340
서 론
소아의 대퇴골 골절은 견인술, 고수상 석고 고정 등의 보존적인 치료에서 유연성 골수정, 금속판 내고정술, 외 고정 장치, 교합성 골수정 등의 수술적 치료까지 다양한 방법이 이용되고 있다2,6,7,24). 치료 방법의 선택은 환자의 나이, 골절의 위치와 형태 등에 따라 다르나, 최근 학동기 의 소아에서는 환아의 빠른 학교로의 복귀나 가족의 사회 적 복귀를 위해 수술적 치료의 이용이 증가되고 있는 추
세이다8,11). 하지만, 소아 대퇴골 골절의 수술적 빠른 골
의 치유와 함께, 운동 및 보행을 허용하고, 또한 합병증이 작은 내고정물이 우선되어야 한다6). 외고정 장치를 이용 한 치료는 핀 감염, 슬관절 강직, 그리고 제거 후 발생하 는 재 골절 등의 합병증을 흔히 동반하며23), 유연성 골수 정은 분쇄가 있거나 체중이 많은 환자에서 부정정렬의 빈 도가 많은 것으로 알려져 있다16).
본 연구는 소아 대퇴골 골절에서 최소 침습적 금속판
소아 대퇴골 골절에 대한 최소 침습적 금속판 고정술
박병철․오창욱․경희수․전인호․민우기․조창현
경북대학교 의과대학 정형외과학교실
Minimally Invasive Percutaneous Plating of Pediatric Femoral Fractures
Byung-Chul Park, M.D., Chang-Wug Oh, M.D., Hee-Soo Kyung, M.D., In-Ho Jeon, M.D., Woo-Kie Min, M.D., and Chang-Hyun Cho, M.D.
Department of Orthopedic Surgery, College of Medicine, Kyungpook National University, Daegu, Korea P u rp o s e : To determine the efficacy of percutaneous plating for pediatric femoral fractures.
M a te ria ls a n d M e th o d s : Fourteen children (mean age, 9.1 years-old) with a femoral fracture were treated with m inim ally invasive percutaneous plating. After a tem porary reduction by m anual traction or flexible nailing, a plate w as inserted into the subm uscular plane through proxim al or distal incisions of 2-3 cm . Screw s w ere then fixed with the control of the fracture alignm ent under fluoroscopic guidance. All procedures were carried out w ithout opening the fracture site. The loca- tions of the fracture are as follow s: 10 in the m iddle, 2 in the subtrochanteric, 1 in the proxim al, and 1 in the distal area. Seven had a com m inution in the fracture, and nine had associated injuries or fractures. According to Flynns criteria, the patients w ere evaluated after a m inim um of 1 year (m ean, 2.1 years).
R e s u lts : All the fractures united without the need for a bone graft. The mean radiographic healing tim e was 11.1 w eeks (range, 1014 w eeks). No residual radiographic frontal or sagittal plane angu- lation >10 or a leg length discrepancy >5 m m was observed in any patient. No patient showed any lim itation in the joint, lim ping, or im plant related problem s. All the patients show ed excellent final results.
C o n c lu s io n : Minimally invasive percutaneous plating is a safe and acceptable surgical option for the treatm ent of pediatric fem oral fractures.
K e y W o rd s : Pediatric femoral fractures, Minimally invasive percutaneous plating
통신저자:오 창 욱
대구광역시 중구 삼덕 2가 50 경북대학교병원 정형외과
TEL: 053-420-5630․FAX: 053-422-6605 E-mail: [email protected]
Address reprint requests to Chang-Wug Oh, M.D.
Department of Orthopedic Surgery, Kyungpook National University Hospital 50, 2 ga, Samdeok-dong, Jung-gu, Daegu 700-721, Korea
Tel: +82.53-420-5630, Fax: +82.53-422-6605 E-mail: [email protected]
고정술을 전향적으로 시행하고 그 결과와 효용성을 알아 보고자 하였다.
