저작자표시-비영리-변경금지 2.0 대한민국 이용자는 아래의 조건을 따르는 경우에 한하여 자유롭게 l 이 저작물을 복제, 배포, 전송, 전시, 공연 및 방송할 수 있습니다. 다음과 같은 조건을 따라야 합니다: l 귀하는, 이 저작물의 재이용이나 배포의 경우, 이 저작물에 적용된 이용허락조건 을 명확하게 나타내어야 합니다. l 저작권자로부터 별도의 허가를 받으면 이러한 조건들은 적용되지 않습니다. 저작권법에 따른 이용자의 권리는 위의 내용에 의하여 영향을 받지 않습니다. 이것은 이용허락규약(Legal Code)을 이해하기 쉽게 요약한 것입니다. Disclaimer 저작자표시. 귀하는 원저작자를 표시하여야 합니다. 비영리. 귀하는 이 저작물을 영리 목적으로 이용할 수 없습니다. 변경금지. 귀하는 이 저작물을 개작, 변형 또는 가공할 수 없습니다.
TLR4 endogenous ligand S100A8/A9 levels
in adult-onset Still’s disease
and their association with disease activity and
clinical manifestations
by
Hyoun-Ah Kim
Major in Medicine
Department of Medical Sciences
The Graduate School, Ajou University
TLR4 endogenous ligand S100A8/A9 levels in
adult-onset Still’s disease
and their association with disease activity and
clinical manifestations
by
Hyoun-Ah Kim
A Dissertation Submitted to The Graduate School of
Ajou University in Partial Fulfillment of the Requirements
for the Degree of Ph. D.
of Medicine
Supervised by
Chang-Hee Suh, M.D., Ph.D.
Rheumatology
Department of Rheumatology
The Graduate School, Ajou University
August, 2015
This certifies that the dissertation
of Hyoun-Ah Kim is approved.
SUPERVISORY COMMITTEE
Sun Park
Kyi Beom Lee
Chang-Hee Suh
Jisoo Lee
You-Sun Kim
The Graduate School, Ajou University
June, 19th, 2015
- ABSTRACT -
TLR4 endogenous ligand S100A8/A9 levels
in adult-onset Still’s disease and their association
with disease activity and clinical manifestations
Objective: S100A8/A9 has been suggested as a biomarker of disease activity in patients with systemic juvenile idiopathic arthritis or adult-onset Still’s disease (AOSD). We investigated the clinical significance and the pathogenic role of this marker in AOSD.
Materials and Methods: Serum samples were collected from 36 AOSD patients, 40 rheumatoid arthritis (RA) patients, and 33 healthy controls (HC) for enzyme-linked immunosorbent assay (ELISA) of S100A8/A9, follistatin-like protein 1 and interleukin-18 (IL-18). Of the AOSD patients, follow-up samples were collected from 16 patients after resolution of disease activity. Furthermore, S100A8/A9 expression levels in biopsy specimens obtained from 26 AOSD patients with skin rashes and 8 AOSD with lymphadenopathy were investigated via immunohistochemistry. Peripheral blood mononuclear cells (PBMC) from active AOSD and HC were evaluated for IL-1β release, and in vitro study with PBMC and THP-1 cell line was done for cell signal of S100A8/A9.
Results: Serum S100A8/A9 in AOSD patients was higher than those of RA patients and HC. However, follistatin-like protein 1 in AOSD was not different from RA and HC. The IL-18 levels of AOSD were higher than those of RA and HC. Serum S100A8/A9 correlated with leukocyte count, erythrocyte sedimentation rate, C-reactive protein (CRP), ferritin, and
systemic score, however the IL-18 correlated only with ferritin and systemic score. In addition, S100A8/A9 was decreased after disease activity was resolved in followed-up AOSD patients. Furthermore, the IL-1β and TNF-α levels of AOSD were higher than those of HC. Serum S100A8/A9 levels correlated with IL-1β, TNF-α, ferritin, and CRP. The grade of inflammatory cells expressing S100A8/A9 ranged from 1 to 3 in skin and lymph node biopsies of active AOSD. The grading of staining of S100A8/A9 was more intense in inflammatory cells of skin lesions with karyrrhexis (p=0.028), mucin deposition (p=0.014), and neutrophil infiltration (p=0.006). Furthermore, the correlation between inflammatory cell grading of CD68 and that of S100A8/A9 was shown (p<0.001) in skin biopsies. S100A9 was a strong inducer of IL-1β expression in peripheral blood mononuclear cells. S100A9 induced signal transduction pathways, including JNK and p38 in PBMC from HC and AOSD patients.
Conclusion: The data suggest that serum S100A8/A9 may be a useful biomarker for evaluating disease activity in AOSD patients. Furthermore, S100A8/A9 may contribute to the inflammatory response by induction of inflammatory cytokines, and serve as a clinicopathological marker for assessment of disease activity in AOSD.
Key words: Adult-onset Still’s disease, S100A8/A9, disease activity, biomarker, interleukin-1β
TABLE OF CONTENTS
ABSTRACT ··· i
TABLE OF CONTENTS ···iii
LIST OF FIGURES ··· iv
LIST OF TABLES ··· vi
. Ⅰ INTRODUCTION ··· 1
. Ⅱ MATERIALS AND METHODS ··· 4
. Ⅲ RESULTS ··· 9 . Ⅳ DISCUSSION ··· 34 . Ⅴ CONCLUSION ··· 39 REFERENCES ··· 40 국문요약 ··· 48
LIST OF FIGURES
Fig. 1. The levels of S100A8/A9 (A), follistatin-like protein 1 (B), and interleukin-18 (C) in 36 adult-onset Still’s disease (AOSD), 40 rheumatoid arthritis (RA) patients, and 33 healthy controls (HC) ··· 11
Fig. 2. The receiver-operating characteristic (ROC) curves for S100A8/A9, follistatin-like protein 1, interleukin-18 (IL-18), C-reactive protein (CRP), and ferritin levels in adult-onset Still’s disease and controls ··· 12
Fig 3. The levels of S100A8/A9 (A), follistatin-like protein 1 (B), and interleukin-18 (C) in 16 patients with adult-onset Still’s disease (AOSD) according to disease activity ·· 15
Fig. 4. The levels of interleukin-1β (IL-1β) (A) and tumor necrosis factor-α (TNF-α) (B) in 20 patients with active adult-onset Still’s disease (AOSD) and 20 healthy controls (HC). ··· 17
Fig. 5. The correlation between S100A8/A9 and inflammatory markers, such as inteleukin-1β (IL-1β), tumor necrosis factor-α (TNF-α), ferritin, and C-reactive protein (CRP) in patients with adult-onset Still’s disease and healthy controls ··· 18
Fig. 7. Lymph node biopsy findings in patients with adult-onset Still’s disease ··· 25
Fig. 8. S100A8/A9 expression levels in inflammatory cells in skin biopsy of patients with adult-onset Still’s disease ··· 26
Fig. 9. S100A8/A9 expression levels in inflammatory cells in lymph node biopsy of patients with adult-onset Still’s disease ··· 29
Fig. 10. Interleukin-1β (IL-1β) secretion after treatment with S100A9 in peripheral blood monocytes from healthy controls (HC) and patients with adult-onset Still’s disease (AOSD) ··· 30
Fig. 11. Activation of JNK and p38 in a human monocyte cell line after treatment with S100A9 or S100A8/A9 ··· 31
Fig. 12. Activation of JNK and p38 after treatment with S100A9 in peripheral blood mononuclear cells (PBMC) from healthy controls (HC) and patients with active adult-onset Still’s disease (AOSD) ··· 32
Fig. 13. Toll like receptor 4 (TLR4) expression in peripheral blood mononuclear cells (PBMC) from healthy controls (HC) and patients with active adult-onset Still’s disease (AOSD) ··· 33
LIST OF TABLES
Table 1. Clinical characteristics of patients ··· 9
Table 2. Correlation between disease activity markers and systemic score in 36 patients with adult-onset Still’s disease ··· 14
Table 3. Correlation between the change of disease activity markers and the change of systemic score in follow-up 16 patients with adult-onset Still’s disease ··· 16
Table 4. Histopathologic and immunohistochemical staining features of skin in adult-onset Still’s disease ··· 19
Table 5. Histopathologic and immunohistochemical staining features of lymph node in adult-onset Still’s disease ··· 24
Table 6. The inflammatory cell staining for S100A8 and S100A9 of skin in adult-onset Still’s disease ··· 27
Table 7. Correlations between inflammatory cell grading of CD4, CD8 and CD68 staining and that of S100A8 and S100A9 staining ··· 28
I. INTRODUCTION
Adult-onset Still’s disease (AOSD) is a systemic inflammatory disorder of unknown etiology that is analogous to the systemic form of juvenile idiopathic arthritis (systemic JIA). AOSD is characterized by spiking fever, arthritis, evanescent rash, elevated liver enzymes, lymphadenopathy, hepatosplenomegatly, and serositis (Bywaters, 1971; Fautrel, 2008). However, the spectrum of differential diagnoses is wide and includes infectious, neoplastic, and autoimmune disorders, which should be ruled out before the diagnosis of AOSD. Since the symptoms and laboratory results are not disease specific, diagnosis of AOSD and accurate determination of disease activity is difficult (Ohta et al., 1987; Pouchot et al., 1991; Efthimiou et al., 2007; Cagatay et al., 2009). The most commonly used biomarkers for AOSD have included the erythrocyte sedimentation rate (ESR), serum C-reactive protein (CRP) and ferritin, but these are nonspecific markers. Therefore, a simple biomarker that could be used to evaluate disease activity would be very useful.
