요추 추간판 탈출증과 유사한 자발성 경막외 혈종
을지의과대학 노원을지병원 신경외과학교실
경동현·문병관·김주승·강희인·이승진
= Abstract =
Spontaneous Lumbar Epidural Hematoma Mimicking Lumbar Disc Herniation
Dong Hyun Kyung, M.D., Byung Gwan Moon, M.D., Joo Seung Kim, M.D., Hee In Kang, M.D., Seung Jin Lee, M.D.
Department of Neurosurgery, Nowon Eulji General Hospital, Eul Ji College of Medicine, Seoul, Korea
bjective:Spontaneous lumbar epidural hematoma is a rare entity, although the precipitating factors such as anticoagulation therapy frequently precede it. The authors report four cases of surgically confirmed spontane- ous epidural hematoma mimicking lumbar disc herniation.
Methods:Between 1995 and 1998, four patients with spontaneous lumbar epidural hematoma were diagnosed.
The clinical findings which are identical to that of acute disc herniation are included in this study. The operative findings and radiological characteristics are also included.
Results:The magnetic resonance(MR) image findings demonstrated epidural lesions of intermediate to low signal intensity equivalent to those of normal discs on T1-weighted images, and epidural lesions of high signal intensity higher than these normal discs on a T2-weighted image. The image findings also showed rim enhanced pattern of the gadolinium-enhanced T1-weighted MR images. All of the hematomas was associated with a small concomitant disc herniation or underlying annular tear.
Conclusion:The authors speculate that spontaneous lumbar epidural hematoma results from tearing of the fragile penetrating vein caused by underlying disc or annulus disruption between Batson’ plexus and vertebral body.
KEY WORDS:Spontaneous lumbar epidural hematoma・Lumbar disc herniation・Batson’s plexus.
서 론
척수 경막외 혈종은 매우 드문 질환이며 현재까지 전세계적 으로 약 270례, 국내에서는 약 13례가 보고되었다6)13)14)23)
. 발생요인으로는 척추외상, 항응고제 치료, 임산 및 분만후, 출혈성 소인, 척추 동정맥기형, 요추천자 또는 경막외 마취 등이 알려져 있지만 자발성 경막외 혈종은 이러한 요인 없 이 발생원인 불명일 경우를 말한다2)5)9)17)18)22)24)26)28)
. 자발 성 요추 경막외 혈종이 요통 및 하지 방사통과 같은 추간판 탈출증의 증상을 유발하여 수술로써 증명되어 보고 된 것은 전세계적으로 약 30례에 불과하다3-5)8)10)12)16)19)20)25)29)
. 저자들의 교실은 임상 및 방사선학적 소견이 요추 추간판 탈출증과 매우 유사한 4례의 자발성 요추 경막외 혈종을 경
험하였기에 문헌고찰과 함께 보고 하고자 한다.
대상 및 방법
1995년 5월부터 1997년 12월까지 임상 및 방사선학적 으로 요추 추간판 탈출증으로 수핵 제거술을 시술하여 수술 소견과 병리소견이 유기화된 혈액낭으로 밝혀진 4례를 대 상으로 하였다. 환자의 증상은 요통 및 편측의 하지 방사통 이었으며, 이학적 검사상 요추 신경근 긴장 소견이 뚜렷하 였다. 방사선학적으로 단순 요추부 X-선 촬영과 전산화단 층촬영, 척수강조영술 및 핵자기공명영상이 실시되었으며, 탈출형(extrusion) 및 이주형(sequestration) 추간판 탈출 증으로 판독되어 수술현미경을 이용한 디스크 제거술을 하 였다. 환자의 연령 분포, 성별, 증상발현부터 수술까지의 경
OOOO
과기간, 방사선학적 판독소견, 병리학적 소견, 수술소견을 정리하였다(Table 1).
결 과
환자의 연령 분포는 21세에서 34세이고 모두 남자였다.