대상 및 방법
2000년 1월부터 2004년 6월까지 본원에서 치료한 87 명의 5세 이상-15세 미만의 대퇴골 골절 환자 중에서 최 소 침습적 금속판 고정술을 시행한 경우는 19명이었으 며, 그 중 병적 골절 또는 기존 질환의 합병증에 따른 골 절을 제외한 14명을 연구 대상에 포함하였다. 환자의 나 이는 5-14세로 평균 9세였으며, 남자가 11명, 여자가 3 명이었다.
수술적 적응증은 학동기의 대퇴골 간부 또는 전자하부 골절을 기본 대상으로 하였으며, 골절부위 또는 그 양상 이 유연성 골수정(flexible intramedullary nail)으로 고 정이 힘든 경우, 10세 이상의 환자, 다발성 골절, 또한 뇌 손상 등으로 제어되지 않는 강직 등이 있을 때를 적극 적인 대상으로 하였다. 사용된 금속판은 LCP (locking compression plate-large fragment, SynthesⓇ, Uni- ted States), LC-DCP (limited contact dynamic compression plate, SynthesⓇ, United States), DCS (dynamic condylar screw, SynthesⓇ, United States) 등이었다.
1. 수술 방법
환아는 마취 후에 투시가 가능한 수술대에 앙와위로 눕힌 다음 도수 견인 또는 유연성 골수정을 이용하여 임 시 정복을 실시하였다. 유연성 골수정은 Oh 등18)의 방법 과 같이 원위 대퇴부의 성장판 상방에서 1개 또는 2개의 골수정(2.5 mm 또는 3.0 mm)을 내측 또는 외측에서 삽 입하여 골절부를 임시 정복을 하였다. 정복이 어렵거나 정복 후에도 각형성 등이 남은 경우 외고정 시 사용되는 1-2개의 하프핀 골절 원근위부에 삽입하여 조절하였다.
적절한 길이의 선택된 금속판은 가능한 원위 또는 근위 대퇴골의 외측부에 맞게 굽히고, 원위 또는 근위부의 약 2-3 cm의 피부 절개 후 만든 근육 하면(submuscular plane)으로 삽입하였다. 형광 투시경의 감시하에 금속판 과 대퇴골의 정렬을 조절하였고, 최소 3개씩 이상의 나사 못을 각각의 골편에 경피적으로 고정하였다(Fig. 1).
술 후 부목 또는 보조구의 착용을 하지 않았으며, 슬관 절 및 고관절의 능동적 관절 운동을 허용하였다. 부분 체 중부하는 약 4주 경부터 목발 사용 하에 허용하였고, 전 체중 부하는 골진이 충분히 성숙된 후에 허용하였다.
추시 방사선 촬영은 술 후 최소 4주 간격으로 하였으 며, 골의 유합은 골절부위를 잇는 가골의 형성이 된 시점 을 기준으로 하였고, 각 변형을 포함한 전후 및 측면 정렬 에 대하여 측정을 하였으며, 최종 추시에서는 건측의 대 퇴골과 함께 계측을 하여 하지 부동을 확인하였으며, 최
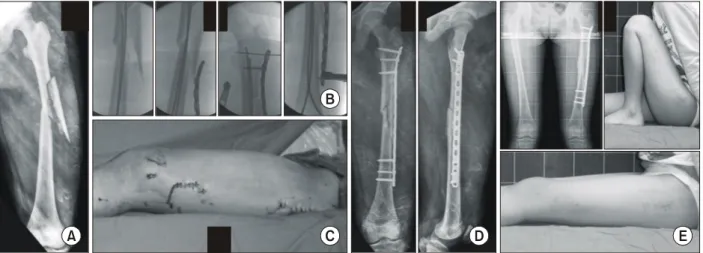
Fig. 1. An 11-year-old girl had a comminuted fracture of femoral shaft (A). After the temporary reduction with flexible nailing, percutaneous plating with a LCP (locking compression plate) was made under fluoroscopy (B). Postoperative photo shows the distal incisions used for temporary nail insertion and plate placement and the proximal incision used for screw placement (C). Fixation and alignment were satisfactory on the postoperative radiograph (D). After 1 year of follow-up, she had a minimal leg length discrepancy with an excellent function of hip and knee (E).