S100A8 and S100A9 are two calcium-binding proteins that belong to the S100 family (Edgeworth et al., 1991). S100A8 and S100A9 form heterodimers that are the biologically relevant forms, and those are expressed by infiltrating monocytes and neutrophils under inflammatory conditions, but not in quiescent resident macrophages and lymphocytes (Foell et al., 2004; Vogl et al., 2004; Vogl et al., 2007; Raquil et al., 2008). S100A8/A9 can be detected in high levels in serum and body fluids in patients with different types of infectious, inflammatory, and malignant disorders (Striz et al., 1993; van Zoelen et al., 2009). Some studies showed that systemic JIA was associated with high concentrations of S100A8/A9 (Frosch et al., 2003; Frosch et al., 2009). Recently, one study reported that
serum S100A8/A9 was increased in patients with AOSD and correlated with disease activity (Jung et al., 2010).
Follistatin-like protein 1, originally cloned from an osteoblast cell line as a transforming growth factor β-inducible gene, was found to be highly overexpressed in mouse paws during early arthritis (Shibanuma et al., 1993; Thornton et al., 2002). Follistatin-like protein 1 has been found in rheumatoid arthritis (RA) synovial tissue, and anti-follistatin-like protein 1 antibodies have been detected in the serum and synovial fluid of RA patients (Tanaka et al., 1998; Clutter et al., 2009). Also, transfection of follistatin-like protein 1 into macrophages and fibroblasts led to the up-regulation of inflammatory cytokines that are believed to play central roles in chronic arthritis (Clutter et al., 2009). A recent study demonstrates that follistatin-like protein 1 may represent a useful biomarker of disease activity in systemic JIA (Wilson et al., 2010).
Interleukin-18 (IL-18), originally described as interferon-γ inducing factor, seems to exert powerful Th1-promoting activities in synergy with IL-12 (Ushio et al., 1996). Macrophages, Kupffer cells, keratinocytes, articular chondrocytes, synoviocytes, and osteoblasts are able to synthesize IL-18 (Lotito et al., 2007). Many studies have revealed a broad spectrum of effects that implicate IL-18, a member of the IL-1 superfamily, as a pivotal regulator of chronic inflammation in human autoimmune diseases (Dinarello, 2000). Serum levels of IL-18 were reported to be elevated in patients with active AOSD compared to those with other autoimmune diseases like systemic lupus erythematosus (SLE), RA, and systemic sclerosis (Kawashima et al., 2001). Serum IL-18 levels in the steroid nonresponders were significantly higher than in the steroid responders (Yamaguchi et al., 1992). Also, we
previously reported elevated concentrations of IL-18 in patients with active and inactive AOSD (Choi et al., 2003).
It has been reported that the serum levels of S100A8/A9, follistatin-like protein 1, and IL-18 are elevated and suggested to be disease activity markers in AOSD or systemic JIA. However, the sample sizes in those studies were small, and there has been no study regarding follistatin-like protein 1 in AOSD. Therefore, we have investigated the clinical significance of S100A8/A9, follistatin-like protein 1, and IL-18 in Korean AOSD patients with serial samplings. Furthermore, to explore the in vivo involvement of S100A8/A9 in AOSD, we prospectively recruited active AOSD patients, RA, and HC for investigation of correlation between S100A8/A9 and inflammatory cytokines. Immunohistochemically stained biopsy specimens were obtained from skin lesions of 26 patients and lymph nodes of 8 patients with active untreated AOSD for S100A8/A9. In addition, we investigated the link between IL-1β and S100A8/A9 in peripheral blood mononuclear cells (PBMC) and THP-1 cell line.
II. MATERIALS AND METHODS
1. Subjects
Thirty-six AOSD patients, 40 RA patients as a disease control, and 33 healthy controls (HC) were included in the study. AOSD patients were diagnosed according to Yamaguchi’s criteria (Yamaguchi et al., 1992) after exclusion of common infections and hematological and autoimmune diseases. RA patients satisfied the American College of Rheumatology (ACR) 1987 revised criteria for the classification of RA (Arnett et al., 1988). Serum samples were collected from patients and controls. Of the 36 AOSD patients, follow-up samples were collected from 16 patients after resolution of disease activity. All blood samples were stored at -20˚C immediately after collection.
Information on the medical history, clinical symptoms, and physical examinations was entered into a database when serum sampling was done. Each patient also underwent a series of laboratory tests, including complete blood count (CBC), ESR, CRP, rheumatoid factor (RF), anti-nuclear antibody (ANA), ferritin (normal 13-150 ng/mL for women and 30-400 ng/mL for men), liver function tests, and urinalysis. AOSD disease activity was evaluated according to the method described by Pouchot et al.(Pouchot et al., 1991), which assigns a score from 0 to 12 and adds 1 point for each of the following manifestations: fever, typical rash, pleuritis, pneumonia, pericarditis, hepatomegaly or abnormal liver function tests, splenomegaly, lymphadenopathy, leukocytosis ≥ 15,000/mm2, sore throat, myalgia, and
abdominal pain. We defined resolution of disease activity of AOSD with this score ≤ 2, arbitrarily.
2. S100A8/A9, follistatin-like protein 1, IL-18, IL-1β and TNF-α
assay
Serum S100A8/A9 levels were measured using commercial enzyme-linked immunosorbent assay kits (Buhlmann Laboratories, Schonenbuch, Switzerland) according to the manufacturer’s instructions. Follistatin-like protein 1 levels were also determined using an enzyme-linked immunosorbent assay kits (USCN life, Wuhan, China) according to the manufacturer’s instructions. Also, serum IL-18 levels were measured using commercial enzyme-linked immunosorbent assay kits (eBioscience, SanDiego, CA, USA) according to the manufacturer’s instructions. Serum IL-1β and tumor necrosis factor-α (TNF-α) levels were measured using commercial enzyme-linked immunosorbent assay kits (R & D Systems, Minneapolis, MN, USA) according to the manufacturer’s instructions.
3. Histopathologic analysis of skin biopsy and lymph node
Skin biopsies were obtained from 26 patients with active AOSD and lymph node biopsies from 8 patients. We evaluated the hematoxylin and eosin-stained sections. The slides were independently examined by 2 pathologists (JHH and HY) with respect to the following skin histological parameters: (1) epidermal change, (2) degree of inflammatory cell infiltration, presence of (3) karyorrhexis, (4) vasculitis, and (5) interstitial mucin. Lymph node histological parameters were evaluated with respect to (1) different patterns of reaction (follicular, paracortical or diffuse hyperplasia), (2) kinds of infiltrating inflammatory cells, (3) degree of immunoblast proliferation, and (4) degree of vascular proliferation.
4. Immunohistochemistry and evaluation
Immunohistochemistry and in situ hybridization of Epstein-Barr virus-encoded RNA (EBER) were performed with primary antibodies for rule out of EB virus infection on 4-µm-thick representative tissue sections of formalin-fixed, paraffin-embedded tissue section. The results of immunohistochemistry were analyzed in the Benchmark XT automated immunohistochemistry stainer (Ventana Medical Systems Inc, Tucson, AZ, USA). The primary antibodies used were given as follows: CD4, 1:10 and CD8, 1:50 (Thermo Fisher Scientific, Fremont, CA); CD68, 1:200 (Novocastra Laboratories Ltd, Newcastle, United Kingdom); S100A8, 1:400 and S100A9, 1:500 dilution (Abcam Systems, Cambridge, MA, USA). Detection was done using the Ventana Optiview DAB Kit (Ventana Medical Systems). Each marker was recorded as the numbers of positive inflammatory cells divided by the numbers of total inflammatory cells, then expressed as a graded on a scale from 1 to 3: 1,1-33%; 2, 34-66%,; 3, 67-100% (CD4, CD8, CD68, S100A8/A9). In situ hybridization for the detection of EBER was performed by first applying the Epstein-Barr virus probe (Novocastra Labroatories Ltd) that contains a random mixture of fluorescein isothiocyanate (FITC)-labeled oligonucleotides that hybridize to EBER1 and EBER2. An anti-FITC antibody was subsequently added and detection was performed with the Ultratech HRP streptavidin-biotin universal detection system (Immunotech, Marseille, France). The data on immunofluorescence staining of 5-µm-thick frozen tissue sections was available in 11 cases of skin biopsies. The panel included polyclonal antibodies to IgG (1:40 dilution; DAKO, Glostrup, Denmark), IgA (1:40 dilution; DAKO), IgM (1:40 dilution; DAKO), C3 (1:40 dilution; DAKO), and fibrinogen (1:40 dilution, DAKO).