증상발현부터 수술까지의 경과기간은 2개월에서 6개월까지 였으며 방사선학적 진단을 실시한 시점은 수술 전 15일 이 내였다. 환자의 과거력상 요추부 외상이나 항응고제 치료 및 혈액 응고장애등의 원인이 될만한 특이 소견은 없었다.
초기증상으로 미만성 요통이 갑자기 발생한후 차츰 요통보 다 하지 방사통이 심해지는 양상을 보였다. 신경학적 검사 상 요추 수핵 탈출로 인한 신경근 긴장소견과 동일하였다.
방사선학적으로 척수강조영술에서는 신경근을 압박하고 전 위시킨 전측방 척추강내 종괴, 전산화단층촬영에서는 등신 호 강도로 보여 탈출된 수핵과 분별되지 않았으나 핵자기공 명영상의 T1WI 상에서 종괴는 수핵과 등신호 강도(iso- signal intensity), T2WI 상에서는 수핵보다 고신호 강도 (high signal intensity)를 보였고 조영증강 후 종괴의 가장 자리 증강(marginal enhancement) 소견이 뚜렷하였고 전 산화단층촬영에서는 등신호 강도를 보였다(Fig. 1). 수술소 견상 종괴는 검붉은 색깔의 낭종으로써, 액화된 혈액을 함 유하였고 신경근을 전위시키고 있었다(Fig. 2). 3례에서는 돌출형(protrusion) 수핵 탈출과 동반되었고, 1례에서 섬유 외륜까지의 균열은 보였으나 수핵 탈출은 없었고 모든 례에 서 낭종과 연결된 섬유륜의 파열을 관찰할 수 있었다. 조직 소견은 혈종에 섬유모세포의 증식과 함께 신생모세혈관의 생성이 보이고 혈철소(hemosiderin)를 함유한 조직구(hi- stiocyte)들이 산재하는 섬유화된 혈종 소견이었다(Fig. 3).
수술후 환자들은 하지 방사통과 요통의 호전이 있었다.
고 찰
자발성 척추 경막외 혈종은 문헌상 매우 드문 질환으로써 발생기전으로 여러 가지 가설들이 있으나 3가지로 요약된 다6)11)13)18)23)
. 첫째로 황색인대의 과대신전시 탄력 조직내 의 미세혈관들의 파열로 척추강 후방에 혈종이 발생될 수 있다는 가설로써 황색인대내 혈종의 기전으로 받아들어지고
있다21)28). 둘째로 경막외 지방조직 등에 있던 미세한 혈관
기형이 자발적으로 파열되어 혈종이 발생하며 출혈 당시 파 괴됨에 따라 수술시야에서 확인할 수 없다는 가설로써 국소 적이 아닌 미만성 경막외 혈종의 발생이론으로 받아들여지 고 있다11). 셋째로 경막외 정맥총은 판(valve)없이 흉, 복강 내 정맥인 기정맥(azygous vein) 및 편기정맥(hemiazy- gous vein), 하대정맥(inferior vena cava)과 분절 정맥(seg- mental vein)을 통해 교통하고 있어 흉, 복강내의 갑작스런 압력 상승시에 경막외 정맥총의 팽창과 함께 파열됨으로써 혈종이 형성된다는 것이다15)18)21)25)
. 이 이론은 많은 환자들 의 병력에서 알 수 있듯이 경미한 외상, 재채기, 무거운 물 건을 들어올리는 자세 등, valsalva maneuver가 원인이 된 다고 기술하고 있으나, 일반적으로 valsalva maneuver시 혈종 발생빈도가 매우 드문 점을 고려한다면 타당성이 적다 고 하겠다28).
1993년 Wiltse와 Fonseca등30)의 연구에 의하면 척추강 내면을 싸고 있는 경막외막(peridural membrane)은 척추체 후면과 경막외 지방조직 및 정맥총 사이에 위치하며 Bat- son’s plexus와 교통하는 관통 정맥(perforating vein)이 경막외막을 투과하여 척추체 골수와 연결되어 있고 추체와 경막외막 사이는 잠재적 공간(potential space)으로 존재한 다고 보고하였다.
