodegradable internal fixation. Acta Orthop Scand, 63: 94-97, 1992.
16. Georg L, Klaus H, Gernot A, Franz U, Irene N and Ernst O: Serial magnetic resonance imaging evaluation of a bioabsorbable interference screw and the adjacent bone. Arthroscopy, 15: 481-488, 1999.
17. Grood ES, Suntal WJ, Noyes FR and Butler DL: Biomechanics of the knee extension exercise. J Bone Joint Surg, 66-A: 725-734, 1984.
18. Harner CD, Irrgang JJ, Paul J, Dear-water S and Fu FH: Loss of motion following anterior cruciate reconstruction. Am J Sports Med, 20:
507-515, 1992.
19. Johnson LL and vanDyk GE: Metal and biodegradable interference screws: Comparison of failure strength. Arthroscopy, 12: 452-461, 1996.
20. Kousa P, Jarvinen TL, Pohjonen T, Kannus P, Kotikoski M and Jarvinen M:Fixation strength of a biodegradable screw in anterior cruci- ate ligament reconstruction. J Bone Joint Surg, 77-B: 901-905, 1995.
21. Mader RA, Raskind JR and Carroll M: Prospective evaluation of arthroscopically assisted anterior cruciate ligament reconstruction. Patel- lar tendon versus semitendinosus and gracilis tendons. Am J Sports Med, 19: 479-448, 1991.
22. Mark W: Absorbable and metal interference screws: Comparison of graft
security during healing. Arthroscopy, 15: 818-826, 1999.
23. Marti C, Imhoff AB, Bahrs C and Romero J: Metallic versus bioab- sorbable interference screw for fixation of bone-patellar tendon-bone auto- graft in arthroscopic anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc, 5: 217-221, 1997.
24. Martinek V, Seil R, Lattermann C, Watkins SC and Fu FH: The Fate of the poly-L-lactic acid interference screw after anterior cruciate ligament reconstruction. Arthroscopy, 17: 73-76, 2001.
25. Matsusue Y, Hanafusa S, Yamamuro T, Shikinami Y and Ikada Y : Tissue reaction of bioabsorbable ultra high strength poly rod. Clin Orthop, 317: 246-253, 1995.
26. Matthews LS and Soffer SR: Pitfalls in the use of interference screws for anterior cruciate ligament reconstruction: Brief report. Arthroscopy, 5:
225-226, 1989.
27. McGuire DA, Barber FA, Elrod BF and Paulos LE: Bioabsorbable interference screws for graft fixation in anterior cruciate ligament recon- struction. Arthroscopy, 15: 463-473, 1999.
28. Noyes FR, Butler DL, Grood ES, Zernicke RF and Hefzy MS:
Biomechanical analysis of human ligament grafts used in knee-ligament repairs and reconstructions. J Bone Joint Surg, 66-A: 344-352, 1984.
29. Noyes FR, Mangine RE and Barber S: Early knee motion after open and arthroscopic anterior cruciate ligament reconstruction. Am J Sports Med, 15: 149-160, 1987.
30. O’’Brien SJ, Warren FR, Pavlov H, Panariello R and Wickiewicz TL:Reconstruction of the chronically insufficient anterior cruciate liga- ment with the central third of the patellar ligament. J Bone Joint Surg, 73- A: 273-286, 1991.
31. Shellock FG, Mink JH, Curtin S and Friedmann MJ: MR imaging and metallic implants for anterior cruciate ligament reconstruction: assess- ment of ferromagnetism and artifact. J Magn Reson Imag, 2: 225-228, 1992.
32. Stahelin AC, Feinstein R and Friederich NF: Clinical experience using a bioabsorbable interference screw for ACL reconstruction. Orthop Trans, 19: 287-288, 1995.
33. Stefan R, Paul WK and Ekkehard WF: Fixation strength of a biodegrad- able interference screw and a press-fit technique in anterior cruciate liga- ment reconstruction with a BPTB graft. Arthroscopy, 13: 61-65, 1997.
34. Wachtl S, Imhoff A, Treibel W and Rodriguez M: Retrospective com- parison of four intraarticular anterior cruciate ligament reconstructions using 3 scoring methods. Arch Orthop Trauma Surg, 114: 25-31, 1994.