5. PBMC preparation and stimulation
PBMC were isolated from human buffy coats and cultured from 6 patients with active AOSD and 6 HC. PBMC were incubated for 24 hours with lipopolysaccharide (LPS) (10ng/mL; Sigma, Deisenhofen, Germany), S100A8/A9 or S100A9 (5 µg/mL), and IL-1β concentrations in supernatants were determined by ELISA (R & D Systems). In parallel sets of experiments, PBMC were primed for 16 hours with interferon-γ (500 IU/mL; Bender MedSystems, Vienna, Austria) prior to stimulation with LPS, S100A8/A9 or S100A9.
6. Cell culture
THP-1 cells were cultured in Dulbecco’s Modified Eagle’s Medium with 10% FBS, 2 mmol/L glutamine, 100 U/mL penicillin, and 100 mg/mL streptomycin. No further authentication of cell lines was done by the authors.
7. Western blot
Upon treatment, cell lines or PBMC were lysed in 20 mM Tris (pH 7.0), 250 mM NaCl, 3 mM EDTA, 3 mM EGTA, 2 mM DTT, 0.5% NP-40, 0.5 mM PMSF, 20 mM β-glycerol phosphate, 1 mM sodium vanadate, and 1 μg/ml leupeptin. Lysates were loaded onto 10 or 12% SDS-PAGE gels. Following transfer and blotting, the proteins of interest were visualized by enhanced chemiluminescence (Pierce, IL, USA) and analyzed.
8. Statistical analysis
The statistical analysis was performed using SPSS, version 12.0 (SPSS, Chicago, IL, USA). A p-value < 0.05 was regarded as statistically significant. The data are shown as
mean ± standard deviation (SD). Differences in S100A8/A9, follistatin-like protein 1, and cytokine levels were determined by a Mann Whitney U test. The ability of S100A8/A9, follistatin-like protein 1, IL-18, ferritin, and CRP to accurately diagnose AOSD patients was evaluated by a Receiver-Operating Characteristics (ROC) analysis. The correlations between their levels and disease activity markers were evaluated with a Spearman’s correlation test. The Wilcoxon signed-rank test was also used to compare levels and disease activity markers in the patients who had follow-up sampling.
RESULTS
1. Clinical characteristics of the patients
The mean age of the AOSD patients was 40.3 ± 13.6 years, and females comprised 81.6%. There were no significant differences in age and gender between groups (Table 1). The main clinical symptoms in AOSD patients included high spiking fever (69.4%), skin rash (72.2%), sore throat (50%), arthritis (52.8%), and lymphadenopathy (36.1%).
Table 1. Clinical characteristics of patients
AOSD (n = 36) RA (n = 40) HC (n = 33) Age (year) 40.3 ± 13.6 40.7 ± 12.5 38.5 ± 7.7 Gender (F/M) 31/5 35/5 31/2 Fever 25 (69.4) 0 (0) Sore throat 18 (50) 0 (0) Skin rash 26 (72.2) 0 (0) Lymphadenopathy 13 (36.1) 0 (0) Splenomegaly 10 (27.8) 0 (0) Hepatomegaly 6 (16.7) 0 (0) Pericarditis 4 (11.1) 0 (0) Pleuritis 4 (11.1) 0 (0) Arthralgia 31 (86.1) 40 (100) Arthritis 19 (52.8) 40 (100) Hemoglobin, g/dL 11.4 ± 1.6 12.0 ± 1.7
Leukocyte, /μL 14,251 ± 5,887 7,074 ± 3,229 Platelet, x103/μL 427.5 ± 788.6 312.4 ± 82.5 Ferritin, ng/mL 4,395.6 ± 496.7 64.5 ± 78 54.2 ± 58.4 ESR, mm/hr 56.3 ± 37.4 29.6 ± 32.6 CRP, mg/dL 9.03 ± 88.41 1.08 ± 1.7 0.09 ± 0.21 AST, mg/dL 91.2 ± 125.7 19.8 ± 5.7 ALT, mg/dL 78.7 ± 111.5 20.6 ± 7.6 ANA positivity 3 (8.3) 12 (30) RF positivity 5 (13.9) 28 (70) Systemic score 4.5 ± 2.34 DAS-28 3.8 ± 1.41 4.3 ± 1.38
AOSD, adult-onset Still’s disease; RA, rheumatoid arthritis; HC, healthy control; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; AST, aspartate transaminase; ALT, alanine transaminase; ANA, antinuclear antibody; RF, rheumatoid factor; DAS-28, disease activity score including 28 joints. All values presented as number (%) or mean ± standard deviation.
2. Serum S100A8/A9, follistatin-like protein 1 and IL-18 levels
S100A8/A9, follistatin-like protein 1, and IL-18 levels in AOSD patients, RA patients, and HC were shown in Fig. 1. The S100A8/A9 levels of AOSD (11.77 ± 8.84 μg/mL) were higher than those of RA (3.53 ± 3.43 μg/mL, p < 0.001) and HC (2.49 ± 1.83 μg/mL, p < 0.001). Also, the IL-18 levels of AOSD (7560.3 ± 7577.6 pg/mL) were higherHowever, follistatin-like protein 1 levels of AOSD were not.
Fig. 1. The levels of S100A8/A9 (A), follistatin-like protein 1 (B), and interleukin-18 (C) in 36 adult-onset Still’s disease (AOSD), 40 rheumatoid arthritis (RA) patients, and 33 healthy controls (HC). Data are expressed as the mean ± SD. A Mann Whitney test was
used to perform the statistical analysis.
In the ROC analysis of S100A8/A9, follistatin-like protein 1, IL-18, CRP and ferritin, area under the curve (AUC) was 0.845 (95% CI 0.753-0.937, p < 0.001), 0.436 (95% CI 0.299-0.573, p = 0.527), 0.983 (95% CI 0.961-1.005, p < 0.001), 0.927 (95% CI 0.865-0.989, p < 0.001), and 0.828 (95% CI 0.723-0.933, p < 0.001), respectively (Fig. 2). With a cut-off value of 366.1 pg/mL, the sensitivity and specificity of IL-18 was highest for diagnosis of AOSD (91.7% and 99.1%, respectively). Also, the sensitivity and specificity of S100A8/A9 were 69.4% and 98%, respectively (cut-off value, 4.55 μg/mL) and those of ferritin were 66.7% and 97%, respectively (cut-off value, 237.3 ng/mL).
follistatin-adult-onset Still’s disease and 33 healthy control. The ROC curve values were 0.983 for IL-18 (95% CI 0.961-1.005; p < 0.001), 0.927 for CRP (95% CI 0.865-0.989, p < 0.001), 0.845 for S100A8/A9 (95% CI 0.753-0.937; p < 0.001), 0.828 for ferritin (95% CI 0.723-0.933; p < 0.001), and 0.436 for follistatin-like protein 1 (95% CI 0.299-0.573; p = 0.527).
The comparisons of S100A8/A9, follistatin-like protein 1, and IL-18 levels according to the clinical manifestations of AOSD were evaluated. Serum S100A8/A9 levels were significantly higher in the AOSD patients with fever (p < 0.001), sore throat (p = 0.006), skin rash (p = 0.034), and splenomegaly (p = 0.019) compared to those without (data not shown). Serum IL-18 levels were significantly higher in the AOSD patients with fever (p < 0.001) and sore throat (p = 0.006) (data not shown). However, serum follistatin-like protein 1 levels were not different.
3. Serum S100A8/A9, follistatin-like protein 1, or IL-18 levels and
disease activity in AOSD patients
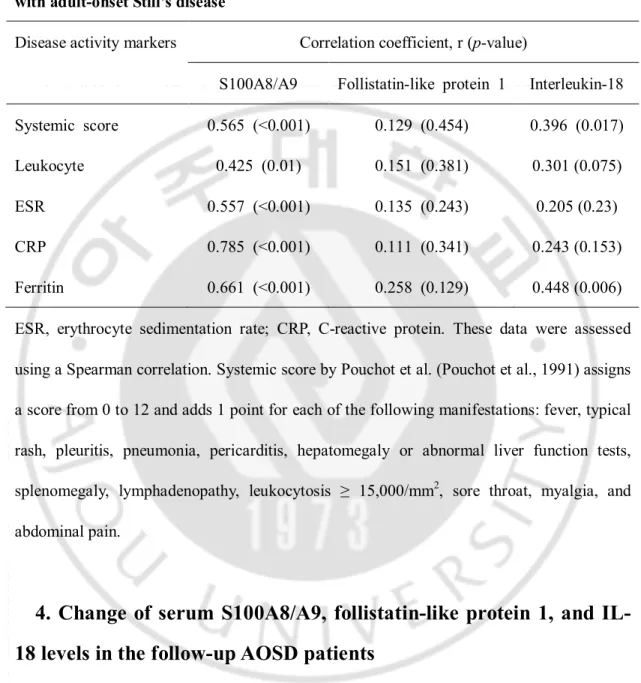
The correlations between preexistent disease activity markers and serum S100A8/A9, follistatin-like protein 1 or IL-18 in AOSD patients are shown in Table 2. Serum S100A8/A9 levels correlated with leukocyte count (r = 0.425, p = 0.01), ESR (r = 0.557, p < 0.001), CRP (r = 0.785, p < 0.001), ferritin (r = 0.661, p < 0.001), and systemic score (r = 0.454, p < 0.001). IL-18 levels correlated only with ferritin (r = 0.448, p = 0.006) and systemic score (r = 0.396, p = 0.017). However, no correlation was found between follistatin-like protein 1 and disease activity markers.