Table 1. Sex, age, duration of symptom, clinical symptoms, preoperative study, radiological and pathological diagnosis in spontaneous lumbar epidural hematoma(n=4)
Sex/Age Duration of
symptom Clinical
symptoms Preoperative study Radiological diagnosis Pathological diagnosis Case 1 M/27 5 months LBP, L3 & L4 Lumbar MRI R/O Schwannoma Venous ectasia
radiculopathy HNP L3-4, with organizing thrombus
central to left protrusion Organizing hematoma Case 2 F/34 2 months LBP & S1 Lumbar CT Extruded disc herniation Organizing hematoma
radiculopathy right L5-S1, caudal migration
Case 3 M/24 6 months LBP & L5 Lumbar MRI Extruded disc herniation Organizing hematoma radiculopathy Lumbar CT myelogram right L4-5,caudal migration
Lumbar myelogram R/O neural tumor
Case 4 M/21 2 months LBP & S1 Lumbar CT Extruded disc herniation Organizing hematoma radiculopathy right L5-S1, caudal migration
LBP:low back pain, R/O:rule out, HNP:herniated nucleus pulposus
1993년 Gundry등10)은 18례의 수술로 확인된 요추 경 막외 혈종 중 14례에서 동반된 수핵탈출과 섬유륜 파열을 볼 수 있었다고 보고하였다.
저자들의 경우 4례 중 3례에서 수핵탈출과 동반하였고 1 례는 섬유륜 파열이 관찰되었다. 수핵 탈출로 인한 신경근 압박소견과 유사하게 보이는 자발성 요추 경막외 혈종은 수 핵 탈출이나 섬유륜의 파열로 인한 장력이 경막외막을 투과 하는 관통정맥의 파열을 유도하고 이로 인한 출혈이 막전공 간(premembranous space)에 축적되어 팽창함으로써 발 생될 가능성이 높다고 추정할 수 있었다. 임상적으로 증상 발현 시초에 미만성 요통으로 시작한 것은 수핵 탈출과 섬