A
B
C D E
종 추시시의 관절 운동제한 등의 합병증을 조사하였다.
최종결과의 판정은 동통, 하지 부동, 부정정렬, 그리고 합병증에 따른 Flynn 등의 방법6)으로 우수, 만족, 불량 으로 구분하였다.
결 과
외상 후 수술 시까지의 평균 기간은 2일(범위, 0-9일) 이었으며, 평균 수술 시간은 65분(범위, 52-80분)이었
다. 동반된 손상을 가진 환자는 9명으로 뇌 손상(뇌 좌상, 경막하 출혈)이 6예, 다발성 골절 2예, 복부 손상(간 열 상)이 2예, 폐 손상(외상성 혈흉 및 기흉) 2예 등이 포함 되었다. 골절부의 분쇄는 7예에서 동반하였으며, 골절의 부위는 중위부가 10예로 가장 많았고, 전자하부 2예(Fig.
2), 근위부 1예, 원위부 1예 등이었다(Table 1).
최소 1년 이상(평균 2.1년)의 추시를 시행한 후, 14명 환자 모두에서 골 이식 등의 추가적인 술식 없이 골 유합
Table 1. Case Data for the Percutaneous Plating of Pediatric Femoral Fractures
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Age Location of Fracture Kinds of Postoperative Final Union period LLD
No Sex Associated injury
(years) fracture comminution implant angulation (o) angulation (o) (weeks) (mm) ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
1 Male 10 Middle Positive Epidural hemorrahge LCP 1/10 0/3 10 0
2 Male 13 Subtrochanteric Positive - DCS 3/6 0/3 12 1
3 Male 8 Middle - Cerebral contusion LCP 0/7 0/2 10 2
4 Male 6 Proximal - Liver laceration LCP 7/15 0/4 10 2
5 Male 13 Middle - - LCP 8/4 2/1 10 -2
6 Male 7 Distal Positive SAH LCP 1/3 0/1 10 0
7 Male 6 Middle - Cerebral contusion LCP 4/6 1/1 11 4
Liver laceration, hip
8 Female 11 Middle Positive LCP 2/3 1/2 14 -1
Dislocation, pneumothorax Hemothorax, Clavicle fx,
9 Male 8 Subtrochanteric Positive LCP 4/2 0/0 10 0
Humerus fx
10 Male 9 Middle - - LCP 6/5 0/1 10 1
11 Male 9 Middle - - LCP 6/10 0/4 12 3
12 Female 8 Middle Positive - LCP 4/5 0/0 12 1
13 Female 9 Middle - Cerebral contusion LC-DCP 2/0 0/0 12 1