Table 2. Correlation between disease activity markers and systemic score in 36 patients with adult-onset Still’s disease
Disease activity markers Correlation coefficient, r (p-value)
S100A8/A9 Follistatin-like protein 1 Interleukin-18
Systemic score 0.565 (<0.001) 0.129 (0.454) 0.396 (0.017)
Leukocyte 0.425 (0.01) 0.151 (0.381) 0.301 (0.075)
ESR 0.557 (<0.001) 0.135 (0.243) 0.205 (0.23)
CRP 0.785 (<0.001) 0.111 (0.341) 0.243 (0.153)
Ferritin 0.661 (<0.001) 0.258 (0.129) 0.448 (0.006)
ESR, erythrocyte sedimentation rate; CRP, C-reactive protein. These data were assessed using a Spearman correlation. Systemic score by Pouchot et al. (Pouchot et al., 1991) assigns a score from 0 to 12 and adds 1 point for each of the following manifestations: fever, typical rash, pleuritis, pneumonia, pericarditis, hepatomegaly or abnormal liver function tests, splenomegaly, lymphadenopathy, leukocytosis ≥ 15,000/mm2, sore throat, myalgia, and
abdominal pain.
4. Change of serum S100A8/A9, follistatin-like protein 1, and
IL-18 levels in the follow-up AOSD patients
Among AOSD patients with high disease activity before starting corticosteroids or immunosuppressive medications, 16 patients were followed up in the resolution of disease activity with low- to moderate- dose corticosteroids (11.09 ± 10.99 mg/d of prednisolone equivalent) and immunosuppressives such as methotrexate or azathioprine. Follow-up sera
Fig. 3. The levels of S100A8/A9 (A), follistatin-like protein 1 (B), and interleukin-18 (C) in 16 adult-onset Still’s disease (AOSD) according to disease activity. Data are expressed
as the mean ± SD. A Wilcoxon signed-rank test was used to perform the statistical analysis.
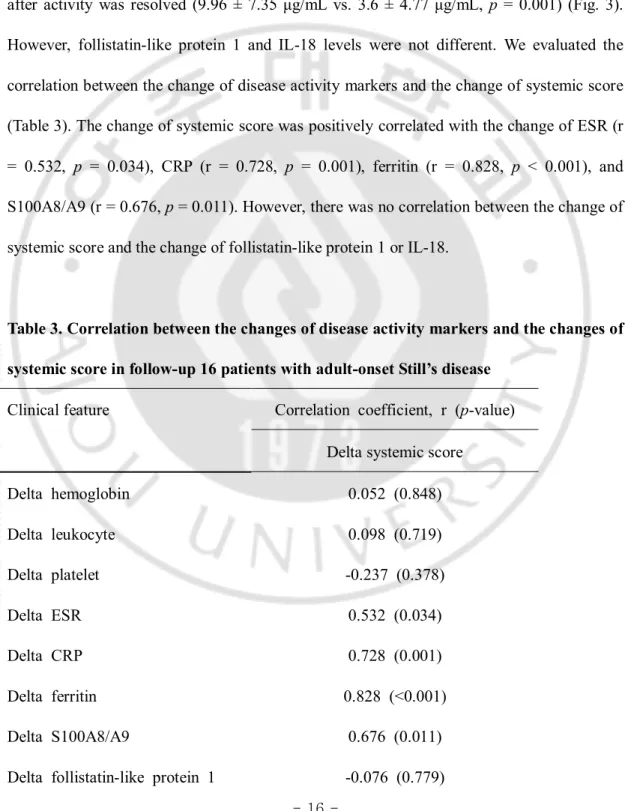
In the AOSD patients who had follow-up, serum S100A8/A9 levels were decreased after activity was resolved (9.96 ± 7.35 μg/mL vs. 3.6 ± 4.77 μg/mL, p = 0.001) (Fig. 3). However, follistatin-like protein 1 and IL-18 levels were not different. We evaluated the correlation between the change of disease activity markers and the change of systemic score (Table 3). The change of systemic score was positively correlated with the change of ESR (r = 0.532, p = 0.034), CRP (r = 0.728, p = 0.001), ferritin (r = 0.828, p < 0.001), and S100A8/A9 (r = 0.676, p = 0.011). However, there was no correlation between the change of systemic score and the change of follistatin-like protein 1 or IL-18.
Table 3. Correlation between the changes of disease activity markers and the changes of systemic score in follow-up 16 patients with adult-onset Still’s disease
Clinical feature Correlation coefficient, r (p-value)
Delta systemic score
Delta hemoglobin 0.052 (0.848) Delta leukocyte 0.098 (0.719) Delta platelet -0.237 (0.378) Delta ESR 0.532 (0.034) Delta CRP 0.728 (0.001) Delta ferritin 0.828 (<0.001) Delta S100A8/A9 0.676 (0.011)
Delta interleukin-18 0.018 (0.948)
ESR, erythrocyte sedimentation rate; CRP, C-reactive protein. These data were assessed using a Spearman correlation. Systemic score by Pouchot et al. (Pouchot et al., 1991) assigns a score from 0 to 12 and adds 1 point for each of the following manifestations: fever, typical rash, pleuritis, pneumonia, pericarditis, hepatomegaly or abnormal liver function tests, splenomegaly, lymphadenopathy, leukocytosis ≥ 15,000/mm2, sore throat, myalgia, and
abdominal pain.
5. Serum IL-1β and TNF-α levels in 20 active AOSD patients and 20
HC
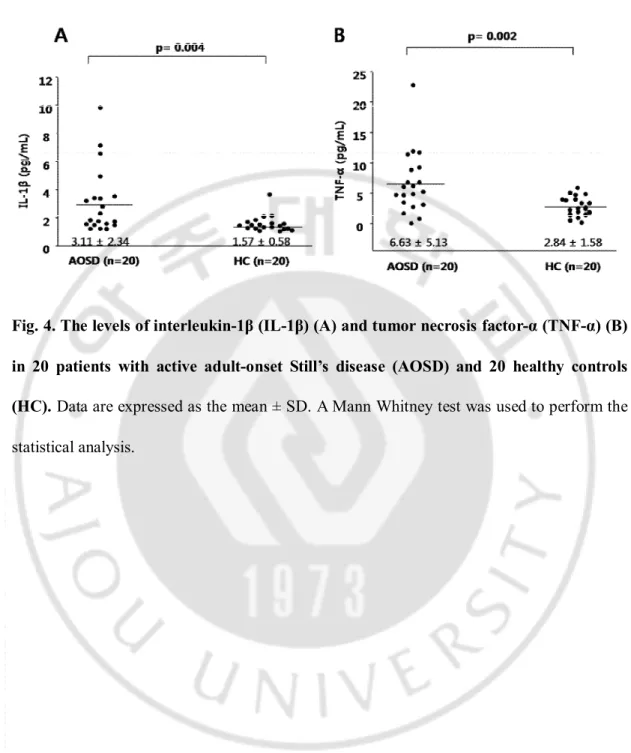
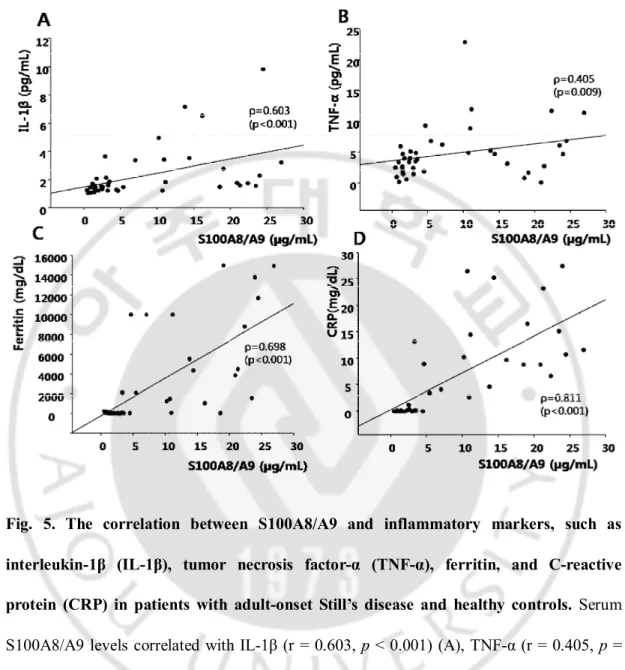
IL-1β and TNF-α levels in 20 active AOSD patients and HC were shown in Fig. 4. The IL-1β levels of AOSD (3.11 ± 2.34 pg/mL) were higher than those of HC (1.57 ± 0.58, p = 0.004), and the TNF-α levels of AOSD (6.63 ± 5.13 pg/mL) were higher than those of HC (2.84 ± 1.58 pg/dL, p=0.002). Serum S100A8/A9 levels correlated with IL-1β (r = 0.603, p < 0.001), TNF-α (r = 0.405, p = 0.009), ferritin (r = 0.698, p < 0.001), and CRP (r = 0.811, p < 0.001) in 20 active AOSD patients and 20 HC (Fig. 5).