유륜 파열로 인한 섬유외륜의 통증 감각신경의 긴장으로 발 생되며 처음부터 방사통이 심하지 않은 이유는 신경근을 압 박할 만큼 충분한 압력으로 혈종이 발생한 것이 아니며 혈 종 발생 후 혈종의 유기화 과정에서 만성 뇌경막하 혈종의 성장기전과 같이 혈종의 액화 및 삼투압편차에 의한 혈종의 만성적 팽창이 신경근 압박증상을 서서히 유도한 것으로 추 정된다. 방사선학적으로 요추부 전산화단층촬영이나 척수강 조영술로는 요추 추간판 탈출증과 구분할 수 없었고 핵자기 공명영상에서는 구분이 가능하였다. 즉, T2WI 상에서 종괴 의 내부가 등밀도의 고신호 강도로 뇌척수액의 신호 강도만 큼 높은 점이 등신호 강도의 추간판 탈출증과 구분되는 점
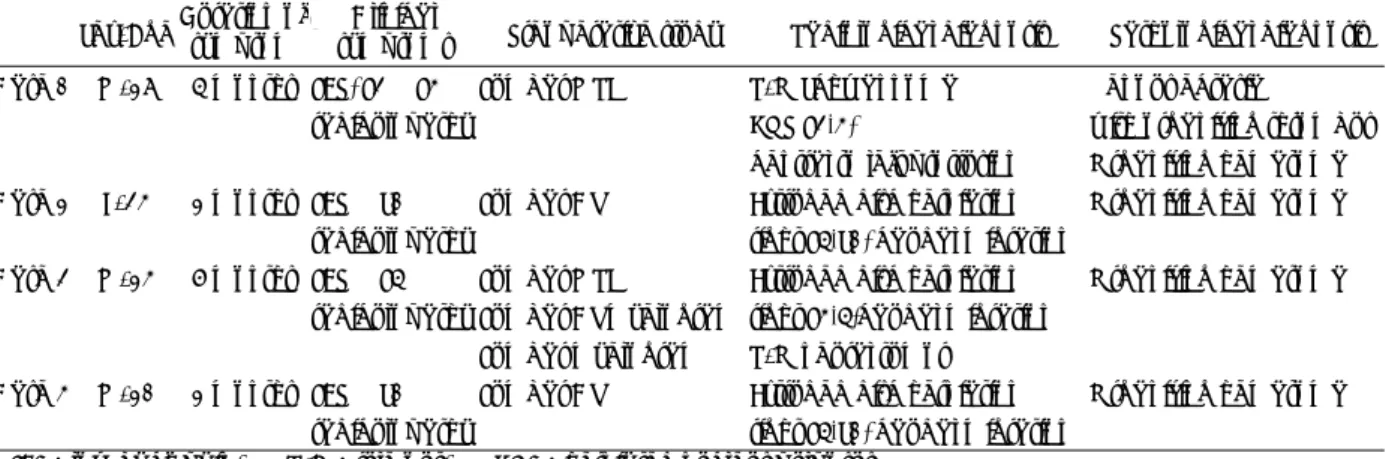
Fig. 1. Lumbar spine radiologic finding(case 3). Axial MR images showing iso-signal intensity in T1WI(A), high signal intensity in T2WI(B), and rim enhancement in Gd-enhanced MR(C). Axial CT showing isodensity(D).
A AA
A BB BB
D D D D
C C C C
이다. 단순한 경막외 혈종인지 그 원인으로써 수핵 탈출 또 는 섬유륜 파열로 인한 것인지를 알기 위해서는 추간판조영 술 및 전산화단층촬영술을 하여 조영제가 섬유륜 균열을 통
해 누출되어 종괴 내부로 충만되는지를 확인함으로써 가능 하다고 하였다29)30). 신경근 긴장이 뚜렷한 막전공간의 요추 부 자발성 경막외 혈종의 치료는 수술적 치료와 보존적 치 료로 구분할 수 있다. 자발성 척추 경막외 혈종의 자연 소실 은 1979년 Correa등7)이 경추부에서 처음 보고 한 이래, 1989년 Avraham등1)이 흉추에서, 1994년 Kingery등15)이 요추부에서 각각 보고하였다. 문헌 조사에 따르면 대부분이 경추부와 흉추부에서 발생하며 임상 경과가 급속히 악화됨 에 따라 즉시 혈종 제거술을 시행한 것을 알 수 있다. 그러 나 요추부에서 국소적으로 막전공간에 생기는 자발성 만성 경막외 혈종에 대한 수술적 치료에 대해서는 논란의 여지가 있다. 그 이유는 이러한 질환이 매우 희귀하며 보존적 치료 와의 비교 보고가 아직 없다는 점이다.
저자들은 만약 신경근 긴장으로 인한 신경학적 결함이 뚜렷하거나 악화되고 있는 상태에서는 추간판조영술 및 전 산화단층촬영을 하여 수핵 탈출의 돌출형과 동반된 경우라 면 수술적 치료가 좋으며 수핵탈출증과 동반되지 않았다면 우 선 보존적 치료후 증상의 악화를 보일 경우 신경공을 통한 내 시경적 낭종 흡인술(transforaminal endoscopic cyst as- piration)을 고려하는 것이 바람직할 것으로 생각하였다.
결 론
임상적으로 요추 추간판 탈출증과 유사한 증상을 보이는 자발성 경막외 혈종은 드문 질환으로써 핵자기공명영상으로 구분될 수 있고 수핵 탈출과의 동반여부를 확인하기 위해서 는 추간판조영술 및 전산화단층촬영이 유용할 것으로 판단 된다. 저자들의 신경외과학교실에서 수술로 증명된 4례를 문헌고찰과 함께 보고하는 바이다.