14 Female 10 Middle Positive Cerebral contusion LCP 3/5 0/0 12 0
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ
Mean 9.1 3.6/5.8 0.3/1.6 11.1 0.9
ꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏꠏ Angulation, the frontal and sagittal angle are described in order; Types of implant: LCP, locking compression plate; DCS, dynamic condylar screw; LC-DCP, limited contact-dynamic compression plate; Fx, fracture; LLD, leg length discrepancy
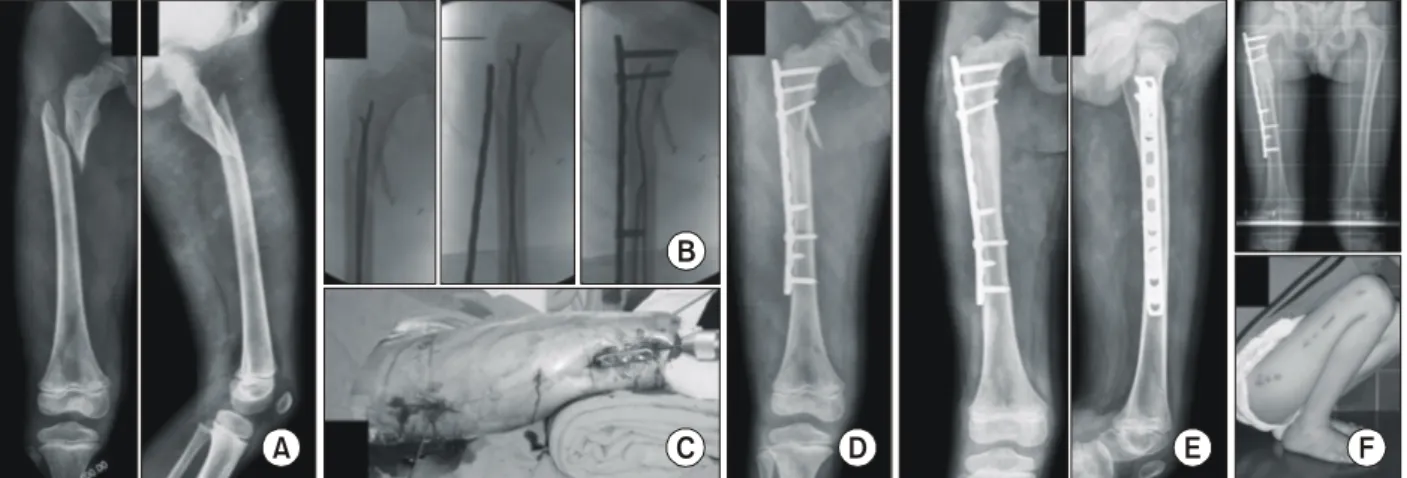
Fig. 2. An 8-year-old boy with a subtrochanteric femoral fracture (A) was treated with percutaneous plating after temporary flexible nailing (B, C). After operation, a good alignment was achieved (D). The fracture was healed 10 weeks after surgery (E). The knee function was excellent without a leg length discrepancy at 2 years after surgery (F).
A
B
C D E F
을 얻었으며, 평균 골 유합 기간은 11.1주(범위, 10-14 주)였다.
수술 직후 전면 각형성은 3.6도(범위, 0-8도), 측면 각 형성은 5.8도(범위, 0-15도)였으며 최종 추시상의 전면 각형성은 0.3도(범위, 0-2도), 측면 각형성은 1.6도(범 위, 0-4도)로, 5도 이상의 각 형성을 보인 환자는 없었 다. 최종 추시상 5도 이상의 회전 변형을 보인 환자는 없 었으며, 평균 하지 부동은 약 0.9 mm의 환측의 과성장 (범위, 단축 2 mm-과성장 4 mm)을 보였으며, 5 mm 이상의 하지 부동을 보인 예는 없었다. 금속판 또는 나사 못의 파손 등이 일어난 경우는 없었으며, 금속판의 제거 는 9명에서 이루어졌으며 그 시기는 평균 8, 9개월(범위, 5-13개월)이었으며, 재골절의 발생은 없었다.
동통, 파행, 관절 운동의 제한, 심부 감염 등을 보인 환자는 없었으며, 최종 추시상의 임상적 결과는 모든 환 자에서 우수의 결과를 보였다.
고 찰
소아 대퇴골 골절의 치료에 많은 방법이 적용되고 있는 데, 전통적인 견인 후 석고고정 방법은 나이가 어리거나 단독 골절의 환자에서 적용될 수 있으나15,22,26), 반복되는 골절부의 조작이 필요하고, 환자의 움직임을 장기간 제한 하며, 간호의 어려움이 따르므로 본 연구의 많은 환자에 서처럼 다발성 골절 환자 또는 타 장기의 손상을 입은 환 자에서는 그 적응증의 제한이 따른다10,12,20).