Fig. 4. The levels of interleukin-1β (IL-1β) (A) and tumor necrosis factor-α (TNF-α) (B) in 20 patients with active adult-onset Still’s disease (AOSD) and 20 healthy controls (HC). Data are expressed as the mean ± SD. A Mann Whitney test was used to perform the statistical analysis.
Fig. 5. The correlation between S100A8/A9 and inflammatory markers, such as interleukin-1β (IL-1β), tumor necrosis factor-α (TNF-α), ferritin, and C-reactive protein (CRP) in patients with adult-onset Still’s disease and healthy controls. Serum S100A8/A9 levels correlated with IL-1β (r = 0.603, p < 0.001) (A), TNF-α (r = 0.405, p = 0.009) (B), ferritin (r = 0.698, p < 0.001) (C), and CRP (r = 0.811, p < 0.001) (D). These data were assessed using a Spearman correlation.
6. Histopathologic and immunohistochemical characteristics of
skin and lymph node in AOSD
Histopathologic features of skin in AOSD were shown in Table 4 and Fig. 6. The skin biopsies showed mild lymphohistiocytic infiltration in the upper dermis. The
inflammatory cell infiltrates extended into the subcutaneous fat tissue in 4 cases (15.4%). Nuclear debris were found on the dermis in 14 cases (53.8%). Four cases had parakeratosis; however, the degree of this finidng was minimal and negligible. More than half of the cases (n = 14, 53.8%) showed interstitial mucin deposition. A few scattered neutrophils were noted in 7 cases (26.9%), and scattered eosinophils and plasma cells were noted in only 1 case (case 14). Case 12 and 18 showed extravasation of red blood cells. Vasculitis was seen in only 2 cases (7.7%). Epidermal changes, such as an interface dermatitis with basal vacuolization or a few necrotic keratinocytes were in some cases (n = 10; 38.5%).
Five among 8 lymph node biopsy cases showed only paracortical hyperplasia, and 3 cases mixed pattern; paracortical and diffuse (n = 2) or paracortical, follicular and diffuse (n = 1). Vascular proliferation was moderate to severe in all cases, and immunoblast prolfieration was moderate to severe in 5 cases (62.5%).
Table 4. Histopathologic and immunohistochemical staining features of skin in adult-onset Still’s disease.
Case Karyorrhexis Mucin CD4 CD8 CD68 S100A8/A9 IF
1 - + 1 2 1 3 2 + - 1 2 1 2 3 + + 1 2c 2c 3 0 4 + - 1 3 1 2 0 5 - + 1 2 1 1 6 - - 1 2 1 2 0
8 - - 1 2 1 1 0 9 - + 1 3 1 1 0 10 - - 1 2 1 1 11 + + 0 3 1 3 0 12 - - 1b 1b 2 3 0 13 - - 1 2c 2c 3 0 14 + + 1 2 c 2 c 3 15 - - 1 2 1 2 16 + + 1 2d 2d 3 17 - - 1 2 1 1 18 + + 1 3 1 3 19 + + 2 1c 1c 2 20 - + 1 2d 2d 3 21 + + 1b 1b 3 3 22 + - 1b 1 b 2 3 23 + + 2 1 2 3 0 24 + + 1b 1 b 2 3 0 25 - - 1 1 2 2 0 26 + + 2 1 2 3
aThe number of CD4-positive lymphocytes was higher than that of CD8-positive
lymphocytes. bThe number of CD8-positive lymphocytes was higher than that of CD4-positive lymphocytes. c The number of CD68-positive lymphocytes was higher than that of
of CD68-positive lymphocytes. IF, Immunofluorescence.
Fig. 6. Skin biopsy findings in patients with adult-onset Still’s disease. The biopsy of case 24 shows mild perivascular inflammatory cell infiltration (A) with karyorrhexis (B). The biopsy of case 18 shows dermal mucin deposition that caused splayed dermal collagen fibers (C). The biopsy of case 3 shows mild lymphohistiocytic infiltration with karyorrhexis and a few necrotic keratinocytes in the epidermis (D). Immunohistochemial staining for CD4 (E) and CD8 (F) in case 17. The number of CD8-positive lymphocytes is higher than the CD4-positive lymphocytes. (Original magnification, x40 (A), x100 (C, E, F), x200 (B,D)
AOSD were shown in Table 5 and Fig. 7. Five cases showed only paracortical hyperplasia, and 3 cases mixed pattern; paracortical and diffuse (case 4 and 29) or paracortical, follicular and diffuse (case 6). Vascular proliferation was moderate to severe in all cases, and immunoblast prolfieration was moderate to severe in 5 of 8 cases (62.5%). Two cases showed mixed inflammatory cell infitrations with scattered neutrophils or eosinophils. Case 27 had pericapsular endarteritis, and case 29 showed hemophagocytic features with a positive signal for EBER in a few scattered small lymphocytes. Pathologic findings of case 3 and 17 were similar to dermatopathic lymphadenitis (Fig.7A and B), and those of case 4, 27 and 29 were similar to angioimmunoblastic T-cell lymphoma (Fig. 7C and D).
Table 5. Histopathologic and immunohistochemical staining features of lymph node in adult-onset Still’s disease.
Case Patterns of reaction Vascular proliferation Immunoblast proliferation Mimics CD4 CD8 S100A8/A9 3 Paracortical 3 1 DL 2 a 2 a 2 4 Paracortical , diffuse 3 3 AITL 3 1 2 6 Follicular, paracortical , diffuse 3 2 2 a 2 a 2 17 Paracortical 2 2 DL 2 1 2 23 Paracortical 2 3 3 1 3 27 Paracortical 3 3 AITL 2 1 1 28 Paracortical 3 1 2 a 2 a 2 29 Paracortical , diffuse 2 1 AITL 1 3 3
aThe number of CD4-positive lymphocytes was higher than that of CD8-positive
lymphocytes. bThe number of CD8-positive lymphocytes was higher than that of CD4-positive lymphocytes. DL, Dermatopathic lymphadenitis; AITL, Angioimmunoblastic T-cell lymphoma.
Fig.7. Lymph node biopsy findings in patients with adult-onset Still’s disease. The biopsy of case 3 shows nodular expansion of paracortex (A) by pale-staining histiocytes, dendritic cells or Langerhans cells (B). Biopsy of case 4 shows paracortical or diffuse hyperplasia with vascular hyperplasia (C). A residual lymphoid follicle is seen (arrow). The paracortex is composed of large immunoblast and small lymphocyte with occasional eosinophils (D). Immunohistochemical staining for CD4 (E) and CD8 (F) in case 4. The number of CD4-positive lymphoid cells is higher than CD8-positive lymphoid cells. (Original magnification, x40 (A, C), x100 (E, F), x200 (B), x400 (D).
Most of the infiltrating cells were CD68 and CD8-positive on immunohistochemistry of skin biopsies. The percentage and intensity of staining of the positive cells was greater for CD8 than CD68 (57.7%). The number of CD8-positive lymphocytes was higher than the CD4-positive lymphocytes in 23 (88.5%) of 26 cases. Direct immunofluorescence staining was negative in all 11 cases. For S100A8 and S100A9 immunohistochemical evaluations, lymphoid cells in the paracortical zone or germinal center of a reactive lymph node were stained. The antibodies revealed a granular pattern of
cytoplasmic staining. The staining patterns of inflammatory cells in skin biopsies were similar to those of lymphoid cells in a lymph node (Fig. 8). The grade of inflammatory cells expressing S100A8/A9 ranged from 1 to 3. The grading of staining of the positive cells in S100A8/A9 was higher when there were karyrrhexis (p = 0.028), mucin deposition (p = 0.014), and neutrophil infiltration (p = 0.006) (Table 6). Furthermore, the correlation between inflammatory cell grading of CD68 and that of S100A8/A9 was significant shown (p < 0.001) (Table 7).
Fig. 8. S100A8/A9 expression levels in inflammatory cells in skin biopsy of patients with adult-onset Still’s disease (original magnification, ´400). Representative instances of frequent expression (A) and rare expression (B) are shown.
Table 6. The inflammatory cell staining for S100A8 and S100A9 of skin in adult-onset Still’s disease
Pathologic finding and S100A8 and S100A9 staining grade
(+), n (-), n p-value Vacuole N = 6 N = 20 Grade 1 2 4 0.292 Grade 2 2 4 Grade 3 2 12 Karyorrhexis N = 12 N = 14 Grade 1 1 5 0.028 Grade 2 3 4 Grade 3 10 4 Mucin N = 14 N = 11 Grade 1 2 4 0.014 Grade 2 1 5 Grade 3 11 3 Neutrophil infiltration N = 9 N = 17 Grade 1 0 6 0.006
Grade 2 1 5 Grade 3 8 6 Necrosis N = 6 N = 20 Grade 1 2 4 0.794 Grade 2 0 6 Grade 3 4 10
All values are means ± standard deviations.