•논문접수일:1999년 6월 16일
•심사완료일:2000년 3월 16일
•책임저자:문 병 관
139-711 서울 노원구 하계 1동 280-1번지 을지의과대학 노원을지병원 신경외과학교실 전화:02) 970-8268, 전송:02) 975-7811 E-mail:[email protected]
References
1) Avraham E, Tadmor R, Ram Z, Feibel M, Itzhak Y:MR de- monstration of spontaneous acute epidural hematoma of the thoracic spine. Neuroradiology 31:89-92, 1989
2) Beatty RM, Winston KR:Spontaneous cervical epidural he- matoma:A consideration of etiology. J Neurosurg 61:143- 148, 1984
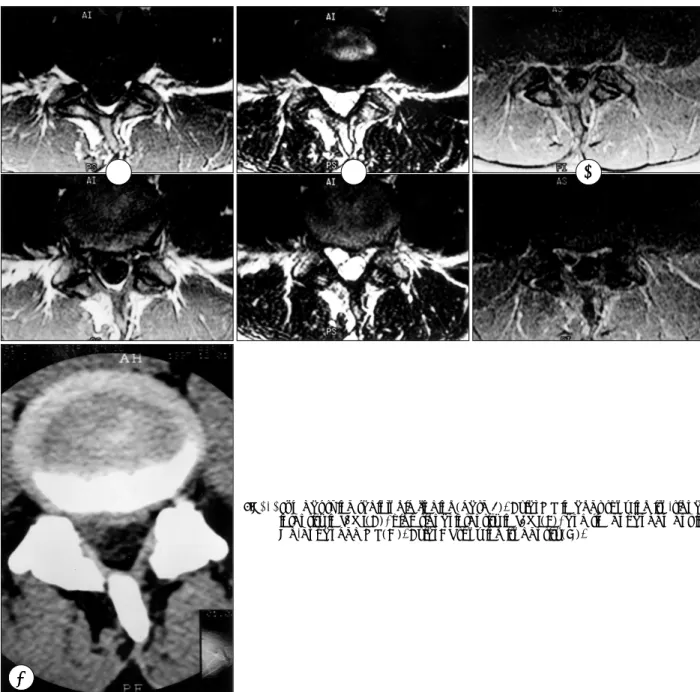
Fig. 2. Intraoperative photograph. Redpurplish colored cystic mass(arrow) showing underneath retracted nerve root.
Fig. 3. Photomicrograph of a representative section of the lesion showing a diffuse hemosiderin infiltration and capillary neovascularization on the fibrous background (HE staining, ×200).
3) Boyd HR, Pear BL:Chronic spontaneous spinal epidural he- matoma:Report of two cases. J Neurosurg 36:239-242, 1972 4) Caldarelli M, Di Rocco C, La Marca F:Spontaneous spinal epidural hematoma in toddlers:Description of two cases and review of the literature. Surg Neurol 41(4):325-329, 1994 5) Calliauw L, Dhara M, Martens F, Vannerem L:Spinal epi-
dural hematoma without lesion of the spine. Clin Neurol Neu- rosurg 90(2):131-136, 1988
6) Chung HS, Chu JW, Lee KC, Lee HK:Acute spontaneous spinal epidural hematoma. J Korean Neurosurg Soc 9(1): 299-303, 1980
7) Correa AV, Breasley BAL:Spontaneous cervical epidural hematoma with complete recovery. Surg Neurol 10(4):227- 228, 1978
8) Devadiga KV, Gass HH:Chronic lumbar extradural hae- matoma simulating disc syndrome. J Neurol Neurosurg Psy- chiatry 36(2):255-259, 1973
9) Foo D, Rossier AB:Preoperative neurological status in pre- dicting surgical outcome of spinal epidural hematoma. Surg Neurol 15(5):389-401, 1981
10) Gundry CR, Heithoff KB:Epidural hematoma of the lumbar spine:18 surgically confirmed cases. Radiology 187(2):427- 431, 1993
11) Han DI, Lee SW, Park CK, Park YS, Kang JK, Song JU:
Two case of spontaneous extradural hematoma on the lumbar spine. J Korean Neurosurg Soc 17(5):1113-1117, 1988 12) Harris ME:Spontaneous epidural spinal hemorrhage. AJR
105:383-385, 1969
13) Hwang YS, Kim YS, Choi JU, Park HC, Kim SJ:Spontane- ous spinal epidural hematoma. J Korean Neurosurg Soc 15 (3): 545-551, 1986
14) Jackson FE:Spontaneous spinal epidural hematoma coinci- dent with whooping cough. J Neurosurg 20:715-716, 1963 15) Kingery WS, Seibel M, Date ES, Marks MP:The natural