이러한 이유와 환자 및 가족의 빠른 사회적 복귀를 돕 기 위하여 소아 대퇴골 골절에 대하여 수술적 치료가 최 근 많이 선호되고 있는데, 유연성 골수정은 골절부의 추 가적인 손상은 주지 않으면서, 빠른 골의 치유 및 재형성 을 유도하며, 성장 판이나 대퇴 골두에 영향을 주지 않는 장점이 있다6,9,13,18). 본 연구의 방법인 최소 침습적 금속 판 고정술도 골절부의 혈류를 보존하므로 유연성 골수정 의 장점을 공유하면서도 교합성 골수정에 버금가는 충분 한 고정력을 가지는 좋은 방법으로 소개되고 있다. 하지 만, 유연성 골수정은 골절의 분쇄가 있는 경우6,16) 정복의 소실과 함께 부정 정복이 일어날 가능성이 많고, 적절치 못한 굵기의 골수정을 선택할 때 부정정렬의 가능성이 많 은 것이 단점인데, 본 연구에서 최초 정복이 소실된 경우 는 없었으며, 또한 많은 수의 환자에서 골절분쇄가 동반 되었으나 부정정렬을 남긴 예는 없어 이는 최소 침습적
금속판 고정술의 장점으로 생각된다. 유연성 골수정은 강 성도의 한계로 인하여 뇌 손상 등으로 심한 강직이 있을 경우나 체중이 많은 경우14,25) 정복의 유지가 힘들뿐 아니 라 골수정이 휘는 현상이 일어날 수 있으므로 석고 부목 이 필요한 것이 현실이다18). 교합성 골수정을 사용하면 위의 합병증을 줄일 수 있겠으나, 대퇴 골두로의 혈류 차 단에 따른 무혈성 괴사가 발생할 수 있고, 또한 대퇴 대 전자부의 조기 골단판 유합에 따른 외반고(coax valga) 와 하지 단축의 위험성이 따르게 된다3,21). 이에 반하여 저자들의 방법은 비교적 강한 고정력을 가진 금속판을 사 용함에 따라 추가적인 조치 없이도 안전하게 환자의 기동 을 조기 허용할 수 있으며, 또한 교합성 골수정의 사용에 따른 합병증을 줄일 수 있는 방법으로 생각된다.
내고정물과 관련된 합병증은 소아 대퇴골의 치료선택 에 또 다른 중요한 기준이 되는데, 외고정 장치는 핀 감염 과 슬관절의 강직은 물론 제거술 후에 재골절의 발생은 외고정 장치의 사용을 제한하게 하는 큰 단점으로 알려져 있다. 전통적인 관혈적 정복 및 금속판 내고정 시에도 유 합 후 금속판을 제거할 경우 재골절의 가능성은 있으나, 최소 침습적 금속판 고정술에 의한 골절부의 가골이 간접 적 골 치유는 직접적 골치유보다 강도가 좋으므로 재골절 의 가능성이 본 연구에서처럼 매우 낮다고 알려져 있다19). 유연성 골수정의 시술 후 가장 많은 환자의 불편감은 슬 관절부에 남아 있는 골수정의 돌출로 인한 통증 또는 자 극증이며, 또한 골수정의 이동에 따른 합병증도 드물지 않는데13), 슬관절 주위의 자극증이나 강직 등은 본 연구 에서는 나타나지 않아, 좋은 치료 방법 중의 하나로 생각 한다.
최소 침습적 금속판 고정술은 성인의 골절 중 골수정이 적용되기 힘든 장관골의 골 간단부의 골절이나 분쇄 골절 에 이용되고 있는데17,19), 소아 대퇴골의 골절의 치료보고 는 많지 않다1). 고식적인 내고정 방법인 관혈적 정복은 불유합의 가능성이 많을 뿐 아니라 골수염 및 심부 감염 의 가능성이 높은데4,5), 이는 특히 두부 손상 환자27)들에 서 시행할 경우 그 위험성이 높다. 하지만, 본 연구에서는 많은 수의 두부 손상 환자가 포함됨에도 불구하고 감염증 이 없었던 것은 최소 침습적 방법의 큰 장점으로 생각된 다. 골절부를 개방치 않고 시술함에 따르는 골절부의 정 렬에 어려움은 이 방법의 기술적 단점인데, 저자들은 1-2개의 유연성 골수정을 미리 삽입하여 대강의 임시정
복을 한 다음 금속판을 고정하여 보다 쉽고 빠르게 시술 할 수 있었다.