Table 7. Correlations between inflammatory cell grading of CD4, CD8 and CD68 staining and that of S100A8 and S100A9 staining
S100A8 and S100A9 staining grade
Grade 0 Grade 1 Grade 2 Grade 3 p-value
CD4 N = 12 N = 9 N = 5 N = 0 Grade 1 4 2 0 0.132 Grade 2 3 2 2 Grade 3 5 5 4 CD8 N = 0 N = 6 N = 14 N = 6 Grade 1 1 3 2 0.516
Grade 3 4 7 3 CD68 N = 2 N = 7 N = 14 N = 3 Grade 1 2 3 1 0 <0.001 Grade 2 0 3 3 0 Grade 3 0 11 10 3
Spearman’s correlations were calculated.
The number of CD4-positive lymphocytes was higher than that of CD8-positive lymphocytes in almost all cases (87.5%) of lymph node biopsies. The grade of inflammatory cells expressing S100A8/A9 ranged from 1 to 3 in lymph node biopsies (Fig. 9). The grading of staining of the positive cells in S100A8/A9 was higher when there was severe vascular proliferation (p = 0.05).
Fig. 9. S100A8/A9 expression levels in inflammatory cells in lymph node biopsy of patients with adult-onset Still’s disease (original magnification, ´400). Representative
instances of frequent expression (A) and rare expression (B) are shown.
7. IL-1β secretion after treatment of S100A8/A9 in PBMC from
active AOSD patients and HC
Stimulation of PBMC from 6 AOSD patients and 6 HC in vitro revealed that S100A9 was capable of inducing IL-1β secretion, with levels comparable with those observed using the inflammation stimulus LPS (Fig. 10). Priming of PBMC with IFN-γ prior to stimulation amplified the effects of both S100A9 and LPS in PBMC from 6 HC and 6 AOSD patients.
Fig. 10. Interleukin-1β (IL-1β) secretion after treatment with S100AA9 in peripheral blood monocytes of healthy controls (HC) and patients with adult-onset Still’s disease patient (AOSD). Peripheral blood monocytes (1 x 106/mL) were incubated for 24 hours with
either 10 ng/mL lipopolysaccharide (LPS) or 5 µg/mL S100A9 or left untreated as controls (medium). IL-1β concentrations in supernatants were determined by enzyme-linked
the mean and standard deviations. *p ≤ 0.05 versus controls.
8. Activation of JNK and p38 in a human monocyte cell line after
treatment with S100A9 or S100A8/A9
Western blot analysis was performed with antibodies specific to IκBα and phosphorylated JNK in human monocyte cells treated with S100A9 or LPS for 4 h (Fig. 11A). IκBα was significantly decreased, and JNK were significantly more phosphorylated at 0.5 hr in human monocyte cells treated LPS, but not in those treated S100A9. Therefore, we performed with those treated with S100A8/A9, and confirmed that JNK and p38 were significantly more phosphorylated in S100A8/A9 than S100A9 at 0.5 hr, which was similar to those treated with LPS (Fig. 11B).
Fig. 11. Activation of JNK and p38 in a human monocyte cell line after treatment with S100A9 or S100A8/A9. THP-1 cells were treated with S100A9, S100A8/A9 or lipopolysaccharide (LPS) for the indicated time. Total cellular proteins were extracted for immunoblot analysis. (A) IκBα and phosphorylated JNK in THP-1 cells treated LPS and S100A9. (B) Phosphorylated JNK and p38 in THP-1 cells treated S100A8/9.
PBMC from active AOSD patients and HC
Western blot analysis was performed with antibodies specific to p100, p52, phosphorylated IκBα and JNK in PBMC from HC and AOSD treated with LPS for 2 h (Fig. 12A). IκBα and JNK were significantly more phosphorylated at 0.5 hr in PBMC from HC and AOSD treated with LPS. Western blot analysis was performed with antibodies specific to phosphorylated JNK and p38 in PBMC from HC and AOSD treated with S100A9 or LPS for 4 h (Fig. 12B). JNK and p38 were significantly more phosphorylated at 0.5 hr in PBMC from HC and AOSD treated with S100A9 similar to those treated with LPS (Fig. 12B).
Fig. 12. Activation of JNK and p38 after treatment with S100A9 in peripheral blood mononuclear cells (PBMC) from healthy controls (HC) and patients with active adult-onset Still’s disease (AOSD). PBMC were treated with lipopolysaccharide (LPS) or S100A9 for the indicated time. Total cellular proteins were extracted for immunoblot analysis. (A) p100, p52, phosphorylated IκBα and JNK in PBMC from HC and AOSD treated with LPS. (B) Phosphorylated JNK and p38 in PBMC from HC and AOSD treated with LPS and S100A9.
S100A8/A9 has been known as an endogenous ligand of TLR-4. Western blot analysis performed with antibodies specific to TLR4 in PBMC from 3 active AOSD patients and 3 HC (Fig. 13). TLR4 expressions were increased in AOSD patients compared to HC.
Fig. 13. Toll like receptor 4 (TLR4) expressions in peripheral blood mononuclear cells (PBMC) from healthy controls (HC) and patients with active adult-onset Still’s disease (AOSD). TLR4 expressions were increased in AOSD patients compared to HC.
DISCUSSION
To examine clinical significance of serum S100A8/A9 levels, we measured its levels in AOSD patients and compared them to those of RA patients and HC. Also, we evaluated its levels as a biomarker for disease activity. Serum level of S100A8/A9 of AOSD patients was significantly higher than that of RA patients and HC. Serum levels of S100A8/A9 correlated with leukocyte count, ESR, CRP, ferritin, and systemic score.
Many features of AOSD and systemic JIA seem to be explained by the known effects of proinflammatory cytokines like IL-1, IL-6, macrophage colony-stimulating factor, tumor necrosis factor (TNF)-α, and IL-18. In particular, IL-1, a protein with pleiotropic effects, upregulates its own transcription as well as that of IL-6 (Mellins et al., 2011). IL-1 stimulates the destruction of cartilage and bone; for example, it does so by inducing follistatin-like protein 1, an inflammatory product of joint matrix cells (Wilson et al., 2010; Mellins et al., 2011). In addition, IL-1 activity in systemic JIA is amplified by endogenous factors like S100A8, S100A9, and S100A12 that are themselves produced in excess. This signaling can lead to increased production of proinflammatory cytokines, including IL-1β, which, in turn, further increases production of S100 production (Wittkowski et al., 2008; Frosch et al., 2009). Therefore, in the present study, we evaluated the endogenous factors related to IL-1, such as S100A8/A9, follistatin-like protein 1, and IL-18, with serum of AOSD patients as a disease activity marker.
S100 proteins, which mediate inflammatory responses and are involved in the recruitment of inflammatory cells to sites of injury, have been suggested to form
“damage-proteins form a family with more than 20 members including three that are linked to innate immune functions by their expression by myeloid cells: S100A8, S100A9, and S100A12. Recently, S100A8/A9 has been shown to be the endogenous ligand of Toll-like receptor-4, to play an important role in innate immunity, and to be associated with human sepsis and endotoxemia (Vogl et al., 2007; van Zoelen et al., 2009). This signaling leads to increased production of proinflammatory cytokines such as IL-1β, which, in turn, further increases production of S100 proteins (Mellins et al., 2011). One study showed that serum S100A8/A9 levels were significantly elevated in patients with active systemic JIA compared to those in HC, patients with systemic infections, and patients with leukemia (Frosch et al., 2009). Additionally, S100A8/A9 distinguished systemic onset JIA from infections with a specificity of 95% in contrast to CRP levels. Recently, S100A8/A9 was evaluated as a marker for disease activity in AOSD (Jung et al., 2010). Serum S100A8/A9 was increased in patients with AOSD, in close correlation with disease activity. In the present study, serum S100A8/A9 levels of AOSD patients were significantly higher than RA patients and HC. In addition, serum S100A8/A9 levels showed strong correlations with known disease activity markers such as leukocyte count, ESR, CRP, ferritin, and systemic score. Furthermore, in the follow-up AOSD patients, most patients had significantly decreased S100A8/A9 levels after resolution of disease activity, and the changes of serum S100A8/A9 levels were correlated with the changes of systemic scores. Therefore, these results suggest that serum S100A8/A9 can provide reliable clinical information for monitoring the disease activity and treatment response.
Laboratory markers of active disease in AOSD include ESR, CRP, and ferritin, but these markers do not discriminate AOSD from other inflammatory condition. Also, initial
differential diagnosis of AOSD can be difficult, and it remains a significant clinical challenge to differentiate AOSD from other causes of fever, such as malignancy and infection. In this study, we showed highest sensitivity and specificity of IL-18 for diagnosing AOSD. Also, S100A8/A9 showed strong correlations with known disease activity markers with follow-up samples. However, we didn’t compare these markers from febrile disorders, and had relative small sample size in follow-up samples. Therefore, further study with large sample size would be needed for evaluating specificity of these markers in AOSD patients and treatment response with control groups of febrile disorders.