resolution of a lumbar spontaneous epidural hematoma and associated radiculopathy. Spine 19(1):67-69, 1994 16) Kotilainen EM, Pajulo O:Spontaneous epidural hematoma
as a cause of sciatic pain in a schoolboy. Pediatr Neurol 17(4): 350-352, 1997
17) Lee KS, McWhorter JM, Angelo JN:Spinal epidural hema- toma associated with Paget's disease. Surg Neurol 30:131-
134, 1988
18) Lee MS, Kwon Y, Jung HW, Kim HJ, Chi JG:Spinal epi- dural hematoma caused by ruptured vascular malformation. J Korean Neurosurg Soc 14(2):443-450, 1985
19) Levitan LH, Wiens CW:Chronic lumbar extradural hema- toma:CT findings. Radiology 148:707-708, 1983
20) Markham JW, Lynge HN, Stahlman GE:The syndrome of spontaneous spinal epidural hematoma. Report of three case.
J Neurosurg 26(3):334-342, 1967
21) Mirkovic S, Melany M:Case report:A thoracolumber epi- dural hematoma simulating a disc syndrome. J Spinal Disord 5:112-115, 1992
22) Packer NP, Cummins BH:Spontaneous epidural haemorr- hage:A surgical emergency. Lancet 18(8060):356-358, 1978 23) Paik JM, Chung H, Choi GH, Yeo HT, Rhee JK:A case of
spontaneous cervical spinal epidural hematoma. J Korean Neu- rosurg Soc 20(6):480-486, 1991
24) Pan G, Kulkarni M, MacDougall DJ, Miner ME:Traumatic epidural hematoma of the cervical spine:Diagnosis with magnetic resonance imaging. J Neurosurg 68:798-801, 1988 25) Pear BL:Spinal epidural hematoma. Am J Roentgenol Ra-
dium Ther Nucl Med 115:155-164, 1972
26) Robertson WC Jr, Lee YE, Edmonson MB:Spontaneous spi- nal epidural hematoma in the young. Neurology 29(1):120- 122, 1979
27) Stephanov S, Preux J:Lumbar epidural hematoma following epidural anesthesia. Surg Neurol 18(5):351-353, 1982 28) Sweasey TA, Coester HC, Rawal H, Blaivas M, McGillicuddy
JE:Ligamentum flavum hematoma:Report of two cases. J Neurosurg 76:534-537, 1992
29) Watanabe N, Ogura T, Kimori K, Hase H, Hirasawa Y:
Epidural hematoma of the lumbar spine, simulating extruded lumbar disc herniation:Clinical, discographic, and enhanced magnetic resonance imaging features. A case report. Spine 22 (1):105-109, 1997
30) Wiltse LL, Fonseca AS, Amster J, Dimartino P, Ravessoud FA:Relationship of the dura, Hofmann’s ligaments, Batson’s plexus, and a fibrovascular membrane lying on the posterior surface of the vertebral bodies and attaching to the deep layer of the posterior longitudinal ligament. An anatomical, radio- logic, and clinical study. Spine 18(8):1030-1043, 1993