본 연구의 단점은 개체의 수가 작으며, 비교적 짧은 추 시 등으로 인해 장기적인 관점에서 정확한 하지부동 및 임상결과를 알지 못하는 것이므로 이는 추가적인 연구가 필요할 것이다.
결 론
최소 침습적 금속판 고정술은 다발성 손상, 뇌손상 또 는 분쇄를 동반한 소아 대퇴골 골절의 치료에서 우수한 결과를 가져올 수 있는 좋은 치료 선택이 될 수 있을 것으 로 생각된다.
참고문헌
1. Agus H, Kalenderer O, Eryanilmaz G, Omeroglu H:
Biological internal fixation of comminuted femur shaft fractures by bridge plating in children. J Pediatr Orthop, 23: 184-189, 2003.
2. Aronson J, Tursky EA: External fixation of femur fractures in children. J Pediatr Orthop, 12: 157-163, 1992.
3. Beaty JH, Austin SM, Warner WC, Canale ST, Nichols L: Interlocking intramedullary nailing of femoral-shaft fractures in adolescents: preliminary results and complications. J Pediatr Orthop, 14: 178-183, 1994.
4. Caird MS, Mueller KA, Puryear A, Farley FA: Compres- sion plating of pediatric femoral shaft fractures. J Pediatr Orthop, 23: 448-452, 2003.
5. Eren OT, Kucukkaya M, Kockesen C, Kabukcuoglu Y, Kuzgun U: Open reduction and plate fixation of femoral shaft fractures in children aged 4 to 10. J Pediatr Orthop, 23: 190- 193, 2003.
6. Flynn JM, Hresko T, Reynolds RA, Blasier RD, Davidson R, Kasser J: Titanium elastic nails for pediatric femur fractures: a multicenter study of early results with analysis of complications. J Pediatr Orthop, 21: 4-8, 2001.
7. Galpin RD, Willis RB, Sabano N: Intramedullary nailing of pediatric femoral fractures. J Pediatr Orthop, 14: 184-189, 1994.
8. Greisberg J, Bliss MJ, Eberson CP, Solga P, d'Amato C:
Social and economic benefits of flexible intramedullary nails in
the treatment of pediatric femoral shaft fractures. Orthopedics, 25: 1067-1070, 2002.
9. Heinrich SD, Drvaric DM, Darr K, MacEwen GD: The operative stabilization of pediatric diaphyseal femur fractures with flexible intramedullary nails: a prospective analysis. J Pediatr Orthop, 14: 501-507, 1994.
10. Herndon WA, Mahnken RF, Yngve DA, Sullivan JA:
Management of femoral shaft fractures in the adolescent. J Pediatr Orthop, 9: 29-32, 1989.
11. Hughes BF, Sponseller PD, Thompson JD: Pediatric femur fractures: effects of spica cast treatment on family and community. J Pediatr Orthop, 15: 457-460, 1995.
12. Kregor PJ, Song KM, Routt ML Jr, Sangeorzan BJ, Liddell RM, Hansen ST Jr: Plate fixation of femoral shaft fractures in multiply injured children. J Bone Joint Surg, 75-A:
1774-1780, 1993.
13. Ligier JN, Metaizeau JP, Prevot J, Lascombes P: Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg, 70-B: 74-77, 1988.
14. Luhmann SJ, Schootman M, Schoenecker PL, Dobbs MB, Gordon JE: Complications of titanium elastic nails for pediatric femoral shaft fractures. J Pediatr Orthop, 23: 443-447, 2003.
15. Martinez AG, Carroll NC, Sarwark JF, Dias LS, Kelikian AS, Sisson GA Jr: Femoral shaft fractures in children treated with early spica cast. J Pediatr Orthop, 11: 712-716, 1991.
16. Narayanan UG, Hyman JE, Wainwright AM, Rang M, Alman BA: Complications of elastic stable intramedullary nail fixation of pediatric femoral fractures, and how to avoid them.