We showed the correlation between S100A8/A9 and proinflammatory cytokines, such as IL-1β and TNF-α. Moreover, we also confirmed that this marker was immunohistochemically stained in skin and lymph node from AOSD patients. We confirmed that S100A9 was a strong inducer of IL-1β expression in phagocytes of HC and AOSD patients. Furthermore, we showed that S100A9 or S100A8/A9 induced signal transduction pathways, including JNK and p38 in PBMC from HC and AOSD patients or THP-1 cell. We analyzed the expression of S100A8 and S100A9 with skin and lymph node biopsy specimens obtained during the initial phase of AOSD before treatment. S100A8/A9 was expressed in skin and lymph node affected by AOSD; variable percentages of inflammatory cells were positive for S100A8 and S100A9. Such staining was correlated with the numbers of CD68-stained inflammatory cells in skin of AOSD. Furthermore, enhanced S100A8/A9 staining was evident in neutrophil infiltration and inflammatory skin lesions with mucin depositions and karyorrhexis. Although we did not compare inflammatory skin or lymph
expressed at low levels in normal epidermis (Ehrchen et al., 2009). S100A8 and S100A9 are highly expressed in the skin lesions of several inflammatory skin diseases, such as psoriasis, lupus erythematosus and lichen planus (Gabrielsen et al., 1986; Kunz et al., 1992). S100A8/A9 can induce proinflammatory cytokine and chemokine expression as well as proliferation of normal human keratinocytes, and it could represent an important part of positive-feedback mechanism in initiation and amplification of inflammatory skin diseases (Nukui et al., 2008). Furthermore, in psoriasis, epidermal S100A8/A9 overexpression seems to be related with increased serum S100A8/A9 levels, which correlated with disease activity (Benoit et al., 2006). Epidermal overexpression of S100A8/A9 was observed in typical skin rash of systemic JIA, and correlated with the highly increased serum S100A8/A9 levels (Frosch et al., 2003; Frosch et al., 2005). In this study, we showed that S100A8/A9 was expressed in skin and lymph node affected by AOSD, and correlated with neutrophil infiltrations and CD68-stained inflammatory cells. These results could suggest that the infiltrating neutrophil and CD68-positive inflammatory cells are main source cells of S100A8/A9 related inflammation. Furthermore, S100A8/A9 staining was evident in inflammatory cells of skin lesions with mucin depositions and karyorrhexis. Therefore, such results strongly suggest that S100A8/A9 plays an important role in the skin dermal inflammation of AOSD. However, we could not demonstrate the correlation between serum S100A8/A9 levels and S100A8/A9 expression of skin, because we did not have the serum samples of AOSD patients done biopsy.
In addition to clinicopathological implication of S100A8/A9 in AOSD, our data showed the key role of innate immune processes of S100A8/A9 in the pathogenesis of
AOSD. We confirmed that S100A9 was a strong inducer of IL-1β expression in phagocytes of HC and AOSD patients. Furthermore, we showed increased TLR-4 expression in PBMC from AOSD patients compared to HC. These results were consistent previous data (Foell and Roth, 2004; Tsan and Gao, 2007). S100A8/A9 has been known as an endogenous ligand of TLR-4 promoting expression of proinflammatory proteins such as chemokines, cytokines, or signal transduction molecules, similar to LPS (Vogl et al., 2007). S100A8/A9 also induces a thrombogenic, inflammatory response in human microvascular endothelial cells by decreasing the expression of cell junction proteins and molecules and by increasing the transcription of proinflammatory chemokines and adhesion molecules (Viemann et al., 2005). The elevation of S100A8/9, internal TLR-4 ligand, in AOSD may interpret the similarity of inflammatory responses and disease manifestations of AOSD and septic conditions through these molecular basis.
CONCLUSION
We found higher level of S100A8/A9 in the serum of, and upon immunohistochemical staining of pathological skin tissue from, patients with active AOSD. We also found that S100A8/A9 correlated with several inflammatory markers and disease activity markers, and that this DAMP drives IL-1β production. These findings improves our understanding of the role played by S100A8/A9 in immunopathogenesis but also may provide novel diagnostic or therapeutic strategies in AOSD.
REFERENCES
1. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF, Cooper NS, Healey LA,
Kaplan SR, Liang MH, Luthra HS, et al.: The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum 31: 315-324, 1988
2. Benoit S, Toksoy A, Ahlmann M, Schmidt M, Sunderkotter C, Foell D, Pasparakis
M, Roth J, Goebeler M: Elevated serum levels of calcium-binding S100 proteins A8 and A9 reflect disease activity and abnormal differentiation of keratinocytes in psoriasis. Br J Dermatol 155: 62-66, 2006
3. Bywaters EG: Still's disease in the adult. Ann Rheum Dis 30: 121-133, 1971
4. Cagatay Y, Gul A, Cagatay A, Kamali S, Karadeniz A, Inanc M, Ocal L, Aral O, Konice M: Adult-onset Still's disease. Int J Clin Pract 63: 1050-1055, 2009
5. Choi JH, Suh CH, Lee YM, Suh YJ, Lee SK, Kim SS, Nahm DH, Park HS: Serum
cytokine profiles in patients with adult onset Still's disease. J Rheumatol 30: 2422-2427, 2003
6. Clutter SD, Wilson DC, Marinov AD, Hirsch R: Follistatin-like protein 1 promotes
7. Dinarello CA: Interleukin-18, a proinflammatory cytokine. Eur Cytokine Netw 11: 483-486, 2000
8. Edgeworth J, Gorman M, Bennett R, Freemont P, Hogg N: Identification of p8,14 as
a highly abundant heterodimeric calcium binding protein complex of myeloid cells. J Biol Chem 266: 7706-7713, 1991
9. Efthimiou P, Kontzias A, Ward CM, Ogden NS: Adult-onset Still's disease: can recent advances in our understanding of its pathogenesis lead to targeted therapy? Nat Clin Pract Rheumatol 3: 328-335, 2007
10. Ehrchen JM, Sunderkotter C, Foell D, Vogl T, Roth J: The endogenous Toll-like receptor 4 agonist S100A8/S100A9 (calprotectin) as innate amplifier of infection, autoimmunity, and cancer. J Leukoc Biol 86: 557-566, 2009
11. Fautrel B: Adult-onset Still disease. Best Pract Res Clin Rheumatol 22: 773-792, 2008
12. Foell D, Frosch M, Sorg C, Roth J: Phagocyte-specific calcium-binding S100
proteins as clinical laboratory markers of inflammation. Clin Chim Acta 344: 37-51, 2004
Arthritis Rheum 50: 3762-3771, 2004
14. Frosch M, Ahlmann M, Vogl T, Wittkowski H, Wulffraat N, Foell D, Roth J: The myeloid-related proteins 8 and 14 complex, a novel ligand of toll-like receptor 4, and interleukin-1beta form a positive feedback mechanism in systemic-onset juvenile idiopathic arthritis. Arthritis Rheum 60: 883-891, 2009
15. Frosch M, Metze D, Foell D, Vogl T, Sorg C, Sunderkotter C, Roth J: Early activation of cutaneous vessels and epithelial cells is characteristic of acute systemic onset juvenile idiopathic arthritis. Exp Dermatol 14: 259-265, 2005
16. Frosch M, Vogl T, Seeliger S, Wulffraat N, Kuis W, Viemann D, Foell D, Sorg C, Sunderkotter C, Roth J: Expression of myeloid-related proteins 8 and 14 in systemic-onset juvenile rheumatoid arthritis. Arthritis Rheum 48: 2622-2626, 2003
