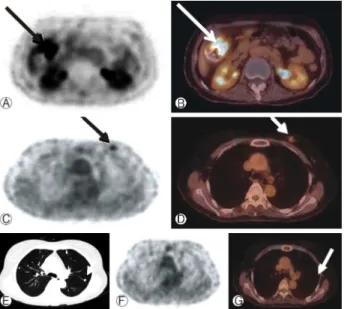
Pulmonary epithelioid hemangioendothelioma misconceived as pulmonary metastasis of other malignancies
4
0
0
전체 글
(2)
(3)
(4)
수치
관련 문서
Often models uncertainty about specific pa- rameters is reflected as uncertainty in specific entries of the state space matrices A, B, C, D.. Let p = (p 1 , ..., p n )
In the change of physical strength, The exercise group showed statistically significant differences in muscle strength(right), muscle strength(left),
As a result of performing a compound exercise of spinning and Zumba for 8 weeks, the change in α-amylase showed a significant difference in the exercise group (p<.01), and
A) Clinical view of the recession defects B) Tunnel preparation with VISTA C) Deepithelialization using a high-speed handpiece at the hard palate. D)
There was no significant difference between the groups in problems of eating habits, but the obesity group considered overeating as a problem while the normal
Pilot Confirm runway 09 left for landing. ATC gives you further instructions to turn right heading 310. On the radar display, there was an area to avoid which requires a
In the lower extremity balance, the change in left unilateral clerk showed a statistically significant difference as the exercise group increased post-test
In the change of active oxygen, As a result of the active oxygen change between the two groups, there was a statistically significant difference according