J Pediatr Orthop, 24: 363-369, 2004.
17. Oh CW, Ihn JC, Park BC, et al: Minimally invasive plate osteosynthesis for periarticular tibial fractures. J Korean Orthop Assoc, 36: 449-453, 2001.
18. Oh CW, Park BC, Kim PT, et al: Retrograde flexible intramedullary nailing in children's femoral fractures. Int Orthop, 26: 52-55, 2002.
19. Perren SM: Evolution of the internal fixation of long bone fractures. The scientific basis of biological internal fixation:
choosing a new balance between stability and biology. J Bone Joint Surg, 84-B: 1093-1110, 2002.
20. Reeves RB, Ballard RI, Hughes JL: Internal fixation versus traction and casting of adolescent femoral shaft fractures. J Pediatr Orthop, 10: 592-595, 1990.
21. O'Malley DE, Mazur JM, Cummings RJ: Femoral head avascular necrosis associated with intramedullary nailing in adolescent. J Pediatr Orthop, 15: 21-23, 1995.
22. Sanders JO, Browne RH, Mooney JF, et al: Treatment of femoral fractures in children by pediatric orthopedists: results of a 1998 survey. J Pediatr Orthop, 21: 436-441, 2001.
23. Skaggs DL, Leet AI, Money MD, Shaw BA, Hale JM, Tolo VT: Secondary fractures associated with external fixation in pediatric femur fractures. J Pediatr Orthop, 19: 582-586, 1999.
24. Song HR, Oh CW, Shin HD, et al: Treatment of femoral shaft fractures in young children: comparison between conser- vative treatment and retrograde flexible nailing. J Pediatr Orthop B, 13: 275-280, 2004.
25. Stans AA, Morrissy RT, Renwick SE: Femoral shaft frac- ture treatment in patients age 6 to 16 years. J Pediatr Orthop, 19: 222-228, 1999.
26. Won CH, Chung MS, Lee CS: Ninety-ninety skeletal trac- tion for fractures of the femoral shaft in children. J Korean Orthop Assoc, 25: 1385-1390, 1990.
27. Ziv I, Rang M: Treatment of femoral fracture in the child with head injury. J Bone Joint Surg, 65-B: 276-278, 1983.
= 국문초록 =
목 적: 본 연구의 목적은 최소 침습적 금속판 고정술을 이용하여 소아 대퇴골 간부 골절을 치료하고 그 결과 및 장점을 알아보기 위함이다.
대상 및 방법: 14명의 환아(평균 나이 9.1세)에서 최소 침습적인 금속판 고정술을 시행하였고, 투시 가능한 수술대 위에서 도수 견인술 또는 유연성 골수정으로 임시 정복을 한 후, 근위 및 원위부에 2-3 cm의 절개를 하고, 형광투시경의 도움 하에 금속판을 경피적으로 삽입한 다음, 골절부를 개방치 않고 고정하였다. 골절부는 대퇴 중간부가 10예, 전자하부 2예, 근위부 1예, 원위부 1예 등이었으며, 분쇄성이 7예였고, 다른 부위의 골절 또는 외상을 동반한 경우가 9명이었다. 1년 이상(평균 2.1년)의 추시 후 Flynn 등의 방법에 따라 평가하였다.
결 과: 모든 환자에서 골 이식 없이 골 유합을 얻었으며, 평균 골 유합 기간은 11.1주(범위, 10-14주)였다.
최종 추시상에서 10도 이상의 각형성, 또는 5 mm 이상의 하지 부동을 보인 환자는 없었다. 관절운동의 제한 또는 파행 등의 기능장애 소견이나, 내고정물에 관련된 문제를 나타낸 환자는 없었으며, 최종 임상적 결과에서 모든 환자가 우수의 결과를 보였다.
결 론: 최소 침습적 금속판 고정술은 소아 대퇴골 골절에서 안전하고도 좋은 수술적 치료 방법이 될 것으로 생각된다.
색인 단어: 소아 대퇴골 골절, 최소 침습적 금속판 고정술