17. Gabrielsen TO, Dale I, Brandtzaeg P, Hoel PS, Fagerhol MK, Larsen TE, Thune PO:
Epidermal and dermal distribution of a myelomonocytic antigen (L1) shared by epithelial cells in various inflammatory skin diseases. J Am Acad Dermatol 15: 173-179, 1986
18. Jung SY, Park YB, Ha YJ, Lee KH, Lee SK: Serum calprotectin as a marker for disease activity and severity in adult-onset Still's disease. J Rheumatol 37:
1029-1034, 2010
19. Kawashima M, Yamamura M, Taniai M, Yamauchi H, Tanimoto T, Kurimoto M,
Miyawaki S, Amano T, Takeuchi T, Makino H: Levels of interleukin-18 and its binding inhibitors in the blood circulation of patients with adult-onset Still's disease. Arthritis Rheum 44: 550-560, 2001
20. Kunz M, Roth J, Sorg C, Kolde G: Epidermal expression of the calcium binding surface antigen 27E10 in inflammatory skin diseases. Arch Dermatol Res 284: 386-390, 1992
21. Lotito AP, Campa A, Silva CA, Kiss MH, Mello SB: Interleukin 18 as a marker of
disease activity and severity in patients with juvenile idiopathic arthritis. J Rheumatol 34: 823-830, 2007
22. Mellins ED, Macaubas C, Grom AA: Pathogenesis of systemic juvenile idiopathic arthritis: some answers, more questions. Nat Rev Rheumatol 7: 416-426, 2011
23. Miyamae T, Marinov AD, Sowders D, Wilson DC, Devlin J, Boudreau R, Robbins P,
Hirsch R: Follistatin-like protein-1 is a novel proinflammatory molecule. J Immunol 177: 4758-4762, 2006
S100A8/A9, a key mediator for positive feedback growth stimulation of normal human keratinocytes. J Cell Biochem 104: 453-464, 2008
25. Ohta A, Yamaguchi M, Kaneoka H, Nagayoshi T, Hiida M: Adult Still's disease: review of 228 cases from the literature. J Rheumatol 14: 1139-1146, 1987
26. Pouchot J, Sampalis JS, Beaudet F, Carette S, Decary F, Salusinsky-Sternbach M, Hill RO, Gutkowski A, Harth M, Myhal D, et al.: Adult Still's disease: manifestations, disease course, and outcome in 62 patients. Medicine (Baltimore) 70: 118-136, 1991
27. Raquil MA, Anceriz N, Rouleau P, Tessier PA: Blockade of antimicrobial proteins S100A8 and S100A9 inhibits phagocyte migration to the alveoli in streptococcal pneumonia. J Immunol 180: 3366-3374, 2008
28. Roth J, Vogl T, Sorg C, Sunderkotter C: Phagocyte-specific S100 proteins: a novel
group of proinflammatory molecules. Trends Immunol 24: 155-158, 2003
29. Shibanuma M, Mashimo J, Mita A, Kuroki T, Nose K: Cloning from a mouse
osteoblastic cell line of a set of transforming-growth-factor-beta 1-regulated genes, one of which seems to encode a follistatin-related polypeptide. Eur J Biochem 217: 13-19, 1993
30. Striz I, Wang YM, Svarcova I, Trnka L, Sorg C, Costabel U: The phenotype of alveolar macrophages and its correlation with immune cells in bronchoalveolar lavage. Eur Respir J 6: 1287-1294, 1993
31. Tanaka M, Ozaki S, Osakada F, Mori K, Okubo M, Nakao K: Cloning of
follistatin-related protein as a novel autoantigen in systemic rheumatic diseases. Int Immunol 10: 1305-1314, 1998
32. Thornton S, Sowders D, Aronow B, Witte DP, Brunner HI, Giannini EH, Hirsch R:
DNA microarray analysis reveals novel gene expression profiles in collagen-induced arthritis. Clin Immunol 105: 155-168, 2002
33. Tsan MF, Gao B: Pathogen-associated molecular pattern contamination as putative endogenous ligands of Toll-like receptors. J Endotoxin Res 13: 6-14, 2007
34. Ushio S, Namba M, Okura T, Hattori K, Nukada Y, Akita K, Tanabe F, Konishi K,
Micallef M, Fujii M, Torigoe K, Tanimoto T, Fukuda S, Ikeda M, Okamura H, Kurimoto M: Cloning of the cDNA for human IFN-gamma-inducing factor, expression in Escherichia coli, and studies on the biologic activities of the protein. J Immunol 156: 4274-4279, 1996
Wittebole X, Laterre PF, Boermeester MA, Roth J, van der Poll T: Expression and role of myeloid-related protein-14 in clinical and experimental sepsis. Am J Respir Crit Care Med 180: 1098-1106, 2009
36. Viemann D, Strey A, Janning A, Jurk K, Klimmek K, Vogl T, Hirono K, Ichida F, Foell D, Kehrel B, Gerke V, Sorg C, Roth J: Myeloid-related proteins 8 and 14 induce a specific inflammatory response in human microvascular endothelial cells. Blood 105: 2955-2962, 2005
37. Vogl T, Ludwig S, Goebeler M, Strey A, Thorey IS, Reichelt R, Foell D, Gerke V,
Manitz MP, Nacken W, Werner S, Sorg C, Roth J: MRP8 and MRP14 control microtubule reorganization during transendothelial migration of phagocytes. Blood 104: 4260-4268, 2004
38. Vogl T, Tenbrock K, Ludwig S, Leukert N, Ehrhardt C, van Zoelen MA, Nacken W,
Foell D, van der Poll T, Sorg C, Roth J: Mrp8 and Mrp14 are endogenous activators of Toll-like receptor 4, promoting lethal, endotoxin-induced shock. Nat Med 13: 1042-1049, 2007
39. Wilson DC, Marinov AD, Blair HC, Bushnell DS, Thompson SD, Chaly Y, Hirsch
represent a biomarker for systemic-onset juvenile rheumatoid arthritis. Arthritis Rheum 62: 2510-2516, 2010
40. Wittkowski H, Frosch M, Wulffraat N, Goldbach-Mansky R, Kallinich T,
Kuemmerle-Deschner J, Fruhwald MC, Dassmann S, Pham TH, Roth J, Foell D: S100A12 is a novel molecular marker differentiating systemic-onset juvenile idiopathic arthritis from other causes of fever of unknown origin. Arthritis Rheum 58: 3924-3931, 2008
41. Yamaguchi M, Ohta A, Tsunematsu T, Kasukawa R, Mizushima Y, Kashiwagi H,
Kashiwazaki S, Tanimoto K, Matsumoto Y, Ota T, et al.: Preliminary criteria for classification of adult Still's disease. J Rheumatol 19: 424-430, 1992
- 국문요약 -
성인형스틸씨병에서 TLR4 내인리간드 S1008/A9의
질병활성화 표지자로서 역할 및 임상 양상과의 관련성
서론: 성인형스틸씨병과 소아특발성관절염 환자에서 질병활성화를 예측 할 수 있는 표지자로 S100A8/A9, follistatin 유사단백 1 및 인터루킨 18(IL-18)에 대한 보고가 있다. 그러나, 과거의 보고는 결과가 다양하고 소수의 환자를 대상으로 하였다는 한계점이 있다. 이에 성인형스틸씨병 환자를 대상으로 S100 A8/A9, follistatin 유사단백 1, IL-18을 측정하여 질환의 진단 마커 또는 질병 활성화 표지자로서의 유용성을 알아 보고자 하였다. 또한 이중 질병활성화 표지 자로 확인된 S100A8/A9을 성인형스틸씨병의 침범 장기인 피부와 림프절에 염 색하고, 환자의 말초혈액단핵세포를 가지고 S100A8/A9과 IL-1β와의 연관성 을 확인해보고자 하였다. 방법: 36명의 성인형스틸씨병 환자 및 40명의 류마티스관절염 환자, 정 상인 33명에서 혈청을 수집하였다. 16명의 성인형스틸씨병 환자에서 질병 활성 화가 회복된 후 한번 더 혈청을 수집하였다. 혈청에서 S100A8/A9, follistatin 유사단백 1, IL-18을 효소면역측정법을 이용하여 측정하였다. 또한 성인형스틸 씨병 환자의 임상 및 검사 지표를 확인하였다. 성인형스틸씨병 환자 6명, 정상인 6명에서 말초혈액단핵세포를 수집하였다. 또한 진단을 위해 시행하였던 성인형 스틸씨병 환자 26명의 피부 조직, 8명의 림프절 조직을 이용하여 S100A8/A9 염색하였다.
결과: 성인형스틸씨병 환자의 S100A8/A9 (11.77 ± 8.84 µg/mL)은 류마티스관절염 환자(3.53 ± 3.43 µg/mL, p<0.001) 및 정상인 (2.49 ± 1.8 3 µg/mL, p<0.001)에 비해 유의하게 증가되었으나, 성인형스틸씨병 환자의 foll istatin 유사단백 1은 류마티스관절염 환자와 정상인과 차이가 없었다. 성인형 스틸씨병 환자의 IL-18 (7560.3 ± 7577.6 pg/mL)은 류마티스관절염 환자(2 17.7 ± 292.1 pg/mL, p<0.001) 및 정상인(139.2 ± 86.2 pg/mL, p<0.001) 에 비해 유의하게 증가되었다. 성인형스틸씨병 환자의 혈청 S100A8/A9은 백혈 구 수, 적혈구침강속도, C-반응단백, 페리틴, 전신 활성도 수치와 유의한 양의 상관관계를 보였으며, 성인형스틸씨병 환자에서 질병 활성이 회복된 후S100A8/ A9은 유의하게 감소하였다. 또한, S100A8/A9이 IL-1β 와 종양괴사인자α와 유의한 상관관계를 보였다. 성인형스틸씨병의 피부 및 림프절 조직에서 S100A8/A9이 다양한 강도로 염색되는 것을 확인할 수 있었고, 특히 피부조직 에서 핵파괴나 점액질 침착, 중성구 침범이 있을 때 S100A8/A9의 염색 강도가 높은 것을 확인할 수 있었다. 성인형스틸씨병 환자 6명, 정상인 6명의 말초혈액 단핵세포에 S100A8/A9을 처리하였을 때 유의하게 IL-1β의 분비가 상승한 것 을 확인할 수 있었고, JNK, p38와 같은 전사인자가 활성화 되는 것을 확인하였 다. 결론: 이 결과로 성인형스틸씨병 환자에서 질병활성도 표지자로서 S100 A8/A9이 유용함을 확인할 수 있었다. 또한 성인형스틸씨병에서 S100A8/A9이 피부 조직 및 림프절에 발현하여 질병의 증상에 관여할 것으로 추측되며 중요 사이토카인인 IL-1β의 발현 조절에 작용할 것으로 추측된다.